Proctocolectomy with permanent ileostomy is associated with improved transplant-free survival in patients with PSC
Bregje Mol, Moyrha van Nieuwamerongen, Kim N. van Munster, Martti Färkkilä, Trine Folseraas, Sara K.V. Tjønnfjord, Johannes R. Hov, Kirsten Boberg, Mette Vesterhus, Kristin K. Jørgensen, Annika Bergquist, Jorn C. Goet, Annemarie C. de Vries, Adriaan J.P. van der Meer

TL;DR
Proctocolectomy with ileostomy is linked to better survival in PSC patients, suggesting gut-liver interactions influence disease progression.
Contribution
This study shows that proctocolectomy with ileostomy significantly reduces the risk of liver transplant or death in PSC patients.
Findings
Proctocolectomy with ileostomy reduced the risk of liver transplant or PSC-related death by 59%.
The protective effect was mainly due to a lower rate of liver failure.
Hemi- or subtotal colectomy had a smaller protective effect, while proctocolectomy with pouch showed no benefit.
Abstract
The gut–liver axis is believed to be crucial in the pathogenesis of primary sclerosing cholangitis (PSC). However, the impact of colectomy on liver disease progression is unclear. Our study estimated the effect of colectomy on PSC progression with correction for time dependency and established risk factors by pooling data from several cohorts across different countries. We analysed data from the International PSC Registry (IPSCR), comprising patients from Finland, The Netherlands, Norway, and Sweden. Primary endpoint was defined as liver transplantation (LT) or PSC-related death. Cox proportional hazards regression onto time-dependent colectomy status, with specification for extent, was performed with adjustment for sex, age at diagnosis, large or small duct PSC, features of autoimmune hepatitis, time-dependent inflammatory bowel disease (IBD) status, centre of inclusion, and country…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
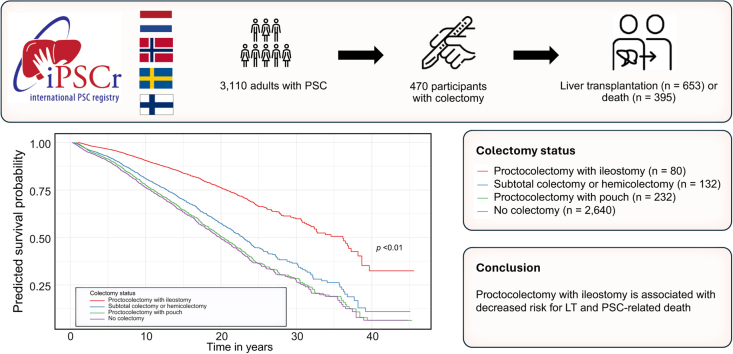 Figure 1
Figure 1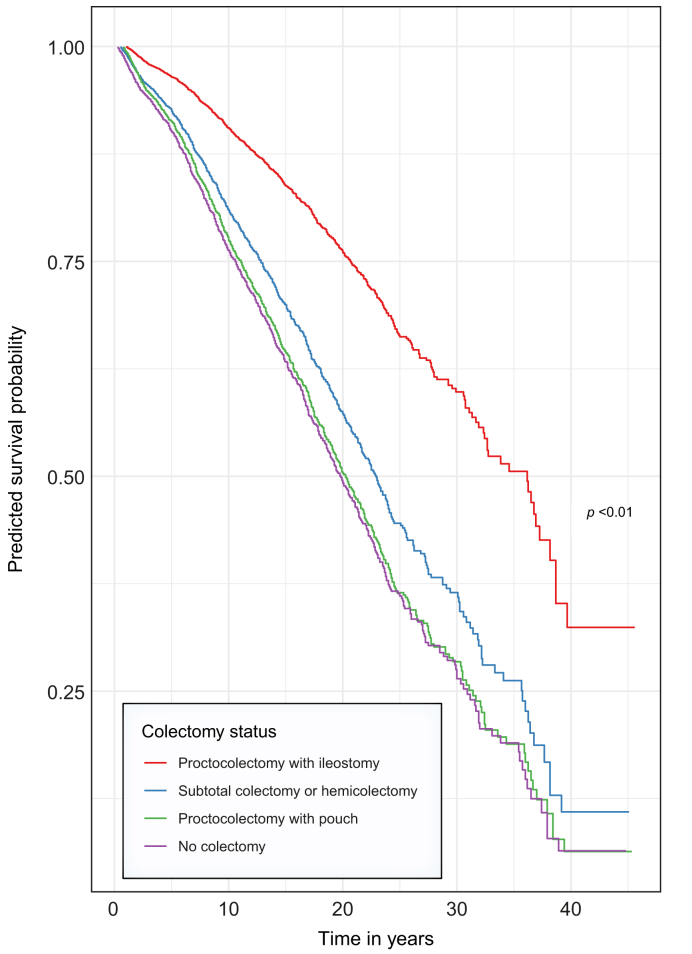 Figure 2
Figure 2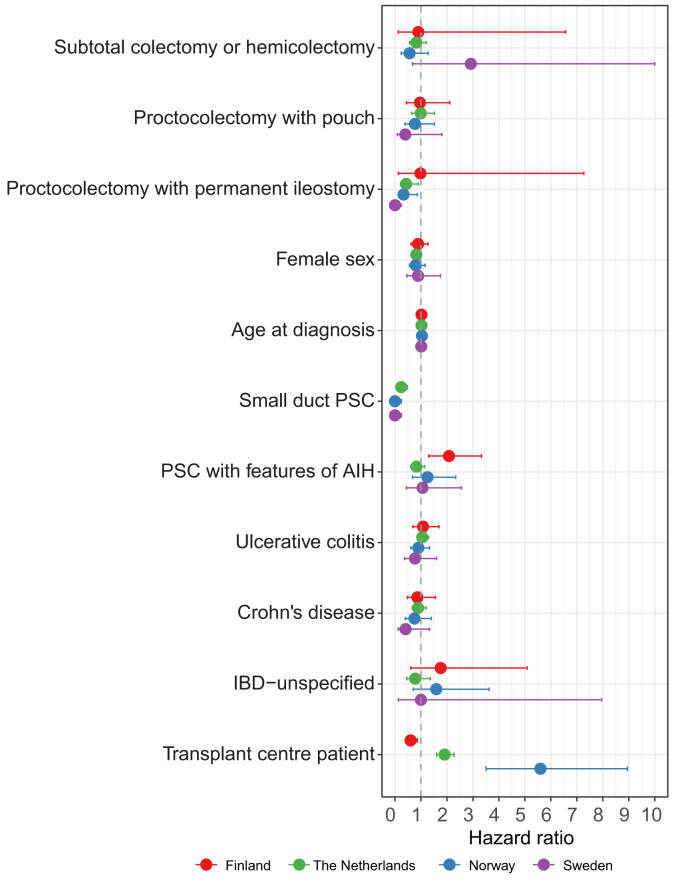 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Diseases and Immunity · Inflammatory Bowel Disease · Gallbladder and Bile Duct Disorders
Introduction
Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver disease characterised by inflammation and fibrosis of the bile ducts. The aetiology of PSC remains elusive, but its strong association with inflammatory bowel disease (IBD) suggests a significant interplay between the liver and the gut, in particular the colon.1 Currently, several hypotheses highlight the gut–liver axis as a crucial component in the pathophysiology of PSC, ranging from a leaky gut, aberrant gut-homing lymphocyte trafficking to colonic microbiota dysbiosis, or a combination thereof.[2], [3], [4]
Given the lack of a full understanding of the disease pathogenesis and the absence of targeted therapies, the therapeutic landscape for PSC remains challenging. In this context, colectomy emerges as a potential modulator of disease progression by interfering with the gut–liver axis. Colectomy in patients with PSC is not uncommon either to manage refractory IBD or as surgical treatment for high-grade dysplasia and colorectal carcinoma (CRC), a condition to which patients with PSC-IBD are particularly at risk.5 Limited evidence suggests more favourable outcomes after liver transplantation (LT) for patients who underwent colectomy.6 Moreover, patients who have undergone proctocolectomy with permanent ileostomy appear to have the most favourable graft outcomes.7 Limited evidence suggests a beneficial effect of colectomy on the disease course of PSC before, as well as a more favourable outcome after, LT.6^,^8 A meta-analysis by Ong et al.8 combined the limited available literature and failed to demonstrate an effect of colectomy on transplant-free survival. However, the existing evidence is fraught with limitations because these studies either depend on small sample sizes, may be confounded by unobserved risk factors, or did not account for time dependency in the effect of colectomy. Time dependency implies a change in risk over time, such as in patients before and after colectomy. The aim of our study was to estimate the effect of colectomy on the disease course of PSC by taking time dependency and established risk factors, such as sex, age, PSC type, and diagnosis of IBD, into account. To increase statistical power and enable comparisons across settings, we set up a collaborative international cohort study for this purpose.
Patients and methods
Study design and participants
This cohort study was based on the International PSC Registry (IPSCR), an international collaboration in which all participating parties maintain a uniform registry with a common core dataset. Data from Finland, The Netherlands, Norway, and Sweden were initially collected retrospectively and are updated prospectively on an annual basis from June 2023 onward. Cohort descriptions are provided in the Supplementary Files. All participants aged 18 years or older with a diagnosis of PSC according to EASL criteria were eligible.9
The study was approved by the institutional review boards of the UMC Utrecht (NL14614.041.06/METC06-267/E), Helsinki University Hospital (29 §/02.02.2024;dnro HUS/1566/2020), Oslo University Hospital (2015/2140), Haraldsplass Deaconess Hospital (2018/1425/REK vest), and Karolinska Institutet (Dnr 2020-01538).
Procedures and outcomes
Data regarding colectomy status were collected retrospectively at inclusion and updated prospectively by medical chart review. The date, indication, and extent of the colectomy was registered for each surgical intervention. Indication was defined as refractory IBD with or without neoplasia; dysplasia or carcinoma; other; or unestablished. Extent of colectomy was recorded as hemicolectomy; subtotal colectomy; or proctocolectomy. In case of a proctocolectomy, whether an ileal pouch-anal anastomosis or permanent ileostomy was constructed was recorded.
The primary outcome measure was transplant-free survival, defined as time from PSC diagnosis up to the last follow-up date, LT, or PSC*-*related death (death resulting from liver failure; hepatobiliary cancer; or other related causes, but excluding death resulting from CRC), with observation time censored at the last follow-up date, or other causes or death. CRC was excluded from the composite endpoints to avoid confounding by indication. In addition, transplant-free survival time was calculated up to LT or all-cause mortality. At inclusion, the date of PSC diagnosis was registered. Date and cause of death were registered retrospectively if applicable and prospectively updated every year. Date and indication for LT were registered retrospectively and prospectively updated every year. Indication for transplantation was defined as end-stage liver disease; recurrent cholangitis; symptoms, including intractable itch and fatigue; cholangiocarcinoma (CCA); hepatocellular carcinoma (HCC); biliary dysplasia; or unestablished.
To distinguish between outcomes driven by liver disease progression vs. occurrence of hepatobiliary cancer, two secondary endpoints were constructed. The first was defined as time from PSC diagnosis up to LT or death resulting from liver failure, with censoring at last follow-up or other causes of death. The second secondary endpoint was defined as the time from PSC diagnosis up to occurrence of hepatobiliary malignancy, censored for all other preceding events, or loss to follow-up. Occurrence of hepatobiliary malignancies (i.e. CCA, HCC, gallbladder carcinoma [GBC], pancreatic cancer, or unclear hepatobiliary malignancy), and CRC were registered retrospectively and prospectively updated every year.
The following data on potential confounders and effect modifiers based on previous literature were collected at study inclusion and updated annually by medical chart review: age at diagnosis; sex at birth; PSC type according to the International PSC Study Group (IPSCSG) definitions10 (i.e. large duct [LD], small duct [SD], or PSC with features of autoimmune hepatitis [AIH]), and concurrent diagnosis of IBD, including date and type (i.e. ulcerative colitis [UC], Crohn’s disease [CD], or IBD unspecified [IBD-u]).11
Centre of inclusion was included to indicate patients originating from transplant centres and to account for potential variation within the selected patient populations. Country of residence was also collected to adjust for country-specific effects.
Statistical analysis
Given that this was an observational study, formal sample size calculation was not performed. The study encompassed all eligible participants recorded in the registry, ensuring comprehensive analysis of the available data.
Continuous data with approximately normal distribution were expressed as means ± SD, whereas skewed data were expressed as medians with IQRs. Normality of distribution was assessed visually. Categorical variables were expressed as numbers with percentages. Pearson’s Chi-squared test was used to analyse categorical data. Independent t tests or Mann-Whitney U tests were used to analyse continuous data depending on whether data showed a normal or skewed distribution, respectively.
Transplant-free survival was estimated using the Kaplan–Meier method, and differences between countries were evaluated using the log-rank test. The effect of colectomy on the primary and secondary outcomes was determined via a Cox proportional hazards model using the coxph function from the survival package in R (R Foundation for Statistical Computing, Vienna, Austria).12 Events within the first year after colectomy were censored because of a presumed delayed effect. In addition, two sensitivity analyses were performed: in the first analysis, events occurring within 1 year after colectomy were assigned to the precolectomy period. The second analysis was performed without censoring events within 1 year after colectomy, assuming the possibility of a direct effect. In the multivariable model, the effect of colectomy was corrected for the following established risk factors: sex; age at diagnosis; PSC type; and IBD status. Inclusion in a transplant centre was added as a covariate to account for variation within the selected populations. Country was added as a covariate to account for possible country-specific effects.
To account for immortal time bias, both colectomy status and IBD status were included as time-dependent exposure variables by using the counting process approach to the analysis of survival time.13 This method stratifies the observation time over several data records, corresponding to time intervals with constant values of all covariates.14 The method of time-depending variables ensures that the accumulated risk in a specific risk group is adjusted for in the subsequent risk group. In case of multiple colonic surgical interventions, the time of exposure for each type of colectomy was calculated. If restorative surgery took place within 1 year after initial surgery, the type of colectomy after restoration was scored. By default, participants after proctocolectomy were coded as having no IBD. A sensitivity analysis was performed including only participants with a diagnosis of both PSC and IBD. A second sensitivity analysis was performed by including the indication for colectomy in an analysis in only participants after colectomy, retaining PSC disease duration as time axis. The rule of three was applied to estimate 95% CIs when no events were observed.15
Predicted survival probabilities from the final Cox proportional hazards model were used to generate predicted survival curves. The survfit function provided survival estimates with specified levels and mean values for continuous variables and were plotted by colectomy status using the ggplot2 package.16 The results of the multivariable models per country were visualized in a forest plot using the dotwhisker package.17 We considered p <0.05 to be statistically significant. IBM SPSS version 28.0 (IBM, Armonk, NY, USA) and R Studio 4.3.2 (RStudio, Inc. Boston, MA, USA) were used to conduct the statistical analyses.18^,^19
Results
Participant characteristics
In total, 3,110 participants were included; 1,341 from The Netherlands, 1,075 from Finland, 528 from Norway, and 166 from Sweden. Most were men (64%) with a mean age at diagnosis of 37 ± 15 years. The median calendar year of diagnosis was 2008 (IQR: 2001–2014). Of all participants, 46% were under the care of a transplant centre. Patients were diagnosed with LD PSC in 88% of cases and 75% of cases were diagnosed with IBD. Of the IBD cases, 17% were diagnosed after PSC diagnosis. The median follow-up time was 10 years, resulting in a total follow-up time of 32,236 patient-years. Participant characteristics stratified by country are presented in Table 1.Table 1. Participant characteristics stratified by country.Table 1IPSCR (N = 3,110)the Netherlands (N = 1,341)Finland (N = 1,075)Norway (N = 528)Sweden (N = 166)Male, n/N (%)1,974 /3,110 (64%)851/1,341 (64%)631/1,075 (59%)382/528 (72%)110/166 (66%)Age at diagnosis, mean (SD)/N37 (15)/ 3,10739 (15)/ 1,34136 (14)/ 1,07339 (16)/ 52834 (14)/ 165Calendar year of PSC diagnosis, median (IQR)/N2008 (2001-2014)/ 3,1092004 (1995-2008)/ 1,3412012 (2007-2017)/ 1,0752011 (2007-2017)/ 5282006 (2000-2010)/165Follow-up time, median (IQR)/N9 (4-15)/ 30879 (5-15)/ 13418 (4-14)/ 10737 (4-13)/ 50815 (11-20)/165Transplant centre inclusion, n/N (%)1,437/3,110 (46%)581/1,341 (43%)556/1,075 (52%)300/528 (57%)166/166 (100%)PSC type, n/N (%)Large duct2,739/3,091 (88%)1,133/1,325 (85%)984/1,075 (92%)485/528 (92%)137/163 (83%)Small duct88/3,091 (3%)79/1,325 (6%)-4/528 (1%)5/163 (3%)Auto-immune hepatitis264/3,091 (9%)113/1,325 (8%)91/1,075 (8%)39/528 (7%)21/163 (13%)IBD, n/N (%)None774/3,110 (25%)391/1,333 (29%)242/1,075 (23%)109/508 (21%)32/164 (19%)Ulcerative colitis1765/3,110 (57%)684/1,333 (51%)654/1,075 (61%)325/508 (62%)102/164 (62%)Crohn’s disease441/3,110 (14%)204/1,333 (15%)155/1,075 (14%)55/508 (10%)27/164 (16%)IBD-unspecified100/3,110 (3%)54/1,333 (4%)24/1,075 (2%)19/508 (4%)3/164 (2%)Colectomy∗, n/N (%)No colectomy2639/3,110 (85%)1154/1,341 (86%)909/1,075 (85%)438/528 (83%)138/166 (83%)Subtotal colectomy or hemicolectomy118/3,110 (4%)67/1,341 (5%)20/1,075 (2%)27/528 (5%)4/166 (2%)Proctocolectomy with pouch230/3,110 (7%)54/1,341 (4%)127/1,075 (12%)37/528 (7%)12/166 (12%)Proctocolectomy with permanent ileostomy80/3,110 (3%)25/1,341 (2%)18/1,075 (2%)25/528 (5%)12/166 (7%)Unknown43/3,110 (1%)41/1,341 (3%)1/1,075 (0.1%)1/528 (0.2%)-Participants characteristics of the IPSCR (International PSC Registry) stratified by country. SD = standard deviation. IQR = inter quartile range. PSC = primary sclerosing cholangitis. IBD = inflammatory bowel disease.Categorical data was analysed with Pearson’s chi-squared test, continuous data was analysed with the independent t-test in case of normal distribution or Mann-Whitney U test in case of skewed distribution.∗Colectomy status at the end of follow-up
Exposure
During follow-up, 470 (15%) participants underwent colectomy; 39 (8%) had a hemicolectomy, 93 (20%) a subtotal colectomy, 295 (63%) a proctocolectomy, and 43 (9%) a colectomy of unknown extent. Among 30 participants who initially underwent a partial (i.e. subtotal or hemi-)colectomy, subsequent surgical intervention necessitated conversion to proctocolectomy. Of the total of 321 proctocolectomies, 232 (72%) received a pouch reconstruction and 80 (25%) received a permanent ileostomy. Active IBD was the indication for initial colectomy in 224 (48%) of participants, active disease and neoplasia in 12 (3%), low-grade dysplasia in 47 (10%), high-grade dysplasia in 45 (10%), adenocarcinoma in 85 (18%), and, in 17 (3%) of the participants, colectomy was performed because of another indication. The indication was unknown in 33 (7%) participants.
Participant characteristics stratified by colectomy status are presented in Table 2. Participants who underwent a colectomy were more likely to have been diagnosed in significantly earlier years compared with those without colectomy (median 2006 vs. 2008, p <0.001). Consequently, follow-up duration differed significantly between participants with and without colectomy, with median follow-up periods of 12 years and 9 years (p <0.001), respectively. In addition, the distribution of IBD type differed significantly between participants with and without colectomy, with fewer participants without IBD (2% vs. 29%, p <0.001) and a higher proportion of UC (80% vs. 53%, p <0.001) in the group who underwent colectomy.Table 2. Participant characteristics stratified by colectomy status.Table 2. Participants with colectomy (N = 470)Participants without colectomy (N = 2,640)p-valueMale, n/N (%)307/470 (65%)1667/2,640 (63%)0.367Age at diagnosis, mean (SD)/N38 (15) /47037 (15)/ 2,6370.117Calendar year of PSC diagnosis, median (IQR)/N2006 (1998-2012)/ 4702008 (2002-2014)/ 2,639<0.001Follow-up time, median (IQR)/N12 (6-19)/ 4709 (4-14)/ 2,617<0.001Transplant centre inclusion, n/N (%)230/470 (49%)1207/2,640 (46%)0.198PSC type, n/N (%)Large duct427/469 (91%)2312/2,622 (88%)0.195Small duct10/469 (2%)78/2,622 (3%)Auto-immune hepatitis32/469 (7%)232/2,622 (9%)IBD type, n/N (%)None11/469 (2%)763/2,611 (29%)<0.001Ulcerative colitis378/469 (80%)1387/2,611 (53%)Crohn’s disease67/469 (14%)374/2,611 (14%)IBD-unspecified13/469 (3%)87/2,611 (3%)Participants characteristics for those who have undergone any type of colectomy compared to those without colectomy. SD = standard deviation. IQR = inter quartile range. PSC = primary sclerosing cholangitis. IBD = inflammatory bowel disease.Categorical data was analysed with Pearson’s chi-squared test, continuous data was analysed with the independent t-test in case of normal distribution or Mann-Whitney U test in case of skewed distribution.
Primary outcome
In total, we observed 395 (13%) deaths, of which 290 (73%) were PSC related. Cause of death was missing for 38 (10%) participants. Of the PSC-related deaths, 77 (27%) participants died from liver failure, 176 (61%) from hepatobiliary cancer, 20 (7%) from CRC, and 11 (4%) from other PSC-related causes. Of the 653 (21%) LTs observed, 237 (36%) were performed because of end-stage liver disease, 46 (7%) because of recurrent bacterial cholangitis, 28 (4%) because of itching or fatigue, 11 (2%) because of CCA, 7 (1%) because of HCC, and 48 (7%) because of biliary dysplasia. Indication for LT was missing for 274 (42%) participants.
The median transplant-free survival time was 22 (95% CI: 21–23) years. Transplant-free survival differed significantly between countries, with a median of 19 (95% CI: 17–20) years for The Netherlands, 23 (95% CI: 19–31) years for Norway, 29 (95% CI: 25–N/A) years for Finland, and 33 (95% CI: 24–N/A) years for Sweden. Survival curves stratified per country are presented in Fig. S1. Median time from colectomy to last follow-up date or endpoint was 5 (1–11) years.
Transplant-free survival was analysed based on colectomy status and specified by extent (i.e. hemicolectomy, subtotal colectomy, proctocolectomy with pouch, or proctocolectomy with permanent ileostomy). The results of the univariable and multivariable models are presented in Table 3. There was a clear separation in hazard rate of endpoints regarding extent of colectomy in univariable analyses, with lowest risk for proctocolectomy with ileostomy. For the endpoint LT or PSC-related death (excluding CRC), proctocolectomy with permanent ileostomy remained the most notable predictor (HR 0.41; 95%:CI: 0.24–0.71). Subtotal colectomy or hemicolectomy and proctocolectomy with pouch were not significantly associated with survival (HR 0.81; 95% CI: 0.58–1.12; and 1.00; 95% CI:0.73–1.38), respectively). Survival differed significantly between proctocolectomy with ileostomy and proctocolectomy with pouch (p = 0.003) and between proctocolectomy with ileostomy and subtotal colectomy or hemicolectomy (p = 0.04). In the multivariable model for the endpoint LT or all-cause mortality, adjusted for sex, age, PSC type, IBD type, country, and inclusion in a transplant centre, patients with proctocolectomy with ileostomy had a significantly decreased hazard compared with patients with intact colon (HR 0.48; 95% CI: 0.28–0.80)). Subtotal colectomy or hemicolectomy or proctocolectomy with pouch were not associated with a significantly decreased hazard (HR 1.13; 95% CI: 0.85–1.50; and 0.80; 95% CI: 0.59–1.08), respectively).Table 3. Multivariable model results for transplant-free survival, defined as liver transplantation or PSC-related death (excluding CRC) (A); and liver transplantation or all-cause mortality (B).Table 3A. Endpoint liver transplantation or PSC-related death (excluding CRC)Univariable HR (95% CI)Multivariable HR (95% CI)ColectomyNoneSubtotal colectomy or hemicolectomyProctocolectomy with pouch**Proctocolectomy with ileostomyReference1.18 (0.85-1.63)1.02 (0.76-1.36)0.62 (0.37-1.06)Reference0.81 (0.58-1.12)1.00 (0.73-1.38)0.41 (0.24-0.71)Female0.82 (0.72-0.95)0.79 (0.68-0.91)Age at diagnosis (per year)1.02 (1.02-1.03)1.02 (1.02-1.03)PSC typeLarge ductSmall ductFeatures of AIHReference0.26 (0.13-0.53)1.03 (0.82-1.29)Reference0.22 (0.11-0.45)1.07 (0.85-1.35)IBDNo IBDUlcerative colitisCrohn’s disease**IBD-unspecifiedReference0.98 (0.85-1.14)0.77 (0.62-0.97)0.91 (0.61-1.36)Reference1.01 (0.86-1.20)0.80 (0.63-1.01)0.96 (0.64-1.45)Countrythe NetherlandsFinlandNorway**SwedenReference0.43 (0.31-0.58)0.87 (0.74-1.04)0.41 (0.34-0.49)Reference0.59 (0.43-0.81)0.78 (0.65-0.93)0.36 (0.30-0.44)Transplant centre patient1.65 (1.44-1.88)1.80 (1.57-2.08)B. Endpoint liver transplantation or all-cause mortalityUnivariable HR (95% CI)Multivariable HR (95% CI)ColectomyNoneSubtotal colectomy or hemicolectomyProctocolectomy with pouch**Proctocolectomy with ileostomyReference1.73 (1.31-2.29)0.97 (0.74-1.28)0.68 (0.41-1.12)Reference1.13 (0.85-1.50)0.80 (0.59-1.08)0.48 (0.28-0.80)Female0.89 (0.78-1.02)0.83 (0.72-0.95)Age at diagnosis (per year)1.03 (1.03-1.04)1.03 (1.02-1.03)PSC typeLarge ductSmall ductFeatures of AIHReference1.48 (0.89-2.46)1.01 (0.81-1.26)Reference1.06 (0.63-1.77)1.15 (0.91-1.44)IBDNo IBDUlcerative colitisCrohn’s disease**IBD-unspecifiedReference0.80 (0.69-0.92)0.67 (0.54-0.83)0.79 (0.53-1.18)Reference0.75 (0.64-0.88)0.69 (0.55-0.86)0.62 (0.41-0.93)Countrythe NetherlandsFinlandNorway**SwedenReference0.21 (0.16-0.28)0.41 (0.35-0.49)0.20 (0.17-0.24)Reference0.26 (0.19-0.35)0.42 (0.35-0.50)0.20 (0.17-0.25)Transplant centre patient1.23 (1.08-1.39)1.33 (1.16-1.52)Univariable and multivariable outcomes of the Cox proportional hazards model for the outcomes (A) liver transplantation or all-cause mortality and (B) liver transplantation or PSC-related death (excluding CRC). The table summarized the hazard ratios (HR) and 95% confidence intervals (95%CI) for colectomy status, sex, age at diagnosis, PSC type, IBD status, country and centre of inclusion.
In line with previous literature, male sex, older age at diagnosis, and inclusion in a transplant centre were associated with reduced survival outcomes. Among the IBD diagnoses, these were associated in the multivariable analysis with reduced HRs for the endpoint LT or all-cause mortality but not for LT or PSC-related death. The predicted survival curve for a 37-year-old male patient with LD PSC and UC in The Netherlands, modelled as though the participant had undergone a specific type of colectomy at the beginning and maintained that status throughout the follow-up period, is presented in Fig. 1. The predicted median survival time for those with proctocolectomy with ileostomy was 35 years compared with 19 years for those without colectomy.Fig. 1. Predicted survival probability for a 37-year-old man with LD PSC and UC from The Netherlands for the endpoint LT or PSC-related death (excluding CRC).The Kaplan–Meier curves demonstrate the estimated survival probabilities over time for participants without colectomy (red line), participants after subtotal colectomy or hemicolectomy (green line), participants after proctocolectomy with pouch (blue line), and participants after proctocolectomy with ileostomy (purple line). Survival probabilities (y-axis) are modelled under the assumption that a participant maintains their colectomy status throughout their follow-up period (x-axis; years since PSC diagnosis). CRC colorectal cancer; LD, large duct; LT, liver transplantation; PSC, primary sclerosing cholangitis; UC, ulcerative colitis.Fig. 1
The model was also applied to each country individually. The results of the individual models are presented in Table S1 and depicted in a forest plot in Fig. 2. Predicted survival curves are presented per country in Fig. S2. Despite some variation between countries, a consistent beneficial effect was estimated in the association between proctocolectomy with permanent ileostomy and transplant-free survival in three out of four countries. The HRs were 0.43 (95% CI: 0.21–0.90) in The Netherlands, 0.98 (95% CI: 0.13–7.27) in Finland, 0.33 (95% CI: 0.13–0.86) in Norway, and 0.00 (95% CI: 0.00–0.25) in Sweden, the latter resulting from no events under 137 person-years in the proctocolectomy with permanent ileostomy group.Fig. 2. Results of the multivariable models stratified per country.The forest plot illustrates the outcomes of the multivariable model for the endpoint LT or PSC-related death (excluding CRC) per country. The variables included in the model are listed on the y-axis, the dots on the x-axis represent the HR for every variable from the country-specific model, including whiskers presenting the 95% CIs. The outcomes for the Finnish model are in red, the outcomes for the model from The Netherlands are in green, the outcomes for the Norwegian model are in blue, and the outcomes for the Swedish model are in purple. The dotted line depicts an HR of 1. AIH, autoimmune hepatitis; CRC colorectal cancer; HR, hazard ratio; IBD, inflammatory bowel disease; LT, liver transplantation; PSC, primary sclerosing cholangitis.Fig. 2
Sensitivity analysis
First, we performed two sensitivity analyses to test the effect of the presumed delayed effect of colectomy of 1 year. We started by modelling a delay of 1 year, which implicates that events within the first year after colectomy were assigned to the precolectomy period (Table S2). The adjusted HRs were 0.91 (95% CI: 0.67–1.25) for subtotal colectomy or hemicolectomy, 1.09 (95% CI: 0.81–1.48) for proctocolectomy with pouch, and 0.47 (95% CI: 0.28–0.79) for proctocolectomy with ileostomy. We also computed a model without censoring of events within 1 year after colectomy. The adjusted HRs were 0.94 (95% CI: 0.69–1.27) for subtotal colectomy or hemicolectomy, 1.09 (95% CI: 0.81–1.49) for proctocolectomy with pouch, and 0.50 (95% CI: 0.30–0.83) for proctocolectomy with ileostomy.
Second, we performed a sensitivity analysis including only participants with a diagnosis of both PSC and IBD (Table S3). Compared with the analysis including all participants, the effect of colectomy was more pronounced for all subtypes. The adjusted HRs were 0.76 (95% CI: 0.53–1.09) for subtotal colectomy or hemicolectomy, 0.55 (95% CI: 0.24–1.27) for proctocolectomy with pouch, and 0.24 (95% CI: 0.09–0.61) for proctocolectomy with ileostomy.
Third, we performed a sensitivity analysis on two secondary endpoints to distinguish between outcomes driven by the progression of liver disease vs. hepatobiliary cancer. In the first analysis, which focused on the liver-specific outcome (Table S4A), the adjusted HRs were 0.65 (95% CI: 0.43–0.97) for subtotal colectomy or hemicolectomy, 0.75 (95% CI: 0.50–1.11) for proctocolectomy with pouch, and 0.24 (95% CI: 0.10–0.53) for proctocolectomy with ileostomy. The second analysis focused on occurrence of hepatobiliary malignancies (Table S4B). In total, we observed 202 (7%) cases of CCA, 34 (1%) of GBC, 38 (1%) of HCC, 5 (0.2%) of pancreatic cancer, and 1 (0.05%) case of hepatobiliary malignancy of unclear origin. The adjusted HRs were 1.26 (95% CI: 0.75–2.13) for subtotal colectomy or hemicolectomy, 1.62 (95% CI: 0.96–2.75) for proctocolectomy with pouch, and 1.17 (95% CI: 0.60–2.29) for proctocolectomy with ileostomy.
Lastly, a sensitivity analysis in participants after colectomy was performed to assess the effect of surgical indication. No significant effect of surgical indication was observed (Table S5). However, the HR for participants after proctocolectomy with pouch was significantly increased compared with those after proctocolectomy with ileostomy (HR 2.01; 95% CI: 1.04–3.88).
Discussion
Our study assesses the effect of colectomy on the disease course of PSC in an international cohort, accounting for time dependency and established risk factors. Our findings indicate that proctocolectomy with permanent ileostomy is associated with a decreased risk of LT and PSC-related death. This effect was mainly associated with postponement of LT and death from liver failure, as shown by the analyses of the secondary outcomes. In the subset of participants with a diagnosis of both PSC and IBD at any time during their follow-up, the effect of colectomy was even more pronounced for all subtypes. Surgical indication did not appear to affect transplant-free survival in those after colectomy. Three additional sensitivity-analysis outcomes also added robustness to the findings.
To date, most studies have concentrated on the effect of colectomy on outcomes following LT, whereas limited evidence exists regarding its effect on disease progression in the pretransplant phase. Ong et al.8 evaluated all available evidence on PSC progression and transplant-free survival in patients who underwent colectomy. In their systematic review, no clear effect on solid clinical endpoints, such as LT or mortality, was found. The conclusions of the largest study included in this systematic review, comprising almost 20,000 patient-years follow-up, are partly in line with our findings. The authors reported a significant association between participants treated with colectomy before PSC diagnosis and a decreased risk of LT and death, however, this effect was not found when colectomy was performed after PSC diagnosis.20 Given that the study by Nordenvall et al.20 was based on Swedish healthcare registers, case verification to ensure minimal case omission and misdiagnosis could not be performed. Moreover, detailed clinical information was not available to correct for PSC type, or stratify for different types of colectomy. Furthermore, the other included studies were based on small sample sizes and their statistical analyses did not correct for a time-depending effect of colectomy.
A few studies have been published describing the effect of colectomy on post-transplant outcomes. A meta-analysis of the report by Steenstraten et al.6 demonstrated a significant beneficial effect of colectomy before LT on the risk of recurrent PSC (HR 0.65; 95% CI: 0.42–0.99). In addition, studies from Trivedi et al.7 and Matar et al.21 included details regarding the extent and type of colectomy and demonstrated a beneficial effect of proctocolectomy with permanent ileostomy compared with proctocolectomy with pouch reconstruction on PSC recurrence rates. The study by Schabl et al.22 could not confirm the beneficial effect of ileostomy, although this analysis was likely underpowered, given that it included only nine participants with an ileostomy.
The strong association between proctocolectomy with permanent ileostomy and transplant-free survival could be explained by various hypotheses. Inflammation in the remaining colon or pouch could lead to persistent translocation of pathogens according to the leaky gut hypothesis and ongoing gut lymphocyte homing in the liver. Unfortunately, data regarding pouchitis were not available in our database. PSC is a strong risk factor for pouchitis.23 Following pouch reconstruction, the mucosa and microbiome of the pouch change significantly and adapt to a more colon-like phenotype.24^,^25 This transformation does not occur in ileal mucosa after ileostomy and appears inherent to stasis in the pouch. Morphological alterations are most predominant in those with pouchitis compared with normal pouches and might be dependent on the microbiota composition.23^,^26 Moreover, pouchitis does not occur before exposure to faecal contents, underscoring the putative role of the microbiota.
Our findings contribute to our understanding of the aetiology of PSC. The gut–liver axis appears to have a role in the pathophysiology of PSC and deserves focus as therapeutic target for PSC management. Therapeutic strategies, such as faecal microbiota transplantation (FMT), could hold promise in modulating gut microbiota and, as a result, could modify PSC progression. Given the potential complications associated with pouch reconstruction in patients with PSC and the beneficial long-term outcomes associated with ileostomy, it might be prudent to consider proctocolectomy with permanent ileostomy when colectomy is indicated. Quality of life (QoL) studies in patients with ileostomy are limited, but available evidence suggests that QoL outcomes are not substantially different between those with pouch or ileostomy.27 This consideration should be discussed with patients with PSC when making surgical decisions.
Our study presents the largest cohort to date describing the effect of colectomy on disease progression of PSC, a situation that cannot be studied in a randomised controlled fashion. It demonstrates the merits of mining data from our large uniform EASL-funded IPSCR, enabling detailed clinical data to be included for the first time to correct for established risk factors and stratification for colectomy extent, as well as correction for the time-dependent effect of colectomy.
Several limitations must be addressed. Given our observational study design, we cannot rule out unknown or overlooked confounders that might influence our outcomes. The effect of colectomy was similar among cohorts in three out of four countries. Proctocolectomy with permanent ileostomy showed no apparent benefit in Finland, likely because of local guidelines reserving ileostomy for pouch failure or technical impossibility of pouch reconstruction. It might be that, because of a high inflammatory burden after pouch failure, the effect of ileostomy was limited in this patient population. Moreover, we observed heterogeneity across countries regarding overall survival and effect of covariates, especially for the effect of participants under care in a transplantation centre. This is most likely attributable to patient selection and national practice guidelines. Although the amount of missing data overall was small, the cause of death and indication for LT were missing in a substantial percentage of participants. These were mostly participants in the Dutch population-based cohort, for whom data could not be retrieved because of GDPR regulations. Moreover, data completeness might have been impacted by the retrospective nature of data collection. The estimated effect of colectomy was similar for the endpoint LT or all-cause mortality and LT and PSC-related death (excluding CRC). Therefore, the risk of informative censoring in this selection of participants is expected to be low. Prognostic markers of liver disease severity were not available for all participants at time of PSC diagnosis and, therefore, were not included in the analyses.
In conclusion, our data indicate a beneficial effect of proctocolectomy with permanent ileostomy on liver disease progression in patients with PSC-IBD. These findings contribute to our understanding of the pathogenesis of PSC, could fuel novel therapeutic strategies, and call for reconsideration in counselling patients awaiting proctocolectomy.
Abbreviations
AIH, autoimmune hepatitis; CCA, cholangiocarcinoma; CD, Crohn’s disease; CRC, colorectal carcinoma; FMT, faecal microbiota transplantation; GBC, gallbladder cancer; HCC, Hepatocellular carcinoma; HR, hazard ratio; IBD, inflammatory bowel disease; IBD-U, inflammatory bowel disease – unspecified; IPSCSG, International PSC Study Group; IPSCR, International PSC Registry; LD, large duct; LT, liver transplantation; PSC, primary sclerosing cholangitis; QoL, quality of life; SD, small duct; UC, ulcerative colitis.
Authors’ contributions
Conceived the idea for this study: BM, KM, JB, CP. Data collection: BM, MN, KM, MF, TF, ST, JH, KB, MV, KJ, AB, AV, AM, RW, AI, CP. Verification of underlying data: BM, MN. Statistical analyses: BM, MN, JB. All authors were involved in critical revision of the manuscript for important intellectual content. All authors had full access to all the data and accepted responsibility to submit for publication.
Data availability
Data are available upon reasonable request from the corresponding author. Deidentified data are available from the corresponding author after approval of a proposal by the IPSCR steering committee and with signed data access agreement.
Financial support
The study was funded by a registry grant from 10.13039/501100009253EASL, the Dutch Organisation for 10.13039/100005622Health Research and Development (10.13039/501100001826ZonMw, grant number:836041010), and a grant from Gilead. The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Conflicts of interest
The authors have no financial or personal relationships to declare that are relevant to this publication.
Please refer to the accompanying ICMJE disclosure forms for further details.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1van Munster K.N.Bergquist A.Ponsioen C.Y.Inflammatory bowel disease and primary sclerosing cholangitis: one disease or two?J Hepatol 8020241551683794045310.1016/j.jhep.2023.09.031 · doi ↗ · pubmed ↗
- 2Berg R.D.Bacterial translocation from the gastrointestinal tract Paul P.S.Francis D.H.Mechanisms in the pathogenesis of enteric diseases 21999 Springer US Boston 1130
- 3Grant A.J.Lalor P.F.Salmi M.Homing of mucosal lymphocytes to the liver in the pathogenesis of hepatic complications of inflammatory bowel disease Lancet 35920021501571180927510.1016/S 0140-6736(02)07374-9 · doi ↗ · pubmed ↗
- 4Hov J.R.Karlsen T.H.The microbiota and the gut-liver axis in primary sclerosing cholangitis Nat Rev Gastroenterol Hepatol 2020231351543635215710.1038/s 41575-022-00690-y · doi ↗ · pubmed ↗
- 5Zheng H.H.Jiang X.L.Increased risk of colorectal neoplasia in patients with primary sclerosing cholangitis and inflammatory bowel disease: a meta-analysis of 16 observational studies Eur J Gastroenterol Hepatol 2820163833902693880510.1097/MEG.0000000000000576 · doi ↗ · pubmed ↗
- 6Steenstraten I.C.Sebib Korkmaz K.Trivedi P.J.Systematic review with meta-analysis: risk factors for recurrent primary sclerosing cholangitis after liver transplantation Aliment Pharmacol Ther 4920196366433074072310.1111/apt.15148 PMC 6593422 · doi ↗ · pubmed ↗
- 7Trivedi P.J.Reece J.Laing R.W.The impact of ileal pouch-anal anastomosis on graft survival following liver transplantation for primary sclerosing cholangitis Aliment Pharmacol Ther 4820183223322988225210.1111/apt.14828 · doi ↗ · pubmed ↗
- 8Ong J.Bath M.F.Swift C.Does colectomy affect the progression of primary sclerosing cholangitis? A systematic review and meta-analysis Gastroenterol Hepatol Bed Bench 11201827728330425805 PMC 6204254 · pubmed ↗