The impact of circulating tumor DNA on the prognosis of liver cancer and its predictive value: a meta analysis
Bing Wu, Shuhui Ke, Lingling Zhu, Rongrong Dong, Jinqian Luan

TL;DR
This study finds that circulating tumor DNA (ctDNA) is linked to worse outcomes in liver cancer patients and may help predict cancer recurrence.
Contribution
The study provides a meta-analysis showing ctDNA's prognostic and predictive value in hepatocellular carcinoma (HCC).
Findings
ctDNA positivity is significantly associated with poorer overall survival in HCC patients.
ctDNA detected postoperatively shows higher accuracy in predicting recurrence.
The pooled AUC for recurrence-free survival prediction is 0.66.
Abstract
ctDNA is a promising biomarker in oncology. However, its prognostic and predictive value in HCC remains underexplored. This meta-analysis aims to evaluate the prognostic impact of ctDNA in HCC and its predictive value for recurrence. A systematic review and meta-analysis were performed following PRISMA guidelines. PubMed, Embase, Web of Science, and CNKI were searched up to 1 June 2025, for studies assessing ctDNA in HCC patients with reported survival outcomes or predictive accuracy. Studies reporting hazard ratios for overall or disease-free survival, or AUCs for prediction, were included. Two reviewers independently screened studies and assessed quality using the Newcastle-Ottawa Scale (NOS). Meta-analyses used random- or fixed-effects models depending on heterogeneity, with sensitivity analyses performed to assess robustness. A total of 219 records were screened from PubMed,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
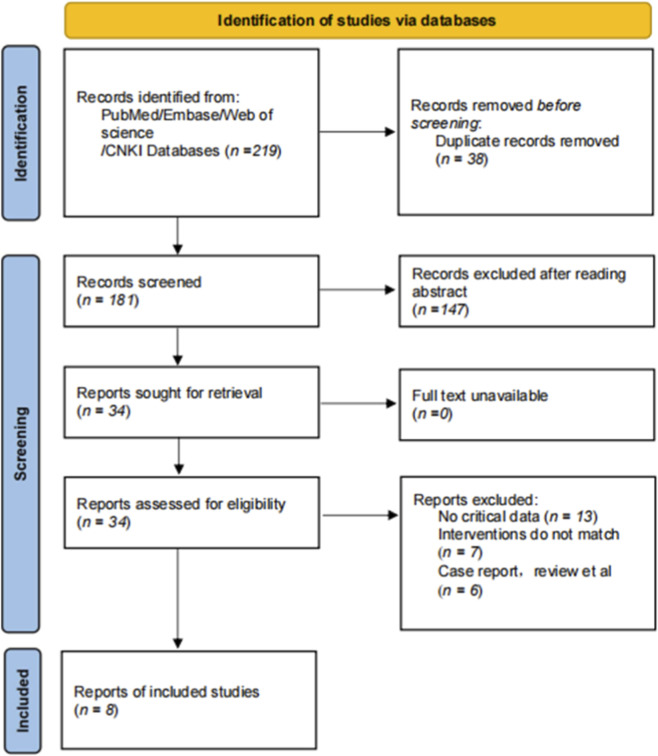 FIGURE 1
FIGURE 1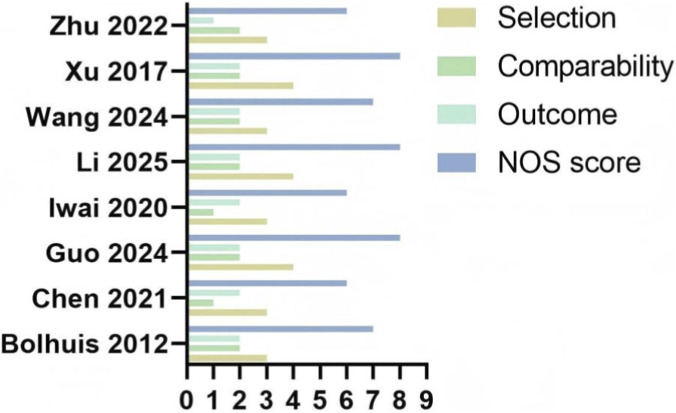 FIGURE 2
FIGURE 2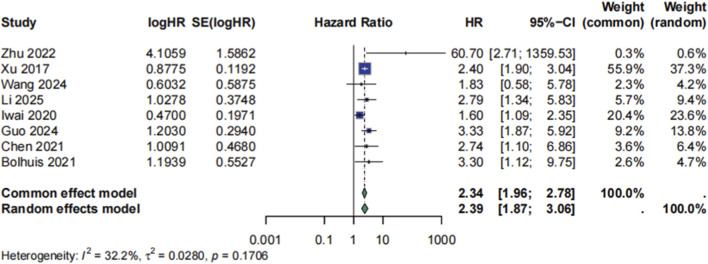 FIGURE 3
FIGURE 3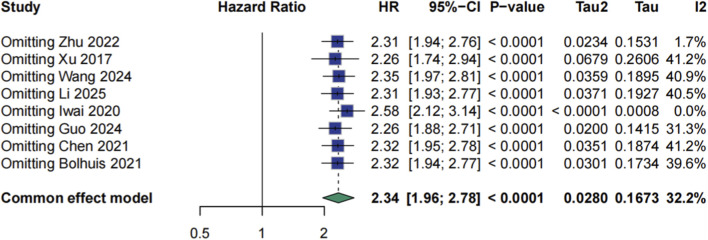 FIGURE 4
FIGURE 4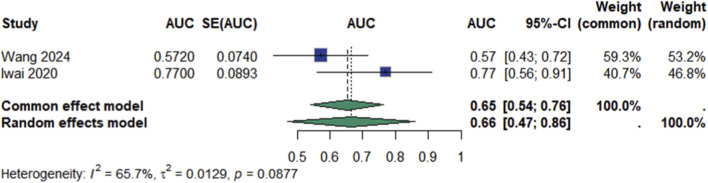 FIGURE 5
FIGURE 5| First author | Publication year | Number of cases | Age (year) | Gender | ctDNA calculating methods | Countries | |
|---|---|---|---|---|---|---|---|
| Male | Female | ||||||
|
| 2021 | 23 | 63 (54–76) | 8 | 15 | ddPCR | Netherlands |
|
| 2021 | 208 | 53.91 ± 8.24 | 162 | 46 | ddPCR | China |
|
| 2024 | 293 | 51 (30–81) | 246 | 47 | qPCR | China |
|
| 2020 | 41 | 69 (18–85) | 25 | 16 | qPCR | Japan |
|
| 2025 | 126 | Non-recurrence group 49.42 ± 10.07 | 96 | 30 | ddPCR | China |
|
| 2024 | 67 | ≥60 27cases; <60 40cases | 39 | 28 | qPCR | China |
|
| 2017 | 1,098 | 55 (15–81) | 905 | 130 | ddPCR | China |
|
| 2022 | 41 | >50 34cases; <50 7cases | 35 | 6 | ddPCR | China |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Genomics and Diagnostics · Single-cell and spatial transcriptomics · Hepatocellular Carcinoma Treatment and Prognosis
Introduction
Hepatocellular carcinoma (HCC) is one of the most prevalent malignancies worldwide and represents a major cause of cancer-related mortality (Chen et al., 2020). Its global burden continues to rise, particularly in regions with high prevalence of chronic hepatitis B and C infection, as well as among populations affected by alcohol-related liver disease and non-alcoholic fatty liver disease (Court et al., 2018). Despite advances in surgical resection, liver transplantation, and systemic therapies, the prognosis for patients with HCC remains poor, characterized by high recurrence rates and limited overall survival, especially in advanced stages (El-Mezayen et al., 2022).
Accurate risk stratification and early recurrence detection are critical for improving clinical outcomes in HCC (Jiang et al., 2024). Conventional surveillance strategies, including imaging and serum biomarkers such as alpha-fetoprotein, often lack the sensitivity and specificity required for timely and individualized management (El-Mezayen et al., 2022). These limitations have prompted the search for novel, dynamic biomarkers capable of capturing the molecular and biological complexity of HCC throughout the disease course (Jiang et al., 2024).
Circulating tumor DNA (ctDNA), comprising fragments of tumor-derived genetic material released into the bloodstream, has emerged as a promising non-invasive biomarker (Alemayehu et al., 2024a). In HCC, growing evidence suggests that the presence and quantitative characteristics of ctDNA may be associated with clinical outcomes, including disease-free survival and overall survival. However, existing studies vary widely in methodology, detection techniques, and clinical endpoints, leading to inconsistent findings and uncertainty regarding the clinical utility of ctDNA in routine practice (Alemayehu et al., 2024b).
In this study, we conducted a comprehensive meta-analysis to evaluate the prognostic and predictive value of ctDNA in patients with HCC. By systematically synthesizing the current evidence, we aim to clarify the role of ctDNA in forecasting clinical outcomes and to support its potential integration into the prognostic framework of HCC management.
Methods
Search strategy
We conducted a systematic review and meta-analysis in accordance with PRISMA guidelines. A comprehensive search was conducted in PubMed, Embase, Web of Science, and CNKI from inception to 1 June 2025, using combinations of the following terms: “hepatocellular carcinoma”, “circulating tumor DNA”, “ctDNA”, “prognosis”, “survival”, “recurrence”, and “liquid biopsy”. No language restrictions were applied. Additional studies were identified by screening reference lists of relevant articles and reviews. A complete list of search terms and strategies is provided in Supplementary Table S1.
Selection criteria
Studies were included if they met the following criteria (Chen et al., 2020): patients were diagnosed with hepatocellular carcinoma based on pathological or radiological criteria (Court et al., 2018); ctDNA was evaluated after curative-intent therapy in peripheral blood using any validated molecular method. A sample was considered ctDNA-positive if at least one mutation was detected in ctDNA with the matched tumor (El-Mezayen et al., 2022); the study reported hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for overall survival (OS) and/or disease-free survival (DFS), or provided sufficient data to estimate HRs; and/or (Jiang et al., 2024) the study assessed the discriminatory ability of ctDNA for predicting survival outcomes using the time-dependent area under the curve (AUC). Case reports, reviews, conference abstracts without sufficient data, and studies with overlapping patient populations were excluded.
Data extraction and quality assessment
Two reviewers independently screened titles, abstracts, and full-text articles for eligibility. Discrepancies were resolved through discussion or consultation with a third reviewer. When multiple models were presented, the most adjusted HRs were prioritized. Study quality was assessed using the Newcastle-Ottawa Scale (NOS) for cohort studies.
Outcomes
The primary outcome was the association between ctDNA status (positive vs. negative or high vs. low levels) and survival outcomes, expressed as HRs for overall survival and disease-free survival. The secondary outcome was the predictive accuracy of ctDNA for recurrence-free survival, assessed by time-dependent AUCs.
Statistical analysis
Meta-analysis was performed using R software (version 4.3.3) with the “meta” and “metafor” packages. For predicted outcomes, the area under the curve (AUC) values were used, while for dichotomous outcomes, HR were calculated. The results were expressed as odds ratios with 95% confidence intervals (CIs). Heterogeneity was assessed using the I^2^ statistic, with a random-effects model applied if I^2^ ≥ 50%, and a fixed-effect model used if I^2^ < 50%. Sensitivity analysis was performed to assess the robustness of the results.
Results
Study selection and characteristics
A total of 219 records were retrieved from PubMed, Embase, Web of Science, and China National Knowledge Infrastructure (CNKI). After removing 38 duplicates, we screened 181 unique articles by title and abstract, excluding 147 for irrelevance. We assessed the full texts of the remaining 34 articles and identified 8 eligible studies (Bolhuis et al., 2021; Chen and Kaiwen, 2021; Guo et al., 2024; Iwai et al., 2020; Li et al., 2025; Wang et al., 2024a; Xu et al., 2017; Zhu et al., 2022), comprising a combined total of 1,907 patients (Figure 1). Quality assessment using the Newcastle-Ottawa Scale (NOS) indicated moderate to high methodological quality across all studies, with a median score of 7 (Figure 2).
Flow chart.
Summary of risk of bias.
Baseline characteristics of the included cohorts are presented in Table 1. The pooled population was predominantly male (78.3%, 1,493/1,907), with a median age of 55 years (range: 15–85 years). The included studies varied considerably in sample size, ranging from 23 to 1,098 participants (Table 1).
Prognostic impact of ctDNA on survival
Meta-analysis using a random-effects model demonstrated a significant association between ctDNA positivity and worse overall survival (OS), with a pooled hazard ratio (HR) of 2.34 (95% CI: 1.96–2.78, p < 0.0001; Figure 3). Moderate heterogeneity was observed (I^2^ = 32.2%, τ^2^ = 0.0280, p = 0.17). Sensitivity analyses excluding each study in turn yielded consistent results, with HRs ranging from 2.26 to 2.58, indicating the robustness of the association (Figure 4).
Meta analysis for HR of prognosis.
Sensitive analysis for HR of prognosis.
Predictive value for recurrence-free survival (RFS)
Two studies (Iwai et al., 2020; Wang et al., 2024b) reported on the predictive accuracy of ctDNA for RFS. The pooled area under the curve (AUC) was 0.66 (95% CI: 0.47–0.86), with substantial heterogeneity (I^2^ = 65.7%, p = 0.09; Figure 5). Notably, the discriminative ability was higher in Iwai 2020 (AUC: 0.77 [0.56–0.91]) than in Wang 2024 (AUC: 0.57 [0.43–0.72]), which may reflect differences in ctDNA sampling timepoints or methodological approaches.
Meta analysis of Recurrence-Free Survival.
Discussion
This meta-analysis underscores the significant prognostic relevance of ctDNA in patients with HCC (Huang et al., 2022). The consistent association between ctDNA positivity and poor OS across studies suggests that ctDNA is not merely a reflection of tumor burden but a biologically meaningful marker of aggressive disease phenotypes (Zhang et al., 2021). It likely integrates multiple dimensions of tumor biology, including proliferative potential, vascular invasion, and metastatic propensity (Aalami et al., 2024). Notably, the prognostic value of ctDNA is not unique to HCC. A recent meta-analysis in pancreatic malignancies also reported that ctDNA-positive status was significantly associated with worse overall survival (HR = 2.00), reinforcing the role of ctDNA as a robust, pan-cancer prognostic biomarker across different solid tumors (Arayici et al., 2024).
The biological rationale supporting the prognostic role of ctDNA lies in its origin and dynamics. ctDNA is released into circulation during cellular apoptosis, necrosis, or active secretion by tumor cells, with its abundance influenced by factors such as tumor size, vascularity, immune clearance, and cellular turnover (Tan et al., 2021). In HCC, where tumors are often heterogeneous and vascularized, ctDNA may serve as a proxy for intratumoral heterogeneity and the presence of aggressive subclones (Cheng et al., 2019). The observed association with OS may therefore reflect an underlying biological shift toward systemic dissemination and resistance to host defenses or therapy (Cui et al., 2020).
The moderate heterogeneity observed among included studies is likely attributable to differences in detection platforms, patient populations, and definitions of ctDNA positivity (Chandrapalan et al., 2022). Some studies utilized PCR-based methods, which target specific mutations with high sensitivity, while others applied broader sequencing techniques that allow for comprehensive mutation profiling but with variable analytical depth (Li et al., 2022). Despite these methodological differences, sensitivity analyses confirmed the robustness of the association with OS, suggesting that the prognostic value of ctDNA remains consistent regardless of assay modality (Oussalah et al., 2018).
In evaluating the predictive performance for RFS, the pooled AUC indicated only modest discriminative accuracy (Liu et al., 2022). This may reflect, in part, methodological heterogeneity among the included studies, particularly regarding the timing and frequency of ctDNA sampling. Studies that performed ctDNA detection during the postoperative or surveillance phase generally reported higher AUCs, suggesting a more effective role for ctDNA in identifying minimal residual disease. Mechanistically, this aligns with the concept that residual malignant clones shed fragmented DNA into the circulation before they are radiologically detectable. ctDNA may thus serve as a leading indicator of molecular relapse, offering a window for earlier intervention (Lumkul et al., 2024). In contrast, pre-treatment ctDNA levels may reflect bulk tumor burden rather than residual disease potential, limiting their utility in forecasting recurrence. These observations underscore the importance of temporal context in ctDNA interpretation and point to the need for standardized protocols regarding assay timing and clinical thresholds.
From a translational perspective, ctDNA holds several theoretical and practical advantages over conventional surveillance tools in hepatocellular carcinoma. Biologically, ctDNA reflects tumor-derived genetic and epigenetic alterations, such as mutations in TP53, TERT promoter, or CTNNB1, as well as methylation changes and fragmentomic signatures. These features allow for a more nuanced understanding of tumor behavior, clonal evolution, and response dynamics (Lumkul et al., 2024). Unlike static biomarkers such as AFP or imaging modalities that rely on structural changes, ctDNA enables real-time monitoring of tumor kinetics and treatment efficacy, potentially capturing molecular resistance before clinical progression (Jin et al., 2019). Furthermore, in patients with impaired hepatic function or elevated bleeding risk, where invasive biopsy is contraindicated, ctDNA offers a safe and repeatable alternative for tumor genotyping and longitudinal assessment. The ability to track tumor-specific molecular profiles through serial blood sampling may ultimately support a shift toward more personalized, adaptive management strategies in HCC (Lumkul et al., 2024). However, the implementation of ctDNA-based monitoring in routine practice requires rigorous validation of its sensitivity, specificity, and cost-effectiveness in prospective studies.
Despite these promising implications, this meta-analysis has several limitations. First, the number of included studies was limited, and their predominantly retrospective design may introduce bias and confounding. Additionally, substantial variability in ctDNA detection methods, thresholds, and sampling timepoints, coupled with the frequent lack of key methodological details such as the blood volume used for cfDNA isolation, may compromise the comparability and sensitivity of ctDNA assessments across studies. Moreover, most studies did not adjust for clinical variables such as tumor stage or treatment type, limiting interpretation of independent prognostic value. Furthermore, the assessment of ctDNA’s predictive accuracy for recurrence was based on only two studies with significant heterogeneity, which precludes strong conclusions in this regard. Finally, the generalizability of our findings may be constrained by the geographical concentration of the included patient cohorts, which were primarily from Asian and European populations. Therefore, future research is needed to validate the prognostic value of ctDNA in broader geographical and ethnic cohorts.
In conclusion, this study supports ctDNA as a promising biomarker for prognostication and recurrence prediction in HCC. Its detection correlates with worse survival outcomes and shows potential for early identification of molecular relapse. However, broader validation in prospective, well-annotated cohorts is necessary. Standardized workflows, defined reporting frameworks, and integration with imaging and clinical parameters will be key to realizing the clinical utility of ctDNA in the management of HCC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aalami A. H. Aalami F. Aliabadi E. K. Amirabadi A. Sahebkar A. (2024). Detection of circulating cell-free DNA to diagnose hepatocellular carcinoma in Chinese population: a systematic review and meta-analysis. Curr. Med. Chem. 31 (22), 3345–3359. 10.2174/0929867330666230622114235 37349993 · doi ↗ · pubmed ↗
- 2Alemayehu E. Belete M. A. Walle M. Getu F. Mulatie Z. Teshome M. (2024 a). Diagnostic accuracy of circulating mi RN As to discriminate hepatocellular carcinoma from liver cirrhosis: a systematic review and meta-analysis. Front. Med. (Lausanne) 11, 1359414. 10.3389/fmed.2024.1359414 38721351 PMC 11076824 · doi ↗ · pubmed ↗
- 3Alemayehu E. Fasil A. Ebrahim H. Mulatie Z. Bambo G. M. Gedefie A. (2024 b). Circulating micro RN As as promising diagnostic biomarkers for hepatocellular carcinoma: a systematic review and meta-analysis. Front. Mol. Biosci. 11, 1353547. 10.3389/fmolb.2024.1353547 38808007 PMC 11130514 · doi ↗ · pubmed ↗
- 4Arayici M. E. İnal A. Basbinar Y. Olgun N. (2024). Evaluation of the diagnostic and prognostic clinical values of circulating tumor DNA and cell-free DNA in pancreatic malignancies: a comprehensive meta-analysis. Front. Oncol. 14, 1382369. PMID: 38983931; PMCID: PMC 11231086. 10.3389/fonc.2024.1382369 38983931 PMC 11231086 · doi ↗ · pubmed ↗
- 5Bolhuis K. van 't Erve I. Mijnals C. Delis-Van Diemen P. M. Huiskens J. Komurcu A. (2021). Postoperative circulating tumour DNA is associated with pathologic response and recurrence-free survival after resection of colorectal cancer liver metastases. E Bio Medicine 70, 103498. 10.1016/j.ebiom.2021.103498 34333237 PMC 8340125 · doi ↗ · pubmed ↗
- 6Chandrapalan S. Bannaga A. Weidner A. Hitchins M. P. Arasaradnam R. P. (2022). A systematic review and meta-analysis: the diagnostic accuracy of methylated SEPTIN 9 for the detection of hepatocellular carcinoma and the clinical evaluation of its use in combination with other surveillance modalities. Scand. J. Gastroenterol. 57 (4), 473–480. 10.1080/00365521.2021.2020331 34957898 · doi ↗ · pubmed ↗
- 7Chen Y. Kaiwen D. (2021). Predictive value of ct DNA in short-term recurrence after radical hepatectomy for hepatocellular carcinoma patients. Pract. Med. J. 38 (06), 504–507+77.
- 8Chen V. L. Xu D. Wicha M. S. Lok A. S. Parikh N. D. (2020). Utility of liquid biopsy analysis in detection of hepatocellular carcinoma, determination of prognosis, and disease monitoring: a systematic review. Clin. Gastroenterol. Hepatol. 18 (13), 2879–9029. 10.1016/j.cgh.2020.04.019 32289533 PMC 7554087 · doi ↗ · pubmed ↗