Use of gastroscopy in the management of pediatric toxic ingestions: insights from a decade of experience – a retrospective study
Marco Marano, Lavinia Di Meglio, Mara Pisani, Bianca Maria Goffredo, Carla Olita, Simona Faraci, Francesca Rea, Salvatore Perdichizzi, Giorgio Zampini, Piero David, Filippo Torroni

TL;DR
This study shows that gastroscopy can effectively remove toxic substances from the stomachs of children in specific poisoning cases.
Contribution
The study provides evidence for the safe and effective use of EGD in pediatric gastrointestinal decontamination.
Findings
EGD successfully removed xenobiotic residues in 15 out of 19 cases.
No complications were reported in any of the patients who underwent EGD.
EGD is particularly useful for sustained-release formulations and delayed gastric emptying.
Abstract
Pediatric poisonings account for a significant proportion of poison center consultations. Gastrointestinal decontamination (GD) is a crucial intervention in cases of acute poisoning, yet its effectiveness remains debated. This study aims to evaluate the role of esophagogastroduodenoscopy (EGD) in pediatric GD by retrospectively analyzing cases of suspected or confirmed toxic ingestions in which EGD was employed as a decontamination technique. A retrospective review was conducted on medical records from our hospital between 1 January 2015, and 31 March 2025. Pediatric patients (<18 years) who underwent EGD for GD following suspected or confirmed ingestion of toxic drugs were included. A total of 19 cases met the inclusion criteria. In all cases, a potentially toxic drug dose was ingested. EGD was primarily indicated in the presence of sustained-release (SR) formulations, delayed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
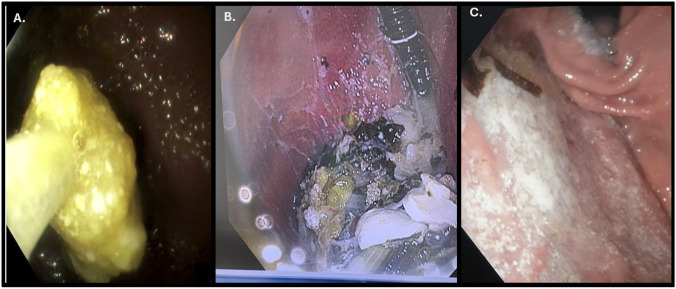 FIGURE 1
FIGURE 1| GD techniques | Procedure | Indication | Contraindication |
|---|---|---|---|
| GL | Position of a Levin probe (32–36 French in adults, 22–28 French in children) and the infusion and aspiration of large volumes of water (almost 2 L) | Within 1 hour from ingestion with trained medical operators | >1 h from ingestion for lack of benefit |
| AC | Charcoal is obtained by controlled pyrolysis of coconut shells, peat, lignite, wood, or petroleum, the activation comes form heating in steam, air, or carbon dioxide at 600 °C–900 °C. This process creates a surface area of 950 to 2,000 m2/g | Within 1 hour from ingestion of drugs absorbed by AC, however, for slow releaser AC can be used up to 4 h | Drugs not absorbed by AC. >1 h from ingestion or 4 h in case of slow releaser |
| WBI | Enteral administration of an osmotically balanced polyethylene glycol-electrolyte solution to enhance bowel emptying and to reduce the drug absorption | Potentially toxic ingestions of sustained-release or enteric-coated drug, drugs not adsorbed by AC (e.g., lithium, potassium, and iron), and for removal of illicit drugs in body “packers” or “stuffers | Severe abdominal distension, vomiting |
| Ipecac syrup | Oral ingestion of ipecac syrup which contains emetine and cephaeline that induce emesis by local gastric irritation and by the stimulation of the emesis chemo-trigger zone | No indicated according to the last AACT and EAPCCT position statement | |
| EGD | Use of an endoscope adapted to the patient’s characteristics | Bezoars | Unprotected airways |
| n | Age/Sex | Drugs (plasmatic level) | Toxic dose | Clinical condition and exams | PSS | Hours before EGD | EGD |
|---|---|---|---|---|---|---|---|
| 01 | 15 years/F | lithium sulfate SR 2490 mg (3.37 mmol/L) | >2.5 mmol/ | drowsiness, confusion metabolic acidosis, >AST, ALT |
| 17 | negative |
| 02 | 15 years/F | -isoniazid 30gr (93.45 μg/mL) | −40 mg/kg | vomit, coma, convulsions, metabolic acidosis, > AST, ALT and CPK | 3 | 12 | bezoar |
| 03 | 16 years/M | eltrombopag 4200 mg (188 mcg/mL) | Unknown | drowsiness and confusion, esophagus erosion | 2 | 2.5 | tablet residual |
| 04 | 14 years/F | quetiapine SR 1400 mg (unknown) | >10 mg/kg | drowsiness and confusion | 2 | 3 | Gastric material with residual tablets |
| 05 | 17 years/F | -biperiden 160 mg (unknown) | -unknown | drowsiness and confusion | 2 | 2 | tablet residual |
| 06 | 17 years/F | Aripiprazole 125 mg (unknown) | 90 mg | >CPK | 1 | 3 | tablet residual |
| 07 | 13 years/M | lithium sulfate SR | >2.5 mmol/L | Vomit, extreme agitation |
| 11 | Gastric material with residual tablets |
| 08 | 13 years/F | acetylsalicylic acid | 150 mg/kg | none | 0 | 4 | bezoar |
| 09 | 14 years/F | -quetiapine SR uncertain mg (1784 ng/mL) | ->10 mg/kg | coma and hypotension | 3 | 4 | bezoar |
| 10 | 16 years/M | caffeine 14000 mg (53 mcg/mL) | −50–200 mg/kg | vomiting, metabolic acidosis, AKI and >CPK | 3 | 5 | negative |
| 11 | 17 years/F | -amitriptyline 112.5 mg (unknown) | ->5 mg/kg | drowsiness and confusion, ileus, bradycardia | 3 | 6 | tablet residual |
| 12 | 17 years/F | lithium sulfate SR 2905 mg (2.96 mmol/L) | >2.5 mmol/L | >AST, ALT | 1 | 6 | bezoar |
| 13 | 11 years/F/104 kg | -repaglinide 15 g (unknown) | -4 mg | none | 1 | 3 | Gastric material with residual tablets |
| 14 | 16 years/F/93 kg | -clozapina 1900 mg (unkown) | ->62.5 mg | confusion | 2 | 3 | Gastric material with residual tablets |
| 15 | 13y F/43 kg | -sertraline 1,500 mg (unkown) | ->2 gr | lethargy | 2 | 2 | bezoar |
| 16 | 16y F/56 kg | Aripiprazole 1000 mg (791.10 ng/mL) | 90 mg | Confusion mild metabolic acidosis | 1 | 10 | negative |
| 17 | 15y F/70 kg | Carbamazepine 6500 mg (27.6 mcg/mL) |
| Coma | 3 | 28 | negative |
| 18 | 17y F/50 kg | -lurasidone 814 mg (unkown) |
| Sinus bradycardia drowsiness and confusion | 2 | >12 h | bezoar |
| 19 | 17y M/ 64 kg | -Lithium sulfate SR 2407 mg (1.08 mmol/L) | >2.5 mmol/L | >AST, ALT | 1 | 6 | tablet residual |
| Ref. | Sex/Age | Drugs | PSS | Other GD | Hours before EGD | EGD/abdomen RX or TC | Outcome |
|---|---|---|---|---|---|---|---|
|
| 40/F | Quetiapine 18 g | 3 | |
| Bezoar | favorable |
|
| 41/M/ | Quetiapine 15gr | 3 | | 13 h | Bezoar | favorable |
|
| 28/M | Quetiapine 24gr | 2 | | 2.5 h | Bezoar | favorable |
|
| 22/M | Quetiapine 15 g | 2 | | 7.5 h | Bezoar | favorable |
|
| 48/M | Quetiapine 15gr | 3 | | >2 h | Bezoar | favorable |
|
| 28/M | Quetiapine 6gr | 3 | | 2.5 h | Bezoar | favorable |
|
| 26/F | Quetiapina Mirtazapine | 3 | |
| Bezoar | favorable |
|
| 26/F | Quetiapina 3gr | 3 | | 3–7 h | tables and food residuals | favorable |
|
| 38/M | Quetiapine 11.8gr | 3 | | 2 h | Bezoar | favorable |
|
| 64/F | Quetiapine | 3 | | >24 h | residual tablets/negative | favorable |
|
| 42/F | KCl 1,000 mEq SR clonazepam 50 mg | 2 | AC/GL | 2–4 h | solid tablets/radiopaque image | favorable |
|
| 49/M | Vegetamine A | 3 | AC | >72 h | Bezoar/ radiopaque image | favorable |
|
| 43/M | Methadone | 3 | AC/WBI | >24 h | Bezoar/radiopaque image | favorable |
|
| 17/M | Diphenhydramine | 3 | AC/ WBI | >24 | Bezoar partially removed/radiopaque image | favorable |
|
| 37/F | lamotrigine 2.6gr Clomipramine SR 4.2 gr | 3 | | 20 h | Bezoar/ radiopaque image | favorable |
|
| 14/M | Fluoxetine | 3 | WBI | 4 h | Solid tablets | favorable |
|
| 44/F | KCl SR 600 mEq | 3 | WBI | 6 h | Bezoar/radiopaque image | favorable |
|
| 28/F | Clomipramine SR 4.5gr | 0 | AC/ GL | 4 h | Bezoar/radiopaque image | favorable |
|
| 25/F | Clomipramine SR 6gr | 3 | | 5.5 h | Bezoar in the esophagus | favorable |
|
| 13/F | diphenhydramine | 3 | | 38 h | Bezoar/ radiopaque image | favorable |
|
| 53/M | Paroxetine SR | 3 | | >10 h | bezoar with partial removal complicated by esophageal | death for MOF and ARDS |
|
| F/64y | Salicylate | 3 | AC | >120 h | packet/paper wrapped and bezoar/negative RX and TC | death for AKI and MOF |
|
| 47/F | Venlafaxine SR 15 gr | 3 | | >120 h | bezoar | persistent come |
|
| 18/F | Theophylline SR18 gr | 3 | GL | 12H | bezoar | favorable |
|
| 16/ F | Bupropion Aripiprazole | 3 | AC | 18 h | bezoar | favorable |
|
| 40/F | Clomipramine | 3 | AC | Unknown | Bezoar/radiopaque image | favorable |
|
| 61/F | Venlafaxine SR Nifedipine Atorvastatin | 3 | AC | Unknown | Bezoar/ oral contrast under fluoroscopy and a cystic-appearing mass | death for MOF |
|
| 55/F | KCl 93 gr | 3 | | 6 | Tablets/radiopaque image | favorable |
|
| 55/F | KCl 120gr | 3 | GL | 12 | Tablets/radiopaque image | favorable |
|
| 23 F | KCl 120 gr | 3 | WBI | 4 | Tablets/radiopaque image | favorable |
|
| 23F | KCl 36gr | 3 | | Unknown | Tablets/radiopaque image | favorable |
|
| 35/F | Amitriptyline 1.45gr | 3 | AC | 2 | Tablets | favorable |
| Radiopaque | Bezoar |
|---|---|
|
|
|
| Vegetamine A | Vegetamine A |
| Methadone |
|
| clomipramine SR | Diphenhydramine |
| Diphenhydramine | Clomipramine SR |
| Salicylate | |
| Venlafaxine SR | |
| Theophylline SR | |
|
| |
| Aripiprazole SR |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoisoning and overdose treatments · Foreign Body Medical Cases · Methemoglobinemia and Tumor Lysis Syndrome
Introduction
Background
Pediatric exposures account for nearly 56% of human exposure calls to U.S. poison centers, according to the latest 2023 data. Among these, 39.8% involve children under the age of five. While pediatric poisonings are primarily unintentional—often resulting from general accidental exposures, therapeutic errors, or unintentional misuse—intentional exposures become the leading cause among adolescents (ages 13–19) and adults (Gummin et al., 2024).
Gastrointestinal decontamination (GD) plays a critical role in managing poisoned patients. Recent U.S. data from 2023 indicate that 78.23% of human exposures occur via the gastrointestinal (GI) route, underscoring the importance of GD in acute poisoning management (Gummin et al., 2024; Albertson et al., 2011; Ornillo and Harbord, 2020).
The most commonly used GD techniques include gastric lavage (GL), activated charcoal (AC), cathartics, whole bowel irrigation (WBI), induced emesis, esophagogastroduodenoscopy (EGD) in selected cases, and combined approaches (Table 1) (Gosselin et al., 2025; Smith, 2010). However, the utility of these techniques remains controversial in the literature, particularly following the most recent position statements. Their effectiveness is often supported only by small studies and lacks robust evidence-based validation (American Academy of Clinical Toxicology and European Association of Poisons Centres and Clinical Toxicologists, 2005; Benson et al., 2024; Höjer et al., 2013; Thanacoody et al., 2015; Park et al., 2018; Hoegberg et al., 2021; Sandilands, 2023). In clinical practice, there is still no clear consensus, and adherence to existing guidelines remains low. Moreover, the use of these techniques has declined over the past decade. According to the 2023 Annual Report, AC was used in only 0.42% of pediatric exposures, while ipecac syrup and GL were not used at all, and WBI was used in only 0.01% of cases (Gummin et al., 2024).
Conducted an international, multicenter, cross-sectional prospective study analyzing the use of GD in children under 18 years of age with toxic exposures. The study assessed the appropriateness of these interventions and found that GD procedures were deemed inappropriate in more than 50% of cases (Mintegi et al., 2017).
Over the past decade, several case reports have described the use of EGD as a GD technique in the management of severe or refractory poisonings, particularly those involving sustained-release (SR) formulations or drugs with a tendency to form bezoars (Gosselin et al., 2025). In this retrospective study, we analyzed all pediatric cases of suspected or confirmed toxic drug ingestion managed at our hospital—with the support of our dedicated pediatric poison control center—in which EGD was used as a decontamination technique.
Methods
Ethics
This study was conducted in accordance with the Helsinki Declaration (Fortaleza revision, 2013), Good Clinical Practice Standards (CPMP/ICH/135/95), and the current Decree-Law 196/2003 regarding personal data protection, as well as all applicable European regulations on this subject. This study was approved by the Ethics Committee of Bambino Gesù Pediatric Hospital code. n. 3648/2025 and date of approval 11/07/2025. Informed consents were collected in all patients.
Study design, setting and selection of participants
We retrospectively analyzed all medical records from the past 10 years, covering the period from 1 January 2015, to 31 March 2025. We selected all pediatric patients with suspected or confirmed ingestion of a toxic drug dose who were treated at our hospital. The inclusion criteria were:
- Confirmed or suspected ingestion of a potentially toxic drug dose.
- Age <18 years.
- Undergoing EGD as a decontamination technique.
The exclusion criterion was:
- Age >18 years.
Interventions and measurements
The indication for EGD at our center was based on multiple factors:
- -Factors related to the drug: ingestion of medications at toxic doses with potential for significant harm, ingestion of sustained-release formulations, or drugs known to delay gastric emptying or reduce gastrointestinal motility due to anticholinergic activity.
- -Factors related to the patient: the clinical condition of the patient and the anticipated severity of toxicity.
- -Factors related to previous experience: previous experience at our institution and evidence reported in the literature.
For each patient, we collected data on the following variables: age, ingested drug (s) and dosage (if known), time between ingestion and arrival at the emergency unit (EU), other GI decontamintion techniques performed, Poisoning Severity Score (PSS), clinical and laboratory abnormalities, indication for EGD, time between ingestion and EGD, EGD findings, complications of the procedure, serum drug levels (if available), and clinical outcomes. The dosage assumed and the serum drug level were considered toxic using the values proposed by Micromedex. EGD was performed by expert pediatric endoscopists under general anaesthesia with advanced airway control. The procedure was conducted either in the operating room or the pediatric intensive care unit (PICU), using an appropriate endoscopic tool (Olympus GIF H 190–185 Tokyo, Japan). The procedures included gastric irrigation with saline solution 0.9%, accurate removal of gastric material using a specific device (retrieval devis Boston Scientific) and aspiration. Informed consent was obtained from all patients’ legal guardians before the procedure. Following gastroscopy, all patients underwent continuous 24-h monitoring.
Outcome
All analyzed variables were collected and organized into a comprehensive table. For each patient, we assessed the ingested dose, the time interval between ingestion and endoscopy, available blood levels, endoscopic findings, final clinical outcome, and any adverse effects or complications related to the procedure.
Data collection and analysis
Two authors (LDM, MM) reviewed all clinical records and extracted the data.
Results
The results are presented in Table 2. We analyzed all the medical records of the last decade and 19 cases met the inclusion criteria.
In all cases, a potentially toxic dose of the drug was ingested. In cases 01, 02, 03, 05, 07, 09, 11, 13, 14, 15, 18, 19 the drug was part of the patient’s home therapy and was ingested in all cases with suicidal intent. GL was performed before EGD in all cases except 11, 13, 17, and 18. AC was administered before EGD in cases 02, 03,04, 05, and 10, and after EGD in cases 11, 15.
The indication for EGD was based on multiple factors, including:
- Certain or reported ingestions of medications at toxic doses that could potentially cause harm (01–19).
- The ingestion of sustained-release (SR) formulations (01, 04, 05, 07, 09, 12, 18, 19).
- Drugs known to delay gastric emptying or reduce GI motility due to their anticholinergic activity (06, 09, 11, 14, 15, 18, 19).
- The clinical condition of the patient and the potential toxicity (01–19).
- Previous experience from our hospital or present in literature (01, 04–07, 09, 11, 12, 14–16, 18, 19).
In cases where bezoars (defined as aggregates of inedible or undigested material), solid tablets, or food material were present, complete aspiration and removal of the xenobiotic were successfully performed.
EGD findings were negative in cases 01, 10, 16, and 17. Pharmacobezoars were observed in cases 02, 08, 09, 12, 15, and 18. Additionally, in cases 02 and 18, residuals in their reticular phase were also reported. Single tablets not forming bezoars were identified in cases 03, 05, 06, 11, 19; while gastric material with residual drug content was found in cases 04, 07, 13, and 14 (Figure 1).
(A). Bezoar; (B) Gastric material with residual tablets; (C) tablet residual.
Drug’s blood levels were obtained in all cases except for 04, 06, 11, 14, and 15. However, these results were only available after the procedure and were not useful in the initial management. Nevertheless, in all the performed cases, elevated drug levels were confirmed apart form case 05, 17, 18, and 19. The levels were monitored, and in all cases, a reduction and, eventually, an absent concentration were observed.
All patients were intubated for the procedure and extubated afterward, except for Patient 09, 10, and 17. Patient 9 was extubated after 48 h due to a comatose state and hemodynamic instability; a 72 h monitoring in PICU was needed. Patient 10 required continuous veno-venous hemodiafiltration (CVVHDF), was extubated after 24 h and needed a 48 monitoring in PICU. Patient 17 required intubation initially for a coma and after for respiratory failure due to a ventilator associated pneumonia and was extubated after 14 days. Additionally, the patient required CVVHDF and was assisted in PICU for 2 weeks.
Patients 01 were admitted to the PICU for the first 48 h and required additional treatments, including CVVHDF. Patients 02, 07, and 16 required 72 h of monitoring in the PICU. Patient 02 received pyridoxine and N-acetylcysteine due to elevated creatine phosphokinase (CPK) and transaminase levels.
Patients 03 and 12 were admitted to the Intensive Short-Term Observation Unit of the ED for 24 h for continued monitoring. Meanwhile, Patients 06, 11, 13, 14, 15, 18, and 19 were admitted to the PICU for 24 h.
Patients 05 and 08 were monitored in the pediatric department for the first 48 h.
Patient 4 was admitted directly in the Neuropsychiatry Unit (NP).
Following their initial admissions to either the pediatric unit or the PICU, all patients were subsequently transferred to the NP unit. The median length of stay in the NP unit was 6 days (range: 3–60 days).
The outcome was favorable for all patients, they were discharged home in good clinical condition. No adverse events were reported following the procedure.
Discussion
The GI tract plays a fundamental role in drug absorption. The toxicokinetics and toxicodynamics of a xenobiotic—such as its anticholinergic properties, SR formulation, or propensity to form bezoars—along with individual patient factors (e.g., co-administration of other substances, anatomical variations, and time since last meal), determine the location and timing of absorption within the GI tract (Miyauchi et al., 2015).
In the stomach, xenobiotics progress through three phases: the tablet/food phase, the soluble/fluid phase, and the reticular/empty phase, each corresponding to a distinct stage of digestion (Miyauchi et al., 2015). Until absorption occurs, drugs technically remain outside the systemic circulation and thus cannot exert toxic effects (Nelson, 2000). The primary objective of gastrointestinal decontamination is to remove the xenobiotic as promptly as possible to prevent systemic absorption. As shown in Table 1, the effectiveness of techniques such as AC and GL is highly time-dependent. In practice, however, patients rarely present to the hospital within 1 hour of ingestion, and routine steps—including medical history collection, physical examination, and poison center consultation—inevitably delay intervention (Albertson et al., 2011; Ornillo and Harbord, 2020; Gosselin et al., 2025).
Although EGD is not currently included in standard guidelines for managing toxic ingestions, its use as a decontamination method was first proposed in 1986 (Gosselin et al., 2025). Initial supporting evidence stems from observational studies. For instance, Miyauchi et al. evaluated endoscopic findings after GL and found no clear correlation between the type of ingested drug and the time elapsed since ingestion (Miyauchi et al., 2015). Similarly, Livshits et al. identified whole tablets, fragments, granules, paste, or slurry in 9% of autopsies of fatal drug overdose cases—98% of which involved drugs known to delay gastric emptying, slow GI motility, or use SR formulations (Livshits et al., 2015).
In our retrospective study, EGD was used as a decontamination technique in 19 pediatric cases of suspected or confirmed toxic ingestion. In 15 of these cases, xenobiotic residues were identified and successfully removed, with no procedural complications reported.
The existing literature on decontaminative EGD is limited to small case series and individual reports. Table 3 summarizes 20 publications describing 32 cases of EGD-assisted decontamination. Similar to our findings, these studies found no consistent correlation between the timing of EGD and endoscopic findings. Common indications included radiographic suspicion or confirmation (via X-ray or CT) of residual tablets or bezoars in the stomach, severe clinical presentation, persistently elevated drug levels, and prior institutional or literature-based experience.
Favorable outcomes were reported in 28 out of 32 published cases. Fatalities and prolonged comas were attributed to the toxicity of the ingested substances, not to the procedure itself. Complications were rare, with only one reported case of esophageal tears, which resolved without major sequelae. Bezoars were identified in 23 of the 32 cases (Table 3).
Based on both our data and previously published reports, decontaminative gastroscopy may have a critical role in selected toxic ingestion scenarios—particularly when involving SR formulations, bezoar-forming substances, or suspected lethal doses (Gosselin et al., 2025; Buckley et al., 1995; Adams et al., 2004; Iwamuro et al., 2015). It remains difficult to define a clear timeframe for the utility of EGD. Even in cases involving the same drug (e.g., Case 6 vs. Case 16) and similar ingested quantities, endoscopic findings varied significantly. An in vitro study by Lotte et al. showed that SR formulations can form bezoars that persist for up to 48 h before fully dissolving (Hoegberg et al., 2019). Our observations support the possibility that solid residues or bezoars may remain in the gastric lumen even more than 24 h post-ingestion.
While imaging modalities such as X-ray or CT scans can assist in identifying retained gastric contents, their utility is limited for non-radiopaque drugs (Guillermo et al., 2014; Sato and Kamijo, 2014; Gavala et al., 2017; Labarinas et al., 2018; McCarthy and Coleman, 2023; Briggs and Deal, 2014; Höjer and Personne, 2008; Johnson et al., 2017; von Düring et al., 2019; Wells et al., 2006; Madan et al., 2021). CT scans are further constrained by radiation exposure concerns and limited availability. Our center is currently exploring the potential role of abdominal ultrasound in detecting residual gastric materials.
Table 4 outlines drugs prone to bezoar formation and those that are radiopaque, based on our experience and prior literature. In many cases, multiple GD techniques were employed concurrently.
We remain cautious about the use of GL. Published studies question its efficacy in removing high-risk ingested doses. Moreover, in cases involving bezoars, GL may break them apart, potentially increasing absorption and limiting the subsequent effectiveness of EGD. In our 15 cases where GL was performed prior to EGD, 12 patients still had significant amounts of bezoars, tablets, or drug-containing material.
At present, data do not support the routine use of gastroscopy in all poisoning cases. However, our findings suggest that EGD can be valuable in selected scenarios, particularly when performed by trained personnel and in the absence of contraindications (Gosselin et al., 2025; Nelson, 2000; Livshits et al., 2015; Buckley et al., 1995; Adams et al., 2004; Iwamuro et al., 2015; Marano et al., 2023). Though EGD may appear invasive, it could prevent the need for more aggressive interventions such as CVVHDF or ECMO in life-threatening overdoses. The availability of skilled practitioners is a key determinant for its use.
Pediatric patients pose unique challenges for GD, including weight-based dosing thresholds, the need for appropriately sized equipment, and the often uncooperative nature of younger children. While adult GD guidelines remain incomplete, evidence in pediatric populations is even more limited. Apart from our study, only seven published case reports describe EGD for decontamination in patients under 18 years (Labarinas et al., 2018; Allen et al., 2022; Johnson et al., 2017; Djogovic et al., 2007; Cereda et al., 1986; Marano et al., 2023; Marano et al., 2024).
This study presents several limitations that should be acknowledged. First, the retrospective study design and relatively small sample size limit the generalizability of the findings. Second, the absence of standardized guidelines to define the appropriateness of the procedure introduces a degree of subjectivity in the clinical decision-making process. This variability may have influenced both the selection of patients and the interpretation of endoscopic findings. Further research with larger cohorts and clearer procedural indications is needed to validate these preliminary observations and to establish evidence-based protocols.
In summary, based on our experience with 19 pediatric patients and 32 previously reported cases, EGD may be a useful tool in managing specific poisonings—particularly those involving massive ingestion, SR formulations, GI motility-impairing substances, or in cases where life-threatening ingestion cannot be ruled out. Our findings underscore the need to better define the role of gastroscopy in clinical toxicology, including standardized indications and contraindications. Further studies are essential to develop evidence-based guidelines for its integration into poisoning management protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adams B. K. Mann M. D. Aboo A. Isaacs S. Evans A. (2004). Prolonged gastric emptying half-time and gastric hypomotility after drug overdose. Am. Journal Emergency Medicine 22 (7), 548–554. 10.1016/j.ajem.2004.08.017 15666259 · doi ↗ · pubmed ↗
- 2Albertson T. E. Owen K. P. Sutter M. E. Chan A. L. (2011). Gastrointestinal decontamination in the acutely poisoned patient. Int. J. Emerg. Med. 4, 65. 10.1186/1865-1380-4-65 21992527 PMC 3207879 · doi ↗ · pubmed ↗
- 3Allen K. Kane I. Connors N. Tecklenburg F. Marvin W. (2022). EGD for refractory toxidromes: is it time to add to the algorithm? J. Investigative Medicine High Impact Case Reports 10. 10.1177/23247096221106760 35748419 PMC 9234829 · doi ↗ · pubmed ↗
- 4American Academy of Clinical Toxicology and European Association of Poisons Centres and Clinical Toxicologists (2005). Position paper: single-dose activated charcoal. Clin. Toxicol. 43 (2), 61–87. 10.1081/CLT-51867 15822758 · doi ↗ · pubmed ↗
- 5Benson B. E. Hoppu K. Troutman W. G. Bedry R. Erdman A. Höjer J. (2017). Position paper update: gastric lavage for gastrointestinal decontamination. Clin. Toxicol. (Philadelphia, Pa.) 51 (3), 140–146. 10.3109/15563650.2013.770154 23418938 · doi ↗ · pubmed ↗
- 6Briggs A. L. Deal L. L. (2014). Endoscopic removal of pharmacobezoar in case of intentional potassium overdose. J. Emergency Medicine 46 (3), 351–354. 10.1016/j.jemermed.2013.08.031 24113476 · doi ↗ · pubmed ↗
- 7Buckley N. A. Dawson A. H. Reith D. A. (1995). Controlled release drugs in overdose. Clinical considerations. Drug Safety 12 (1), 73–84. 10.2165/00002018-199512010-00006 7741985 · doi ↗ · pubmed ↗
- 8Cereda J. M. Scott J. Quigley E. M. (1986). Endoscopic removal of pharmacobezoar of slow-release theophylline. Br. Medical Journal Clin. Research ed. 293 (6555), 1143. 10.1136/bmj.293.6555.1143 3094809 PMC 1341853 · doi ↗ · pubmed ↗