Feeding practices of under-two children in Ethiopia: A systematic review and meta-analysis
Sisay Eshete Tadesse, Amare Tariku, Tefera Belachew

TL;DR
This study reviews feeding practices for children under two in Ethiopia and finds they are below recommended levels, increasing malnutrition risks.
Contribution
The study provides the first comprehensive meta-analysis of infant feeding practices in Ethiopia, identifying key factors influencing these practices.
Findings
Only 58.6% of children were exclusively breastfed, and 20.4% had optimal feeding practices.
Antenatal care, place of delivery, and postnatal care were strongly associated with better feeding practices.
Nutrition education and husband support significantly improved infant feeding outcomes.
Abstract
Globally, child feeding practices remain suboptimal and contribute substantially to a high burden of malnutrition. In Ethiopia, evidence on the overall status of feeding practices among children under two years of age is limited. This study therefore sought to estimate the pooled prevalence of timely initiation of breastfeeding, exclusive breastfeeding, timely initiation of complementary feeding, and minimum acceptable diet, as well as to identify the factors associated with these practices. This systematic review and meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines. A comprehensive literature search was performed in Scopus, HINARI, the Cochrane Library, and PubMed/MEDLINE. Cross-sectional and case-control studies published in English were included. Study quality was assessed using the Joanna Briggs Institute…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
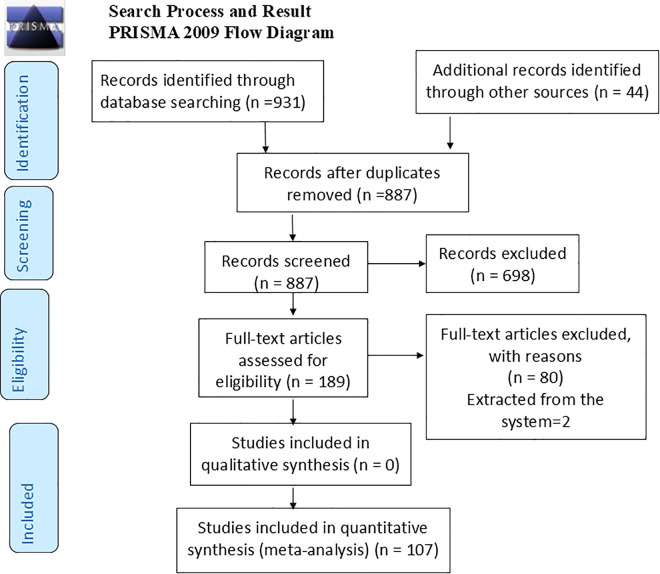 Fig 1
Fig 1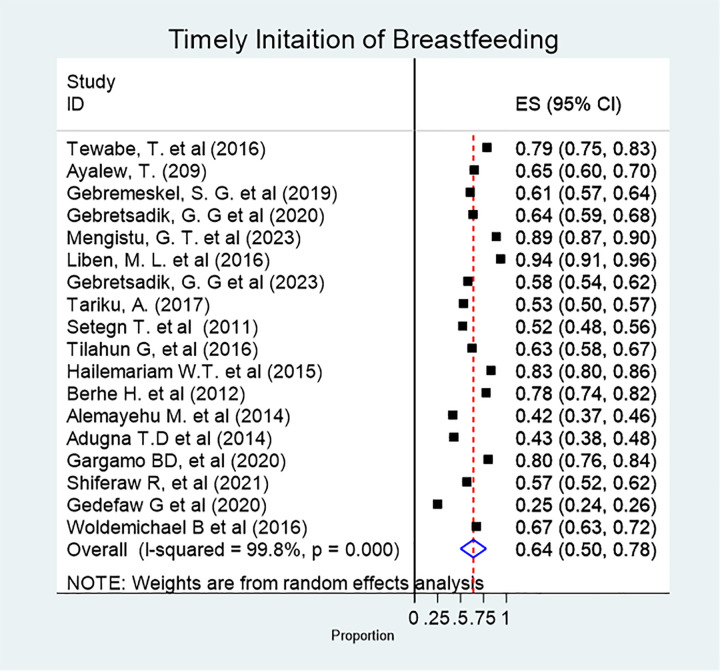 Fig 2
Fig 2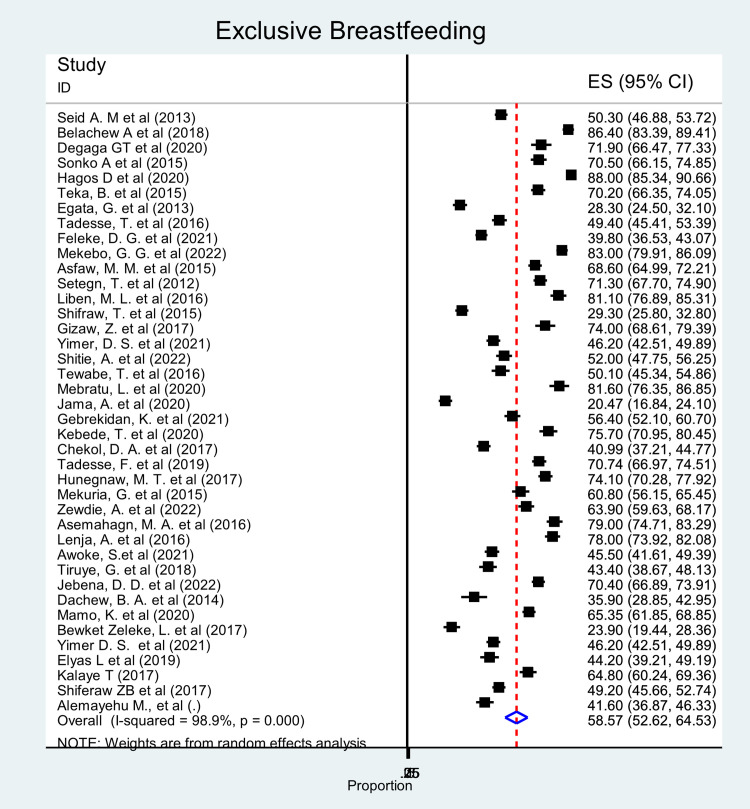 Fig 3
Fig 3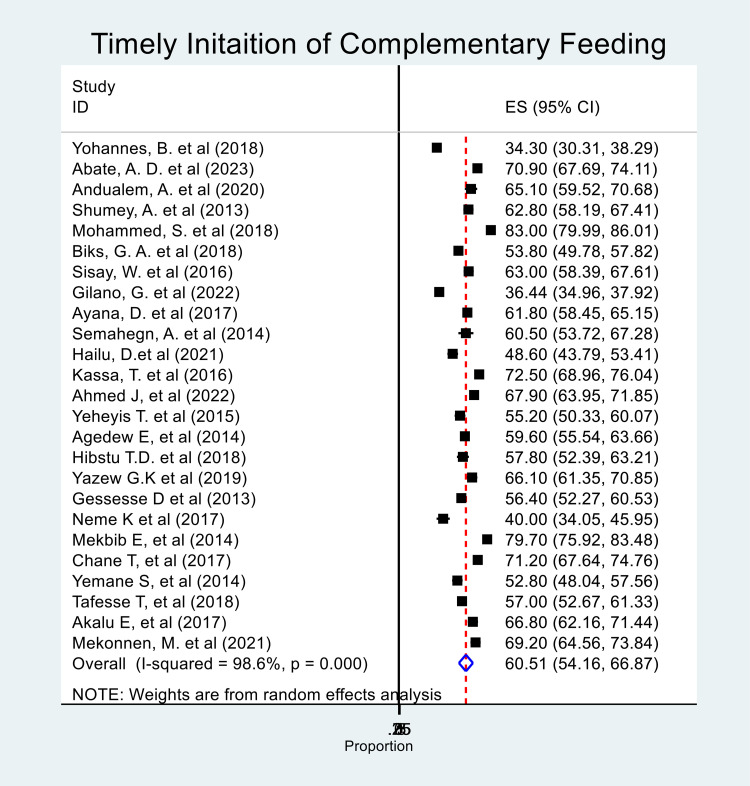 Fig 4
Fig 4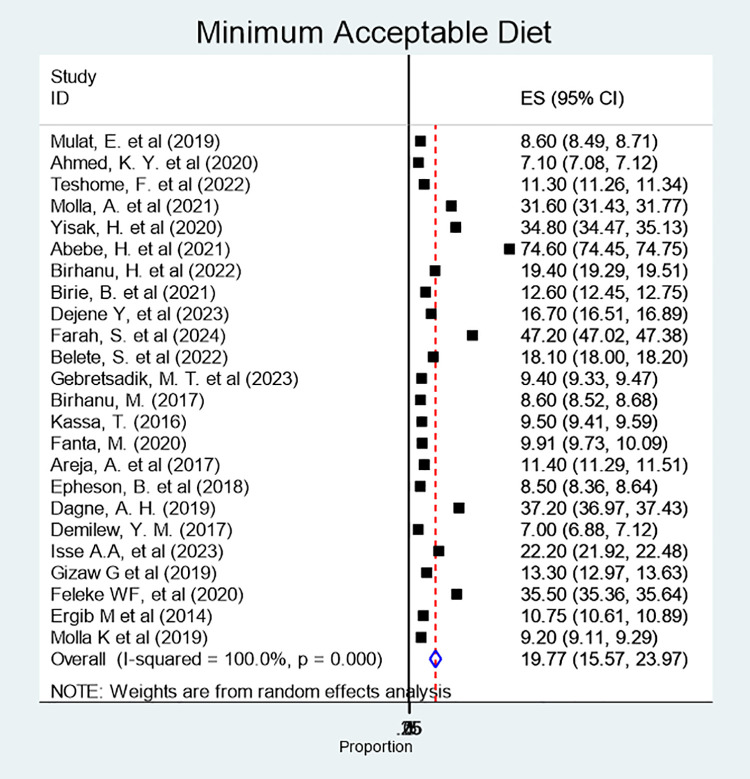 Fig 5
Fig 5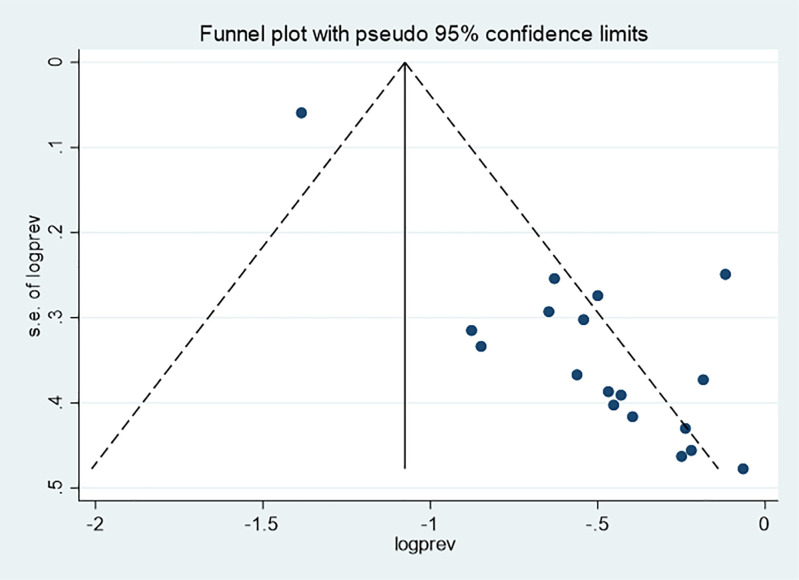 Fig 6
Fig 6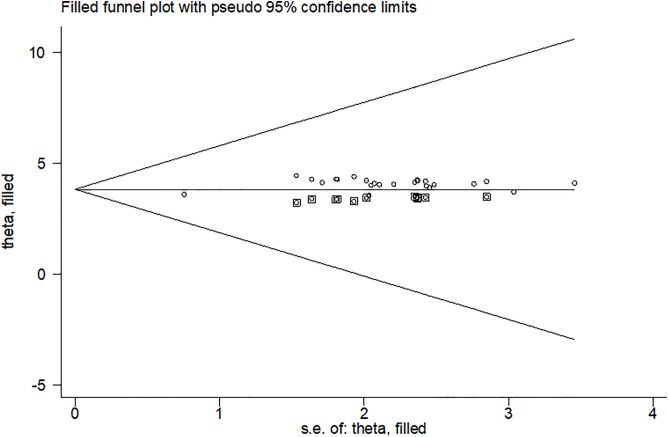 Fig 7
Fig 7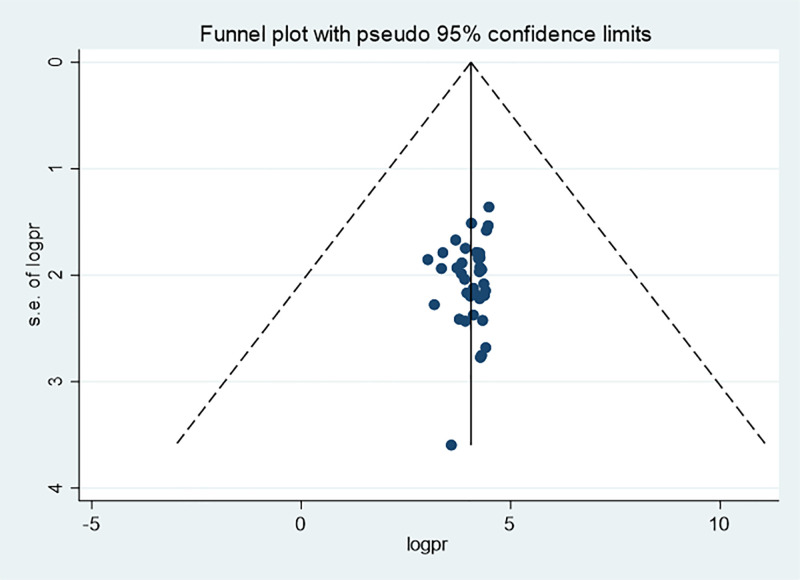 Fig 8
Fig 8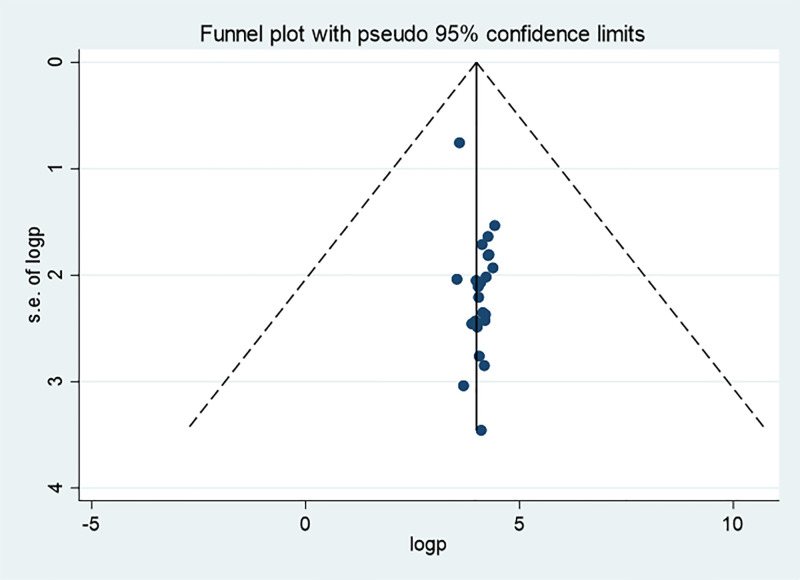 Fig 9
Fig 9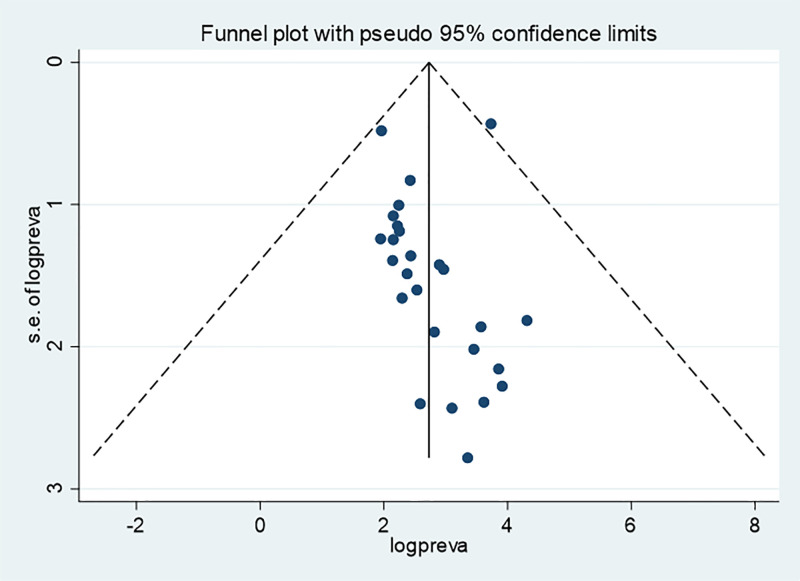 Fig 10
Fig 10Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Child Nutrition and Water Access · Child Nutrition and Feeding Issues
Introduction
Infant feeding practices are key determinants of child health and development. The World Health Organization (WHO) recommends exclusive breastfeeding for the first six months of life, followed by the introduction of complementary foods while continuing breastfeeding up to two years of age or beyond [1]. Globally, nearly half (49%) and 44% of the newborns-initiate breastfeeding within one hour of birth and exclusively breastfed for the first six months, respectively [2]. According to the 2020 global nutrition report, only 18.9% of children aged 6–23 months receive a nutritionally adequate diet [3]. In developing countries, 42% of infants are exclusively breastfed for six months of age, and 73% of children aged 6–8-months receive solid, semisolid, and soft foods [2].
Sub-optimal infant feeding practices are strongly linked to high morbidity and mortality among children. Most growth deficits occur between 6–12 months of age [4] and inappropriate feeding practices contribute up to a third of all cases of child malnutrition [5]. Current data suggest that over 1 million children die each year due to wasting [6]. Many children under-two-year experience delayed introduction of complementary foods, are fed infrequently, or receive foods of inadequate quality [7–9]. Such sub-optimal feeding practices contribute to feeding difficulties, increased risk of infection and allergies, early cessation of breastfeeding, undernutrition, obesity in childhood and adulthood, reduced breast milk intake, and long-term impacts on feeding performance [10,11].
Previous studies have shown that maternal education and age, antenatal care, postnatal care, place of delivery, household wealth, place of residence, maternal employment, household size, and father’s education all significantly influence feeding behaviors [12–15].
Despite the well-established benefits of optimal infant feeding practices, suboptimal practices remain widespread in many regions, including Ethiopia. The 2019 Ethiopian Demographic and Health Survey (EDHS) reported that only 59% of infants under six months were exclusively breastfed, and merely 11.3% of children aged 6–23 months received a minimum acceptable diet [16]. World Bank estimates indicate that undernourished children may lose over 10% of their potential lifetime earnings, adversely affecting national productivity [17]. Although many studies were conducted on infant feeding practices, there were inconsistencies across studies, posing challenges for policymakers, practitioners, and stakeholders in making evidence-based decisions.
Previous systematic reviews and meta-analyses on child feeding practices in Ethiopia have several limitations. For instance, a systematic review and meta-analysis (SRMA) on timely initiation of breastfeeding (TIBF) included a retracted article and focused specifically on the effects of cesarean delivery and kangaroo mother care on preterm and low-birth-weight infants [13]. Similarly, a SRMA on exclusive breastfeeding (EBF) examined only a single influencing factor [14,15]. A SRMA on a minimum acceptable diet (MAD) included only nine studies and didn’t address the determinants [18]. Moreover, earlier SRMA predominantly included cross-sectional studies, limiting the comprehensiveness of the evidence.
The current study addresses the gaps identified in previous SRMA by incorporating a larger number of studies (107) including both case-control and cross-sectional designs, and examining the determinants of infant feeding practices. It also considers four core IYCF indicators: TIBF, EBF, TICF and MAD. This SRMA provides a comprehensive and rigorous synthesis of the available evidence on child feeding practices and will inform decision-making, guide resource allocation, and offer new insight for designing interventions to improve IYCF practices and reduce the burden of malnutrition in Ethiopia.
Materials and methods
Study setting
This systematic review and meta-analysis was conducted in Ethiopia, a country located in the northeastern part of Africa, also known as the Horn of Africa, and one of the most populous nations in the region. Traditional child feeding malpractices such as prelacteal feeding, discarding colostrum and inappropriate timing of complementary feeding remain a major concern, adversely affecting the health of many newborns and young children. Since 2000, efforts to reduce child malnutrition have been implemented through various intervention strategies, including the IYCF program, Seqota declaration, scaling up nutrition, multisectoral nutrition coordination, food and nutrition policy, and the National Nutrition Program, in collaboration with international partners. Similarly, one of the health packages that the country is working on is minimizing inappropriate child feeding and other maladaptive practices.
Search strategy
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [19]. Three reviewers performed a comprehensive search of relevant articles across multiple databases, including MEDLINE (via PubMed), EMBASE, Cochrane Library, SCOPUS, HINARI, and Google Scholar. In addition, gray literature was identified through manual searches.
Searching terms
Search strategies for each database were developed based on the CoCoPop framework:
Condition: studies documenting infant feeding practices
Context: studies conducted in Ethiopia
Population: Studies targeting children under two years of age were included
Relevant articles were searched using the following searching terms: (prevalence) OR (magnitude) AND (determinants) OR (“associated factors”) OR (“risk factors”) AND (“infant feeding practices”) AND (“exclusive breastfeeding”) OR (complementary feeding*) OR (“minimum acceptable diet”) OR (optimum nutrition) AND (Ethiopia). Since no eligible studies were found prior to 2011, only articles published from 2011 onwards were included. This SRMA was registered in PROSPERO with a CRD number of 42023489496. No separate study protocol was prepared.
Eligibility criteria
All studies conducted in Ethiopia that reported prevalence, determinants and factors associated with infant feeding practices, which were published in English were included. Both cross-sectional and case-control study designs were considered. Studies were excluded if the full text was unavailable after attempting to contact the primary investigator for three months, systematic reviews of interventions, review articles, conference abstracts, and editorials.
Data extraction
After obtaining the full texts, duplicates were identified and removed using EndNote. Data extraction was conducted independently by three reviewers (SE, TB, and AT), who screened titles, abstracts, and full articles. The study selection procedure is presented using a PRISMA flow diagram [19]. Studies that met the inclusion criteria were retained, while those “included” and “undecided” studies underwent further full-text assessment. To minimize bias, reviewers independently ranked articles without knowing each other’s decisions, and any discrepancies were resolved through discussion and consensus. Data were then extracted using a Microsoft Excel 2021 extraction sheet, capturing study characteristics (author, year of publication, region, target population, sample size, study design, and response rate), infant feeding practices, subject recruitment procedures, adjusted odds ratios, and population characteristics.
Quality assessment and risk of bias
The quality of included studies was assessed independently by three investigators using the Joanna Briggs Institute (JBI) critical appraisal checklist, and the quality scores were averaged. Any disagreement was resolved through discussion and consensus. During data extraction data quality was ensured by selecting reliable and relevant data sources, removing duplicates and cross-checking extracted data against the original article. Finally, studies with a score of 50% and above were included in this systematic review and meta-analysis.
Data synthesis and analysis
Data were analyzed using STATA/MP version 17.0. The prevalence of infant feeding practices was reported by the forest plots. To estimate the determinants of feeding practices, adjusted odds ratio with a 95% confidence interval (CI) was pooled. Heterogeneity between studies was assessed using the Cochrane Q statistic (significant if the P-value was < 0.05) and quantified with the I² statistic (at least 50%, was considered suggestive of statistically significant heterogeneity) [20].
A Der Simonian and Laird random-effects model was used for studies with high heterogeneity, and a fixed effects model with inverse variance methods was used for similar studies. Heterogeneity was further explored using the Galbraith plot and Forest plot. The source of heterogeneity was tested by running meta-regression, subgroup analysis by sex, age and region), and sensitivity analysis. Publication bias was assessed by funnel plots, Egger weighted regression, and Begg rank correlation tests at p-values < 0.05.
Results
Study characteristics
A total of 975 articles were retrieved from databases by a literature search (Fig 1).
Preferred Reporting Items for Systematic Review and Meta-Analysis for literature screening and selection process, June 2020.
After screening the title and abstract, 189 articles were identified as having information relevant to infant feeding practices. Following full text review, 107 articles were evaluated to have better quality data that met the criteria for abstraction. Of these, 18 studies involving 16,405 participants were included for TIBF [21–33]; 39 papers with 19,987 participants addressed EBF [34–63]; 26 papers involving 15,855 participants assessed TIBF [64–79]; and 24 papers including 15, 495 infants aged 6–23 months were included for assessing MAD [64,75, 80–99]. All included articles were full-text articles employing cross-sectional and case-control designs and were published between 2011 and 2024 (Table 1).
Table 1: Summary of Extracted Studies on Infant Feeding Practices among Under-two Children in Ethiopia.
Pooled prevalence of infant feeding practices
The pooled prevalence of TIBF was 64% (95% CI: 50, 78%). There was substantial heterogeneity among the included studies (χ² = 1404.11; p < 0.0001; I^2^ = 99.7%) (Fig 2).
Forest plot showing the pooled prevalence of timely initiation of breastfeeding among infants in Ethiopia, 2024.
Based on the subgroup analysis, the highest (77.8%) and lowest (47.4%) prevalence of TIBF was reported from Afar and Somali regions, respectively.
The pooled prevalence of EBF among under-two children was 59.6% (95% CI: 52.6, 64.5%). Significant heterogeneity was observed across studies (χ² = 3561.76; p < 0.0001; I^2^ = 98.9%, p = 0.0001) (Fig 3).
Forest plot showing the pooled prevalence of exclusive breastfeeding among children in Ethiopia, 2024.
Based on the subgroup analysis, the highest (79%) and lowest (23.9%) prevalence was reported from the Amhara region. The subgroup analysis was done by region and study setting, and still, there is high heterogeneity.
The pooled prevalence of TICF was 60.5% (95% CI: 54.2, 66.9%) with high heterogeneity between studies (chi-squared = 6066.37, I-squared = 99.6%%, p < 0.001) (Fig 4).
Forest plot showing the pooled prevalence of timely initiation of complementary feeding among infants in Ethiopia, 2024.
The pooled prevalence of MAD among children aged 6–23 months was 19.8% (95% CI: 15.6, 23. 9%) (Fig 5).
Forest plot showing the pooled prevalence of minimum acceptable diet among children aged 6-23 months, 2024.
The subgroup analysis demonstrated that studies conducted in the Amhara region and those conducted at the national level were major contributors for the observed heterogeneity.
Sensitivity analysis
The sensitivity analysis demonstrated that the quality score didn’t affect the outcome of the meta-analysis and there was no significant difference in the overall pooled prevalence.
Publication bias
Publication bias was assessed both subjectively using a funnel plot and objectively using Begg’s and Egger’s tests. For TIBF, the funnel plot and Egger’s test (p = 0.011) suggested the presence of publication bias, whereas Begg’s test indicated no evidence of publication bias (p = 0.289) (Fig 6).
Funnel plot for timely initiation of breastfeeding among infants in Ethiopia, 2024.
Consequently, a trim and fill analysis was done for TIBF (Fig 7).
Funnel plots based on trim and fill analysis for the timely initiation of breastfeeding in children aged 6-23 months in Ethiopia, 2024.
The funnel plot for EBF visually suggested the presence of publication bias, however, both Begg’s (p = 0.556) and Egger’s (p = 0.433) tests didn’t indicate statistically significant publication bias (Fig 8).
Funnel plot for exclusive breastfeeding of infants in Ethiopia, 2024.
Regarding TICF, neither the funnel plot nor Begg’s (p = 0.056) and Egger’s (p = 0.060) tests showed evidence of publication bias (Fig 9).
Funnel Plot for the timely initiation of complementary feeding among children aged 6-23 months in Ethiopia, 2024.
Similarly, the funnel plot for MAD practices showed the presence of possible publication bias; but Begg’s (p = 0.89) and Egger’s (p = 0.934) tests revealed no statistically significant publication bias (Fig 10).
Funnel plot for minimum acceptable diet among children aged 6–23 months in Ethiopia, 2024).
Factors associated with feeding practices of under-two children
Mothers who had antenatal care follow-up were almost three times more likely to initiate breastfeeding early compared with those without antenatal care (AOR = 3.4%; 95% CI: 1.5, 7.5). Mothers who delivered by cesarean section were 70% less likely to initiate breastfeeding timely than those who had vaginal delivery (AOR = 0.3; 95% CI: 0.1, 0.9). Similarly, facility-based delivery was associated with higher odds of timely initiation of breastfeeding compared with home delivery (AOR = 2.3; 95% CI: 1.1, 4.9) (Table 2).
Table 2: Determinants of feeding practices among under-two children in Ethiopia, 2024.
Infants aged 0–1 and 2–3 months were over four times and three times more likely to be exclusively breastfed compared with infants aged 4–6 months (AOR = 4.4; 95% CI: 1.4, 13.6) and (AOR = 2.5; 95% CI: 1.2, 5.1), respectively. Mothers aged 35 years and above were about three times more likely to exclusively breastfeed their children compared with younger mothers (AOR = 3.4; 95% CI: 1.3, 8.7). Rural mothers had significantly higher odds of practicing exclusive breastfeeding compared with their urban counterparts (AOR = 1.8; 95% CI: 1.1, 3.1). Unemployed mothers were also 80% more likely to exclusively breastfeed than employed mothers (AOR = 1.8; 95% CI: 1.2, 2.7). Mothers who delivered in health facilities were twice as the likelihood of exclusively breastfeed compared with those who delivered at home (AOR = 2.1; 95% CI:1.2, 3.7).
Mothers who had normal (vaginal) deliveries were 70% more likely to exclusively breastfeed than those who delivered by cesarean section (AOR = 1.7; 95 CI:1.2, 1.2, 2.6). Postnatal care attendance was also positively associated with exclusive breastfeeding (AOR = 2.3; 95% CI: 1.2, 4.3). Additionally, mothers who received breastfeeding counseling were more likely to practice exclusive breastfeeding compared to those who didn’t (AOR = 2.3; 95% CI:1.4, 3.9) and mothers who received husband support were nearly three times more likely to exclusively breastfeed their infants (AOR = 2.9; 95% CI:1.9, 4.4) (Table 2).
Mothers who attended antenatal care were almost three times more likely to initiate complementary feeding at the recommended time compared with those who did not attend ANC (AOR = 3.4; 95% CI:1.5, 7.5). Likewise, mothers who delivered in health facilities had twice the likelihood of initiating complementary feeding on time compared with mothers who delivered at home (AOR = 2.3; 95% CI:1.1, 4.9) (Table 2).
Receiving nutrition education through practical demonstrations on complementary food preparation was also associated with better feeding practices; mothers exposed to such demonstrations were twice as likely to practice optimal feeding compared with their counterparts (AOR = 2.06; 95% CI:1.28, 3.31). Additionally, children aged 18–23 months were almost three times more likely to receive optimal feeding practices than those aged 6–11 months (AOR = 2.68; 95% CI:1.18, 6.13) (Table 2).
Discussion
The aim of this study was to assess the pooled prevalence of feeding practices and the factors associated with them among children under two years of age in Ethiopia. The pooled prevalence of TIBF, EBF, TICF, and MAD were 64%, 59.56%, 59%, and 19.77%, respectively. A range of determinants were identified, including antenatal care, place and mode of delivery, postnatal care, maternal age and occupation, counseling, husband’s support, place of residence, maternal education, involvement in complementary food preparation demonstrations, and the child’s age.
The pooled prevalence of TIBF was 64%, which is in line with a SRMA done in Ethiopia (61.4%) [15], Sub-Saharan Africa (50.5%) [100] and Bangladesh [101]. According to WHO IYCF standards, it is considered good [102]. However, it was lower than the national and WHO IYCF recommendations [102,103]. But it was higher than the pooled prevalence reported among cesarean delivered mothers in Ethiopia (40.1%) and the recent estimate from 53 WHO European Region member countries (43%) [12,104]. These differences might be attributed to variations in study setting, methodological approaches, socio-demographic and economic characteristics, and health service utilization.
This study demonstrated that the pooled prevalence of EBF in Ethiopia was 59.56%. It is rated good according to the WHO IYCF standards (50%–89%). This result aligns with previous SRMA conducted in Ethiopia and Iran [14,15], the 2019 mini-EDHS report (59%), and a study in Southern Africa (56.57%) [15,105,106]. However, it is higher than the global EBF prevalence of exclusive breastfeeding (44%), SRMAs conducted in Ghana and Iran [107,108], and studies from Sub-Saharan Africa (36%), and Central Africa (53.48%) [105]. Conversely, the prevalence reported in this study is lower than findings from several regions of India and the Nepal DHS [109–111]. Such may be attributed to differences in socio-demographic and economic contexts, access to information, study periods, and methodological approaches.
This study also showed that more than half (59%) of infants received complementary feeding timely. According to WHO standards, it is rated as ‘fair’ (60–79%). This finding is consistent with a SRMA conducted in Ethiopia and a study conducted in South Asia [112,113], and it is congruent with the recent global estimate of 64.5% [114]. However, it is higher than a study conducted in five European Union countries (47%) [115]. These differences might be due to the differences in the study settings.
The pooled prevalence of minimum acceptable diet was 19.77%. This finding is consistent with a SRMA conducted in Ethiopia [18], as well as studies from South Asia [113] and Bangladesh [101], underscoring that many Ethiopian children continue to consume diets of inadequate quality [16]. However, the prevalence observed in this study is higher than the 2019 mini-EDHS report (11.3%), and the Ghana DHS [116], east Africa (11.58%) [117] and Sub-Saharan Africa (9.98%) [118]. In contrast, it was lower than reports from the Democratic Republic of Congo (33%) [119], and a study conducted in Indonesia (29%) [120]. These may reflect differences in the study methodologies, socio-demographic and economic contexts, access to diverse foods, and the time periods during which the studies were conducted.
Antenatal follow-up was identified as a predictor of TIBF. Mothers who attended ANC were three times more likely to initiate breastfeeding timely. This finding is consistent with evidence from a study done in Sub-Saharan African countries [121]. This might be because the nutrition education given during ANC visits which encourages skilled delivery and supports mothers in initiating breastfeeding soon after birth. However, this finding contrasts with studies done in Ethiopia and Namibia, where mothers who attended antenatal care were reported to be less likely to initiate breastfeeding on time [122,123]. This discrepancy may be due to variation in the interaction of health care providers during visits, as well as lack of coordinated responsibility, which could hinder the delivery of consistent messages to mothers.
This study identified place of delivery as a determinant of TIBF. Mothers delivered in a health facility were twice as likely to initiate breastfeeding on time compared with those who delivered at home. This finding is similar with evidence from a global systematic review and meta-analysis, as well as studies conducted in Iran, Namibia, and Nepal [108,123–125]. This might be because mothers who gave birth in a health facility were encouraged by health care providers through counseling and support on colostrum feeding, which enables them to initiate breastfeeding within the recommended time. Additionally, mothers delivering in health facilities are less likely to give prelacteal foods before initiating breastfeeding. On the other hand, studies from Ireland and the UK, and Canada revealed that home delivery was associated with higher odds of timely initiation of breastfeeding [126,127].
There was also a significant association between mode of delivery and TIBF. Mothers who delivered by cesarean section were 70% less likely to initiate breastfeeding timely as compared to vaginal delivery. This finding is consistent with studies conducted in Ghana and Kenya [128,129]. This may be due to post-operative care needs, pain, and fatigue, which can interfere with early skin-to-skin contact and immediate newborn care, both essential for timely initiation of breastfeeding. In contrast, a study from Central America reported a significant association between mode of delivery and timely initiation of breastfeeding [130]. This inconsistency may be due to the difference in socio-economic conditions and the quality and accessibility of health care services.
Younger children were more likely to be exclusively breastfed than older ones, with the likelihood of exclusive breastfeeding declining as age increases. This pattern is consistent with findings from several West African countries [131–133]. A possible explanation is that many mothers perceive breast milk alone as inadequate to meet the growing nutritional needs of older infants, prompting earlier introduction of complementary foods.
Maternal age was emerged as a significant predictor of exclusive breastfeeding. Mothers aged 35 years and older were three times more likely to exclusively breastfeed compared with those aged 15–24 years. This finding is in line with evidence from systematic reviews conducted in Brazil and Ghana [107,134]. One possible explanation is that younger mothers may perceive prolonged exclusive breastfeeding as affecting breast size or physical appearance, which could lead to earlier introduction of supplementary foods [135,136]. Furthermore, younger mothers may have limited awareness on the benefits of EBF, insufficient breastfeeding skills, or more frequent experiences of breastfeeding-related discomfort, all of which may contribute to lower exclusive breastfeeding practices. [137–139].
Maternal employment was a significant negative predictor of EBF. Employed mothers were 43% less likely to exclusively breastfeed their children compared with employed mothers. This finding is consistent with studies conducted across 19 developing countries [140], low and middle-income countries [141], and a SRMA from Ethiopia [14]. This could be because employed mothers return to work too early after birth due to short maternity leave, which can limit their ability to establish and sustain regular exclusive breastfeeding practices.
Conversely mothers from rural areas were 82% more likely to EBF their infants than urban residents. A similar result was reported by a previous SRMA conducted in Asia, Europe, and Africa [142]. This may be because rural mothers are predominantly housewives, are less likely to be engaged in formal employment, and tend to view breastfeeding as a natural maternal norm, unlike many of their urban counterpart. In addition, mothers living in rural areas are less exposed to and less familiar with breast milk substitutes promoted through media marketing compared with those in urban areas [143].
Mothers who delivered in a health facility were twice as likely to EBF their infants than home delivered mothers. This result was in line with studies done in Ethiopia, Tanzania and a systematic review and meta-analysis from Asia, Europe, and Africa [15,142,144]. This might be because women who delivered in a health facility could have a golden opportunity for nutrition education on the importance of EBF. In contrast, this finding contradicts with studies reported from Canada, Ireland and the UK, and Canada, which reported higher EBF rates among mothers who delivered at home [145]. This controversy could be explained by cultural differences among study participants and variations in awareness and understanding of exclusive breastfeeding practices [126,127].
Mothers who had normal delivery were twice as likely to EBF than those who delivered by cesarean section. This finding is consistent with a SRMA conducted in Iran [108]. This could be because of the nutrition counseling and breastfeeding support provided during labor and the immediate postpartum period, which encourage exclusive breastfeeding practices.
It was observed that mothers who received breastfeeding counseling were twice as likely to exclusively breastfeed their children compared with those who did not receive counseling, which was in accord with a SRMA performed by McFadden A et al. [146] and Ethiopia [147]. This may be due to the interactions with individual mothers during counselling, which enhance their knowledge, confidence, and decision-making regarding exclusive breastfeeding.
This study demonstrated that mothers who received support from their husband were almost three times more likely to exclusively breastfeed. This finding was corroborated by a SRMA conducted in Ghana and China [148,149]. This may be attributed to the emotional, physical, and practical support provided by husbands, which can strengthen maternal confidence, reduce stress, and ultimately enhance both the success and duration of exclusive breastfeeding. However, this finding contrasts with evidence from a systematic review and meta-analysis conducted by Sinha B. et a [150].
Mothers who attended postnatal care were more likely to EBF than their counterparts. This finding was in congruence with SRMA conducted in Ethiopia [151,152]. This may be because of the nutrition education and counseling received during the postnatal period, can help address breastfeeding difficulties, increase maternal confidence, and encourage social and family support, ultimately enabling mothers to maintain exclusive breastfeeding for six months.
Mothers who had antenatal care follow-up were more likely to initiate complementary feeding on time. This finding was consistent with a SRMA conducted in Ethiopia [112]. This could be because antenatal care visits provide an opportunity for mothers to receive information and counseling on appropriate complementary feeding practices from healthcare providers, thereby improving infant and young child feeding behaviors.
This study also showed that mothers who delivered at a health facility were more likely to initiate complementary feeding than home delivered mothers, which is in line with a SRMA in Ethiopia [153]. This could be attributed to the fact that mothers who gave birth in health institutions are more likely to receive counseling guidance from health professionals on appropriate child feeding practices.
It was also observed that children aged 18–23 months were more likely to receive a diet of good quality as per the recommendation compared to children aged 6–11 months. This finding was in line with studies done in Ethiopia, Ghana, and Uganda [154–157]. This may be because of the introduction of complementary feeding with a limited food item. Additionally, mothers may perceive that younger children have less developed digestive capacity for foods such as fruits, green leafy vegetables, and meat.
Mothers who received nutrition education through demonstration of complementary food preparation were more likely to achieve MAD as compared to their counterparts. This might be because such demonstration provides practical knowledge and skills on how to select, clean, and cook nutritious food preparation that meet the child’s nutritional needs. By observing and practicing food preparation during demonstrations, caregivers are more likely to adopt positive feeding behaviors, which enhances their confidence, promotes appropriate feeding practices, and supports the overall health and well-being of infants and young children.
This systematic review and meta-analysis have several limitations, including the exclusion of studies published in languages other than English. Furthermore, the high level of heterogeneity observed across the included studies may affect the reliability of the findings by introducing variability that can obscure true effects and potentially lead to misleading conclusions
Conclusions
The pooled prevalence of child feeding practices in Ethiopia remains below both national and global infant and young child feeding recommendations. These suboptimal feeding practice act as an early warning signal, indicating heightened risks of malnutrition, morbidity, and mortality. Under such conditions, achieving the Sustainable Development Goals and the national aspiration of becoming a lower-middle-income country becomes increasingly challenging.
Key determinants influencing infant feeding practices include the child’s age, maternal age, maternal employment status, place of residence, antenatal care attendance, place of delivery, postnatal care utilization, and exposure to complementary food preparation demonstrations.
Strengthening infant feeding practices therefore requires a multifaceted approach. Priority actions should include enhancing nutrition education through practical demonstrations, extending maternity leave to six months or establishing workplace breastfeeding and feeding corners, promoting consistent attendance of antenatal and postnatal care services, increasing facility-based deliveries, and tailoring interventions to maternal age and residential context. Equal emphasis should be placed on promoting age-appropriate feeding practices to ensure optimal growth and development.
Supporting information
S1 FileSupp information.(RAR)
S1 ChecklistPRISMA 2020 checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Organization WH. Infant and young child feeding: model chapter for textbooks for medical students and allied health professionals. World Health Organization. 2009.23905206 · pubmed ↗
- 2UNICEF. UNICEF advocacy strategy guidance for the prevention of overweight and obesity in children and adolescents. New York: UNICEF. 2020. https://www.unicef.org/media/92331/file/Advocacy-Guidance-Overweight-Prevention.pdf
- 3Micha R, Mannar V, Afshin A, Allemandi L, Baker P, Battersby J. 2020 global nutrition report: action on equity to end malnutrition. 2020. https://repository.mdx.ac.uk/item/89022
- 4Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walker N, Horton S, et al. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost?. Lancet. 2013;382(9890):452–77. doi: 10.1016/S 0140-6736(13)60996-4 23746776 · doi ↗ · pubmed ↗
- 5Black R, Victora C, Walker S, Bhutta Z, Christian P, de Onis M. Global nutrition report 2016: from promise to impact ending malnutrition by 2030. Washington DC: International Food Policy Research Institute. 2016. http://dx.doi.org/102499/9780896295841
- 6Ssentongo P, Ssentongo AE, Ba DM, Ericson JE, Na M, Gao X. Global, regional and national epidemiology and prevalence of child stunting, wasting and underweight in low-and middle-income countries, 2006–2018. Scientific Reports. 2021;11(1):5204.33664313 10.1038/s 41598-021-84302-w PMC 7933191 · doi ↗ · pubmed ↗
- 7Organization WH. Exclusive breastfeeding for six months best for babies everywhere. Geneva, Switzerland. 2011. https://pubmed.ncbi.nlm.nih.gov/25164443
- 8Fewtrell MS, Morgan JB, Duggan C, Gunnlaugsson G, Hibberd PL, Lucas A, et al. Optimal duration of exclusive breastfeeding: what is the evidence to support current recommendations?. Am J Clin Nutr. 2007;85(2):635S-638S. doi: 10.1093/ajcn/85.2.635S 17284769 · doi ↗ · pubmed ↗