Comparison of the Effects of Sevoflurane and Isoflurane During Liver Transplant Surgery on the Short-Term Cardiac, Hepatic, and Renal Outcome: A Randomized Clinical Trial
Mohammadreza Moshari, Sadaf Tahery, Mastaneh Dahi Taleghani, Shide Dabir, Maryam Vosoughian, Soudeh Tabashi, Mohsen Ariannik, Firoozeh Madadi

TL;DR
This study compared isoflurane and sevoflurane during liver transplants and found no significant differences in short-term cardiac, liver, or kidney outcomes.
Contribution
The study provides new clinical evidence on the comparative effects of two volatile anesthetics in liver transplant surgery.
Findings
No significant differences were found in postoperative liver and kidney function between isoflurane and sevoflurane groups.
Sevoflurane was associated with higher intraoperative blood product requirements compared to isoflurane.
Both anesthetics showed similar effects on cardiac biomarkers and hemodynamic parameters.
Abstract
Liver transplantation is frequently complicated by ischemia-reperfusion injury (IRI), which may impair hepatic, renal, and cardiac function. Volatile anesthetics such as isoflurane and sevoflurane are believed to mitigate this injury. This study aimed to compare their effects on short-term organ outcomes in deceased donor liver transplant recipients. In this study, 70 liver transplantation candidates at Taleghani Hospital in Tehran were enrolled after obtaining informed consent, and various variables were assessed before, during, and at two intervals immediately after surgery and one week post-operation. Patients were randomly allocated to receive either isoflurane or sevoflurane for anesthesia maintenance using the sealed opaque envelope technique for allocation concealment. Randomization was performed by a study nurse not involved in patient care using computer-generated random…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
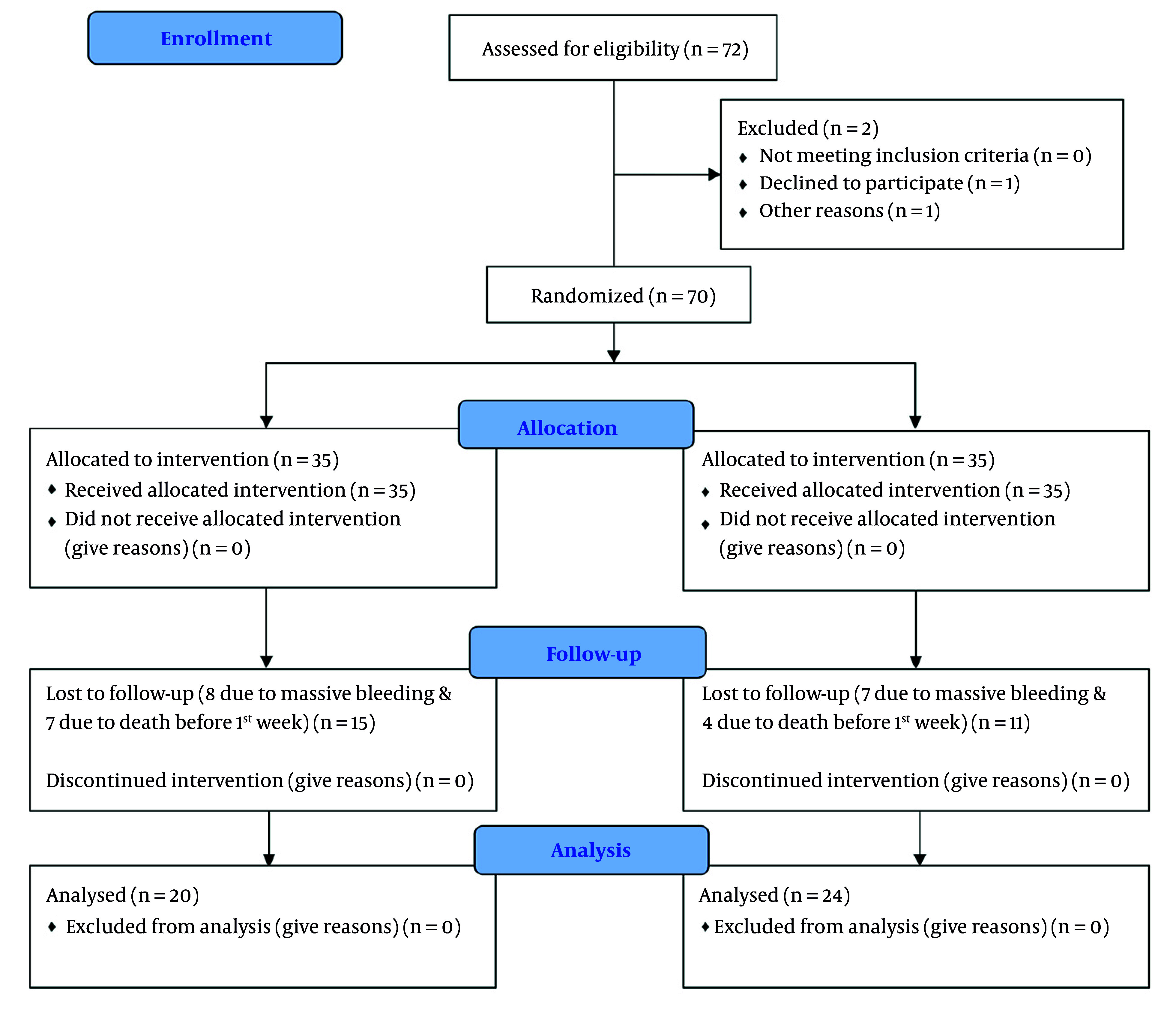 Figure 1
Figure 1| Variables | Isoflurane | Sevoflurane | P-Value |
|---|---|---|---|
|
| 10 males | 11 males | 0.402 |
|
| 44.35 ± 12.014 | 44.25 ± 13.829 | 0.980 |
|
| 23.46 ± 3.182 | 24.93 ± 4.50 | 0.185 |
|
| 23.55 ± 4.019 | 24.04 ± 6.597 | 0.763 |
|
| 38.15 ± 11.940 | 43.88 ± 14.128 | 0.159 |
|
| 1373.50 ± 114.812 | 1402.71 ± 292.288 | 0.677 |
| Laboratory Data/Sampling Time | Isoflurane | Sevoflurane | P-Value |
|---|---|---|---|
|
| |||
| Preoperative | 1.10 ± 0.79 | 1.08 ± 0.81 | 0.947 |
| 6 hrs postop | 1.13 ± 0.71 | 1.09 ± 0.73 | 0.865 |
| 7 d postop | 1.12 ± 0.55 | 1.01 ± 0.50 | 0.486 |
|
| |||
| Preoperative | 145.80 ± 386.72 | 232.46 ± 397.61 | 0.470 |
| 6 hrs postop | 458.20 ± 815.91 | 696.38 ± 864.17 | 0.356 |
| 7 d postop | 221.25 ± 362.13 | 244.29 ± 309.80 | 0.821 |
|
| |||
| Preoperative | 287.95 ± 995.57 | 309.75 ± 484.05 | 0.925 |
| 6 hrs postop | 511.40 ± 910.26 | 698.33 ± 635.82 | 9.428 |
| 7 d postop | 161.05 ± 359.104 | 944.54 ± 3919.79 | 0.379 |
|
| |||
| Preoperative | 9.86 ± 26.26.18 | 9.10 ± 10.74 | 0.898 |
| 6 hrs postop | 10.25 ± 27.30 | 34.28 ± 124.61 | 0.403 |
| 7 d postop | 3.33 ± 3.24 | 4.35 ± 5.10 | 0.442 |
|
| |||
| Preoperative | 0.18 ± 0.60 | 0.01 ± 0.01 | 0.228 |
| 6 hrs postop | 0.05 ± 0.06 | 0.10 ± 0.19 | 0.237 |
| 7 d postop | 0.09 ± 0.10 | 0.09 ± 0.12 | 0.965 |
|
| |||
| Preoperative | 25.13 ± 20.52 | 23.90 ± 29.17 | 0.875 |
| 6 hrs postop | 27.38 ± 18.27 | 40.77 ± 40.97 | 0.159 |
| 7 d postop | 28.94 ± 23.39 | 37.89 ± 39.77 | 0.378 |
| Parameters/Surgery Phases | Isoflurane | Sevoflurane | P-Value |
|---|---|---|---|
|
| |||
| Preanhepatic | 968.00 ± 707.595 | 689.58 ± 556.257 | 0.151 |
| Anhepatic | 381.00 ± 454.346 | 281.25 ± 343.832 | 0.412 |
| Reperfusion | 935.00 ± 568.493 | 775.00 ± 482.070 | 0.318 |
|
| |||
| Preanhepatic | 35.0 | 50.0 | 0.244 |
| Anhepatic | 85.0 | 91.7 | 0.411 |
| Reperfusion | 55.0 | 79.2 | 0.082 |
|
| |||
| Preanhepatic | 6.180 ± 1.788 | 6.10 ± 2.147 | 0.895 |
| Anhepatic | 5.035 ± 1.756 | 5.60 ± 2.512 | 0.395 |
| Reperfusion | 8.455 ± 2.863 | 8.44 ± 3.195 | 0.989 |
|
| |||
| Preanhepatic | 1012.10 ± 400.20 | 907.00 ± 335.27 | 0.348 |
| Anhepatic | 1137.25 ± 625.03 | 1011.00 ± 511.19 | 0.465 |
| Reperfusion | 760.30 ± 304.369 | 782.75 ± 312.05 | 0.811 |
|
| |||
| Preanhepatic | 3.915 ± 1.030 | 4.10 ± 2.28 | 0.740 |
| Anhepatic | 3.050 ± 0.915 | 3.86 ± 1.83 | 0.065 |
| Reperfusion | 4.935 ± 1.588 | 4.67 ± 1.65 | 0.593 |
|
| |||
| Preanhepatic | 52.00 ± 23.02 | 69.79 ± 45.43 | 0.102 |
| Anhepatic | 81.75 ± 52.84 | 108.33 ± 54.50 | 0.110 |
| Reperfusion | 44.75 ± 26.13 | 62.50 ± 44.84 | 0.126 |
| Variables | Isoflurane | Sevoflurane | P-Value |
|---|---|---|---|
|
| 920.00 ± 501.157 | 1228.33 ± 666.664 | 0.096 |
|
| 1.75 ± 1.713 | 2.88 ± 1.727 | 0.037 |
|
| 1.25 ± 1.682 | 2.42 ± 1.692 | 0.028 |
|
| 4225.00 ± 1129.450 | 4182.50 ± 1071.493 | 0.911 |
|
| 82.50 ± 81.556 | 66.67 ± 80.307 | 0.522 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Transplantation Techniques and Outcomes · Cardiac Ischemia and Reperfusion · Cardiac and Coronary Surgery Techniques
1. Background
Liver transplantation is the definitive treatment for end-stage liver disease and has greatly improved in recent decades due to advances in surgical techniques, organ preservation, and immunosuppressive therapy (1, 2). Despite these advances, ischemia-reperfusion injury (IRI) remains a significant challenge, contributing to graft dysfunction and failure post-transplantation (3-5). Ischemia-reperfusion injury occurs when blood supply returns to the liver after a period of ischemia, triggering a cascade of inflammatory responses, oxidative stress, and cellular damage that extend beyond the liver to affect other organs, including the heart and kidneys (6-9).
The pathophysiology of IRI involves complex molecular mechanisms. Oxygen deprivation during ischemia leads to anaerobic glycolysis, acidosis, and cellular ion imbalances. Upon reperfusion, the sudden restoration of oxygen supply causes overproduction of reactive oxygen species (ROS), primarily by Kupffer cells and neutrophils. Reactive oxygen species initiate lipid peroxidation, mitochondrial damage, and activation of pro-inflammatory pathways, including cytokine release, inflammasome activation, and pyroptosis (6, 10-13). This cascade not only worsens hepatic injury but can propagate systemic inflammation and multiorgan dysfunction. Factors such as hepatic steatosis further increase susceptibility to IRI due to impaired microcirculation and reduced antioxidant capacity (14-16).
Strategies to mitigate IRI include optimal perfusion techniques, preconditioning, and pharmacologic interventions (17, 18). Among these, the choice of anesthetic agents during transplantation has attracted attention due to their immunomodulatory and organ-protective effects. Inhalational anesthetics such as isoflurane and sevoflurane have shown potential in attenuating IRI. Isoflurane has demonstrated anti-inflammatory effects and the ability to modulate apoptotic pathways via NF-κB and AKT signaling (7, 19). Sevoflurane, on the other hand, may confer hepatoprotective benefits by reducing oxidative stress, regulating the Nrf2/HO-1 pathway, and limiting cellular apoptosis (20-24).
However, clinical findings comparing these two agents have been mixed. Some studies report reduced hepatic injury and better postoperative outcomes with sevoflurane (22, 25), while others find no significant difference or even favor isoflurane in terms of intraoperative hemodynamic stability or bleeding (19, 26, 27). Additionally, potential side effects such as nephrotoxicity linked to fluoride metabolites from sevoflurane metabolism have raised concerns (20, 21, 23).
2. Objectives
Given this background, the optimal choice of volatile anesthetic in liver transplant surgery remains controversial. This study aims to directly compare the effects of isoflurane and sevoflurane on hepatic, renal, and cardiac outcomes during and after deceased donor liver transplantation. By analyzing intraoperative parameters, biochemical markers, and postoperative complications, the study seeks to determine whether either anesthetic provides superior organ protection. The goal is to provide evidence-based guidance for anesthetic selection in deceased donor liver transplant patients, potentially contributing to improved short-term outcomes and better graft preservation.
3. Methods
3.1. Trial Design and Setting
We conducted a single-center, prospective, parallel-group, randomized clinical trial at the Organ Transplant Surgery Department of Ayatollah Taleghani Hospital (Tehran, Iran) between December 2024 and April 2025. The study protocol was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (IR.SBMU.MSP.REC.1403.160) and registered at the Iranian Registry of Clinical Trials before patient enrollment (IRCT20240909062992N1, registration date: 2024-10-22). All participants provided written informed consent before enrollment.
3.2. Participants
Adult patients (≥ 18 years) listed for orthotopic liver transplantation from deceased donor were screened. Inclusion criteria: Eligibility for liver transplant; ability to consent. Exclusion criteria: Emergency surgery; cardiopulmonary resuscitation during anesthesia; failure to extubate within 24 h; massive intraoperative hemorrhage (> 1 h anhepatic phase or excessive bleeding); death within 7 days.
3.3. Randomization and Blinding
After eligibility confirmation and consent, 70 patients were randomized 1:1 to receive isoflurane or sevoflurane. A computer-generated random sequence (block size = 4) was prepared by an independent statistician. Allocation concealment was maintained using sequentially numbered, opaque, sealed envelopes. An anesthesia technician, not involved in data collection, opened the envelope immediately before induction. Care providers and outcome assessors remained blinded to group assignment; anesthesiologists could not be blinded due to the nature of the intervention but did not participate in data collection.
3.4. Interventions
Anesthetic induction (both groups): Midazolam 0.05 mg/kg, fentanyl 2 - 3 µg/kg, propofol 1.5 - 2 mg/kg, lidocaine 1 mg/kg, cisatracurium 0.15 mg/kg. Maintenance: Isoflurane group: Isoflurane 1.0 - 1.5 MAC Sevoflurane group: Sevoflurane 1.7 - 2.6 MAC Bispectral Index (BIS) was kept between 40 and 60. Intraoperative monitoring included invasive arterial pressure (LiDCO device), central venous pressure, heart rate, urine output, fluid balance, and inotrope use.
3.5. Outcome Measures
Primary outcome: Laboratory markers [alanine aminotransferase (ALT), aspartate aminotransferase (AST), bilirubin, creatinine, troponin, C-reactive protein (CRP)] measured preoperatively, 6 hours post-reperfusion, and on postoperative day 7. Secondary outcomes: Hemodynamic parameters (cardiac output, systemic vascular resistance) and urine output measured at preanhepatic, anhepatic, and reperfusion phases · Inotrope requirement (yes/no) during each phase. Intraoperative transfusion volume (packed red blood cells and fresh frozen plasma). Adverse events (bleeding, arrhythmias, acute kidney injury) were recorded throughout hospitalization.
3.6. Sample Size
The sample size was calculated based on the primary outcome, defined as the postoperative peak serum ALT level as a surrogate marker of hepatic ischemia–reperfusion injury. Based on previously published studies in liver transplantation and pilot institutional data, a clinically meaningful difference of 250 U/L in peak postoperative ALT between the isoflurane and sevoflurane groups was assumed, with an estimated standard deviation of 300 U/L. Using a two-sided independent samples t-test, an alpha level of 0.05, and a statistical power of 80%, a minimum of 32 patients per group was required to detect this difference. To account for potential dropouts, protocol violations, and early postoperative exclusions inherent to liver transplantation studies, the target enrollment was increased by approximately 10%, resulting in a planned sample size of 35 patients per group (70 patients in total).
3.7. Statistical Analysis
Data were analyzed using SPSS v.24. Continuous variables were tested for normality (Kolmogorov-Smirnov) and compared using Student’s t-test or Mann-Whitney U test as appropriate. Categorical variables were compared using χ² test or Fisher’s exact test. Repeated measures (laboratory values across time points) were analyzed by two-way ANOVA with Bonferroni correction. A P-value < 0.05 was considered statistically significant. Analyses followed the intention-to-treat principle. Data are presented as mean ± SD or median (interquartile range) as appropriate. P-values are unadjusted; no correction for multiple comparisons was applied because all biochemical outcomes except transfusion requirements were considered exploratory/secondary.
4. Results
A total of 70 patients were initially enrolled and randomized into two groups. Following the exclusion of patients based on predefined criteria, 44 participants completed the study protocol — 20 in the isoflurane group and 24 in the sevoflurane group (Figure 1). Baseline demographic and clinical characteristics, including age, sex, MELD score, and etiology of liver disease, were similar between the two groups, with no statistically significant differences (Table 1).
Flow diagram of patient enrollment in the study
Regarding the primary outcomes, there were no significant differences in postoperative laboratory markers between the groups. Serum levels of ALT, AST, total bilirubin, creatinine, troponin, and CRP were measured preoperatively, 6 hours after reperfusion, and on postoperative day 7. While both groups demonstrated postoperative elevations consistent with the surgical context, no statistically significant differences were observed at any time point for any of the measured biochemical parameters between the two groups (P > 0.05 for all comparisons) (Table 2).
In terms of secondary outcomes, intraoperative hemodynamic variables, including cardiac output, systemic vascular resistance, and urine output, were recorded during the preanhepatic, anhepatic, and reperfusion phases. These parameters did not differ significantly between the isoflurane and sevoflurane groups across any phase of surgery (P > 0.05). Additionally, the requirement for inotropic support during each phase was comparable between groups, with no statistically significant differences during the preanhepatic (P = 0.87), anhepatic (P = 0.66), or reperfusion (P = 0.47) periods (Table 3).
Notably, a significant difference was observed in intraoperative transfusion requirements. Patients in the sevoflurane group required a greater volume of packed red blood cells (2.88 ± 1.73 units) compared to those in the isoflurane group (1.75 ± 1.71 units; P = 0.037). Similarly, the volume of fresh frozen plasma administered was higher in the sevoflurane group (2.42 ± 1.69 units vs. 1.25 ± 1.68 units; P = 0.028), indicating a greater transfusion burden associated with sevoflurane (Table 4).
As for adverse events, no significant differences were noted between the two groups. The incidence of postoperative bleeding, cardiac arrhythmias, and acute kidney injury was low and similar in both groups. No patients required reoperation or renal replacement therapy during the postoperative period, and no deaths were recorded within the early postoperative phase.
5. Discussion
This randomized clinical trial compared the effects of isoflurane and sevoflurane on short-term hepatic, renal, and cardiac outcomes in patients undergoing liver transplantation. The results demonstrated no significant differences between the two anesthetic agents in postoperative laboratory markers, intraoperative hemodynamics, or inotropic requirements. However, the use of sevoflurane was associated with a significantly higher intraoperative transfusion volume compared to isoflurane.
Our findings align with several previous studies suggesting that both isoflurane and sevoflurane can be safely used for anesthetic maintenance in liver transplantation, with comparable impacts on organ function (22, 27). The lack of difference in postoperative ALT, AST, bilirubin, creatinine, troponin, and CRP levels suggests that neither agent confers a clear advantage in attenuating IRI at the systemic level. This is consistent with the mechanistic similarities between the two agents, both of which have been shown to exert anti-inflammatory and antioxidant effects through modulation of pathways such as NF-κB, AKT, and Nrf2/HO-1 in preclinical studies (24, 28, 29).
Intraoperative hemodynamics, including cardiac output and systemic vascular resistance, were stable and comparable between the groups, supporting previous findings that both volatile anesthetics are hemodynamically acceptable in the setting of liver transplantation (27, 30, 31). Similarly, inotropic support requirements were not significantly different, suggesting no clear superiority of one agent over the other in cardiovascular performance during surgery.
Importantly, no major adverse events such as arrhythmias, acute kidney injury, or early graft failure occurred in either group, indicating that both anesthetics were well tolerated. While the observed difference in transfusion volume may have clinical implications — given the known risks associated with blood product administration — the short-term outcomes did not reveal any organ-specific complications linked to either anesthetic.
Interestingly, our study observed a significantly greater need for packed red blood cell and plasma transfusions in the sevoflurane group. Although the mechanisms underlying this difference are unclear, some reports have suggested that sevoflurane may interfere with coagulation or enhance fibrinolysis, potentially leading to increased bleeding (26, 32). However, these effects remain controversial and warrant further investigation in larger trials specifically designed to assess coagulation profiles.
The findings of this study can help us choose anesthetic drugs based on the coagulation status of each patient. For instance, Eyth et al. developed a model that can predict intraoperative blood transfusion (33). When an anesthesiologist identifies a patient with a higher risk of bleeding based on this model and similar models, they will choose an anesthetic drug with a lower risk of transfusion need, such as isoflurane, as explained in our study. However, this study has a small population. To integrate these findings into clinical practice, future studies will be necessary. Future studies on this area can be categorized into three main areas. First, the findings of this paper should be confirmed in larger studies. Second, more anesthetic drugs should be taken into consideration for such comparisons. Third, since blood transfusion is a determinant factor in liver transplant success (34), we may be able to integrate anesthesia drugs into risk score systems and predictive systems in liver transplant studies (35, 36).
Limitations Given the final sample size of 44 patients and the high variability typically seen in postoperative liver enzyme levels after liver transplantation, the study had limited statistical power to detect small-to-moderate differences in biochemical markers of organ injury or to formally demonstrate equivalence.
5.1. Conclusions
The results obtained in this study showed that the use of isoflurane and sevoflurane did not have a significant difference in the severity of ischemic reperfusion injury caused after liver transplantation surgery on the liver, kidney, and heart; also, in this study, the functional conditions of these organs during and after surgery were evaluated, and by examining at different time intervals, these two inhalation anesthetics did not have a different effect on the short-term outcome of patients after receiving a liver transplant.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang S Toy M Hang Pham TT So S Causes and trends in liver disease and hepatocellular carcinoma among men and women who received liver transplants in the U.S., 2010-2019.P Lo S One.2020159 e 023939310.1371/journal.pone.023939332946502 PMC 7500679 · doi ↗ · pubmed ↗
- 2Mahmud N Selection for Liver Transplantation: Indications and Evaluation.Curr Hepatol Rep.20201932031210.1007/s 11901-020-00527-932837824 PMC 7302921 · doi ↗ · pubmed ↗
- 3Peralta C Jimenez-Castro MB Gracia-Sancho J Hepatic ischemia and reperfusion injury: effects on the liver sinusoidal milieu.J Hepatol.2013595109410610.1016/j.jhep.2013.06.01723811302 · doi ↗ · pubmed ↗
- 4Zhai Y Petrowsky H Hong JC Busuttil RW Kupiec-Weglinski JW Ischaemia-reperfusion injury in liver transplantation--from bench to bedside.Nat Rev Gastroenterol Hepatol.2013102798910.1038/nrgastro.2012.22523229329 PMC 3577927 · doi ↗ · pubmed ↗
- 5Montalvo-Jave EE Escalante-Tattersfield T Ortega-Salgado JA Pina E Geller DA Factors in the pathophysiology of the liver ischemia-reperfusion injury.J Surg Res.20081471153910.1016/j.jss.2007.06.01517707862 PMC 2443391 · doi ↗ · pubmed ↗
- 6Fu P Li W Muriel P Nitric Oxide in Liver Ischemia–Reperfusion Injury.Liver Pathophysiology.20171257978012804274810.1016/b 978-0-12-804274-8.00008-4London, United Kingdom Academic Press · doi ↗
- 7Li CX Ng KT Shao Y Liu XB Ling CC Ma Y Yet al.The inhibition of aldose reductase attenuates hepatic ischemia-reperfusion injury through reducing inflammatory response.Ann Surg.201426023172810.1097/SLA.000000000000042924699020 · doi ↗ · pubmed ↗
- 8Dar WA Sullivan E Bynon JS Eltzschig H Ju C Ischaemia reperfusion injury in liver transplantation: Cellular and molecular mechanisms.Liver Int.201939578880110.1111/liv.1409130843314 PMC 6483869 · doi ↗ · pubmed ↗