Evaluation of improved lung and airway morphology using CT 3D reconstruction after severe scoliosis correction: a retrospective cohort study
Hanwen Zhang

TL;DR
This study uses CT scans to show that correcting severe scoliosis improves lung and airway structure.
Contribution
The novel use of CT 3D reconstruction to evaluate lung and airway changes after scoliosis surgery.
Findings
Posterior spinal fusion significantly improved spinal parameters like Cobb angles.
Lung volume and bronchial diameters increased significantly after surgery.
CT 3D reconstruction is effective for measuring lung and airway morphology changes.
Abstract
Previous studies have not compared lung and airway morphologies before and after treatment for severe scoliosis. Herein, computed tomography (CT) 3-dimensional (3D) reconstruction of the respiratory system was performed to evaluate the changes in lung expansion and airway dilation following posterior spinal fusion for severe scoliosis. Twenty-two patients with severe scoliosis (12 women and 10 men) who treated with posterior spinal fusion (PSF) were included. Pre- and postoperative visits included CT scans and radiographic assessments. Changes in airway dilation were assessed using 3D CT reconstruction of the bronchial tree, and changes in lung volume were evaluated using lung 3D CT reconstruction pre- and postoperatively. Spinal radiographic parameters improved after PSF. The main Cobb angles were 135.89 ± 21.80° and 50.51 ± 16.02° (p < 0.001), and thoracic kyphosis angles were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
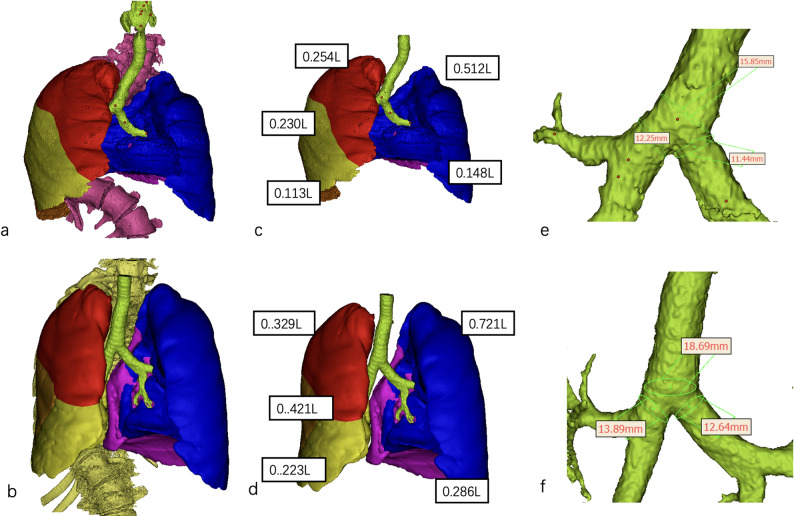 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsScoliosis diagnosis and treatment · Lung Cancer Diagnosis and Treatment · Medical Imaging and Analysis
Background
Correction of severe scoliosis is particularly challenging when the spinal deformity involves a Cobb angle greater than 100°, which is classified as severe [1–3]. The risk of postoperative pulmonary complications increases with declining pulmonary function [4–6]. Although restrictive lung deficits are common in patients with scoliosis, approximately 46% exhibit obstructive or mixed ventilatory defects preoperatively [7–9].
Lung 3D reconstruction helps reliably estimate the lung volume (LV) in patients with severe scoliosis; the lung can be divided into lobes [10–13]. Researchers have quantified the bronchial diameter and length using 3D imaging, [14–16], facilitating the reconstruction of the bronchial tree [17–19]. Further investigation of pre- and postoperative lung and airway morphologies in patients with severe scoliosis is warranted, driven by advancements in 3D lung and pulmonary bronchial tree reconstruction.
However, no studies have yet evaluated pre- and postoperative airway and lung volume morphological features in patients with severe scoliosis. This study utilized low-dose CT before and after posterior spinal fusion to evaluate the alterations in lung volume and airway parameters. We sought to assess whether the treatment of severe scoliosis affects lung and airway morphological features.
Materials and methods
Patient population
This retrospective study was approved by the Institutional Ethics Committee of Beijing Jishuitan Hospital in accordance with the Declaration of Helsinki. All patients provided written informed consent. Thirty-four patients with severe scoliosis who underwent posterior spinal fusion between January 2023 and January 2025 were reviewed. The inclusion criteria were as follows: (1) severe kyphoscoliosis (coronal Cobb angle or thoracic kyphosis angle ≥ 100°) and (2) posterior fusion surgery. The exclusion criteria were as follows: (1) spinal surgery prior to this study and (2) a history of surgery involving the thoracic cage. Demographic parameters included body mass index (BMI), etiology, sex, and age.
Radiographic parameters
Standing full long spinal X-ray in the posteroanterior and sagittal planes was acquired pre- and postoperatively. Alterations in spinal parameters were also evaluated, including the main thoracic Cobb angle, T1 to T12 height, C7 to S1 height, and kyphosis measurements from T5 to T12.
Airway reconstruction parameters
CT scans were performed for all patients using the Siemens SOMATOM Sensation 16 system (Germany, slice thickness:1.0 mm), which were used for preoperativeplanning and postoperative assessment of screw trajectories. Data were obtained in DICOM format and subsequently loaded into Mimics Medical 21.0 (Materialise NV, Leuven, Belgium). The segmented airway tool enabled semi-automatic segmentation of the airway tract, with user-initiated segmentation marking the onset of the trachea [14]. The diameter and lumen area of the trachea (superior to the carina) and the right and left major bronchi were measured.
Lung reconstruction parameters
The Segment Lung Lobes tool detects and fits freeform surfaces through the lung lobe, thereby separating fissures. The freeform surfaces can be updated by adjusting the points. Finally, the lungs were segmented using a freeform surface. The total lung volume (TLV), volume of each lobes, convex-side LV, and concave-side LV were observed on pre- and post-traction CT images using 3D reconstruction, as described in a previous study [20].
Statistical analysis
Radiographic measurements and airway and lung morphological measurements were compared pre- and postoperatively. Differences were assessed using two-tailed paired Student’s t-tests, and correlations were evaluated using Spearman’s rank test. SPSS version 25.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses. Statistical significance was set at p < 0.05.
Results
Twenty-two patients with severe scoliosis were analyzed (12 women and 10 men). The mean age was 23.58 ± 6.22 years, and the mean BMI was 15.24 ± 2.18 kg/m^2^. Etiological diagnoses were congenital scoliosis (n = 7), adult idiopathic scoliosis (n = 8), and neuromuscular scoliosis (n = 7). All patients underwent posterior spinal fusion without spinal osteotomy, and none of them had pulmonary complications or required postoperative ventilator support.
After PSF, all spinal radiographic parameters improved. The main Cobb angles were 135.89 ± 21.80° and 50.51 ± 16.02° in the pre-and postoperative groups, respectively (p < 0.001). Additionally, the thoracic kyphosis angles were 115.75 ± 35.47° and 47.60 ± 8.56° in the pre-and postoperative groups, respectively (p < 0.001). The distances from C7 to S1 were 282.56 ± 40.58 mm and 403.45 ± 40.89 mm in the pre-and postoperative groups, respectively (p < 0.001). Furthermore, the T1–T12 distances were 139.14 ± 29.11 mm and 218.25 ± 35.47 mm in the pre-and postoperative groups, respectively (p < 0.001) (Table 1).Table 1. Comparison of radiographic parameters between the pre- and post-operative groupsPre-operativePost-operativeP-valueMain cobb angle (°)135.89 ± 21.8050.51 ± 16.02 < 0.001C7–S1 (mm)282.56 ± 40.58403.45 ± 40.89 < 0.001T1–T12 (mm)139.14 ± 29.11218.25 ± 35.47 < 0.001Thoracic kyphosis (°)115.75 ± 35.4747.60 ± 8.56 < 0.001
Morphological parameters
The pre- and postoperative TLV values (1.48 ± 0.76 and 1.89 ± 0.33 L, respectively) were significantly different (t = 3.099, p = 0.0101). The pre- and postoperative values for the left LV (0.69 ± 0.34 and 0.88 ± 0.33 L) and right LV (0.69 ± 0.14 and 0.95 ± 0.28 L), respectively ([t = 3.802; p = 0.0029]; [t = 3.415; p = 0.0066]), were significantly different. For further analysis, the lungs were divided into five lobes. The right upper lobe (0.33 ± 0.25 and 0.37 ± 0.19 L, t = 2.159; p = 0.0599) and right middle lobe (0.18 ± 0.11 and 0.26 ± 0.12 L, t = 2.020; p = 0.0710) did not change significantly after PSF. The right lower lobe (0.29 ± 0.12 and 0.37 ± 0.16 L, t = 2.376; p = 0.0421) changed significantly after PSF. Interestingly, the right upper lobe combined with the right middle lobe volume changed significantly after PSF (0.47 ± 0.20 and 0.63 ± 0.23 L, t = 2.613; p = 0.0241). The pre and postoperative values for the left upper lobe volume (0.41 ± 0.19 L and 0.56 ± 0.21 L, respectively) and left lower lobe volume (0.22 ± 0.16 L and 0.33 ± 0.15 L, respectively) were significantly different ([t = 3.267, p = 0.0075] and [t = 4.317, p = 0.0012], respectively). After PSF, the main trachea, left main bronchus, and right main bronchus were dilated. The tracheal diameter exhibited a significant difference between the preoperative and postoperative groups (12.21 ± 1.91 mm vs. 15.32 ± 1.83 mm; p < 0.0001). The left main bronchus increased from 9.83 ± 2.41 to 12.01 ± 1.76 mm (p = 0.0124). The right major bronchus increased in diameter from 9.88 ± 2.41 to 11.63 ± 1.37 mm (p = 0.0058).
The pre- and postoperative groups demonstrated different lumen areas of the trachea (132.11 ± 34.91 mm^2^ vs. 182.41 ± 43.51 mm^2^, p < 0.0001), right main bronchi (81.43 ± 32.61 mm^2^ vs. 107.11 ± 24.71 mm^2^, p = 0.0078), and left main bronchi (79.26 ± 31.41 mm^2^ vs. 98.34 ± 30.11 mm^2^, p = 0.0242) (Table 2). Figure 1 illustrates a representative case.Table 2. Comparison of morphological parameters between the pre- and post-operative groupsPre-operativePost-operativeP-valueTotal lung volume1.48 ± 0.761.89 ± 0.330.0101Left lung volume0.69 ± 0.340.88 ± 0.330.0029Right lung volume0.69 ± 0.140.95 ± 0.280.0066Right upper lobe volume0.33 ± 0.250.37 ± 0.190.0599Right middle lobe volume0.18 ± 0.110.26 ± 0.120.0710Right lower lobe volume0.29 ± 0.120.37 ± 0.160.0421Right upper lobe combined right middle lobe volume0.47 ± 0.200.63 ± 0.230.0241Left upper lobe volume0.41 ± 0.190.56 ± 0.210.0075Left lower lobe volume0.22 ± 0.160.33 ± 0.150.0012Diameter of trachea12.21 ± 1.9115.32 ± 1.83 < 0.0001Lumen area of trachea132.11 ± 34.91182.41 ± 43.51 < 0.0001Diameter of left main bronchi9.83 ± 2.4112.01 ± 1.760.0124Lumen area of left main bronchi79.26 ± 31.4198.34 ± 30.110.0242Diameter of right main bronchi9.88 ± 2.4111.63 ± 1.370.0058Lumen area of right main bronchi81.43 ± 32.61107.11 ± 24.710.0078Fig. 1Images of a 28-year-old man with severe scoliosis who underwent posterior spinal fusion. The lobe volume, main trachea, and diameters of the left and right main bronchi improved after posterior spinal fusion. a Preoperative 3D-reconstruction of the lung, trachea, and spine. b Postoperative 3D-reconstruction of the lung, trachea, and spine. c Preoperative 3D-reconstruction of each lobe. d Postoperative 3D-reconstruction of each lobe. e Preoperative 3D-reconstruction of the bronchial tree. f Postoperative 3D-reconstruction of the bronchial tree
The main thoracic Cobb angle, thoracic kyphosis, T1–T12 distance, and C7–S1 distance were correlated with TLV. The right LV was correlated with the main thoracic Cobb angle, thoracic kyphosis, and C7–S1 distance, but not with the T1–T12 distance. Additionally, the right upper lobe volume correlated with the T11–T12 and C7–S1 distances. The right middle lobe volume was correlated with the C7–S1 distance, whereas the right lower lobe volume was correlated with the main thoracic Cobb angle. The combined right upper and middle lobe volumes correlated with the main thoracic Cobb angle, thoracic kyphosis, T1–T12 distance, and C7–S1 distance. The left upper and lower lobe volumes were correlated with the main thoracic Cobb angle, thoracic kyphosis, T1–T12 distance, and C7–S1 distance. Thoracic kyphosis was also correlated with the diameters of the trachea, left main bronchus, and right main bronchus (Table 3).Table 3. Correlations between lung morphological parameter and radiological variablesVariableMain thoracic Cobb angleTKT1-T12C7-S1P-valueR coefficientsP-valueR coefficientsP-valueR coefficientsP-valueR coefficientsTotal lung volume0.0009 − 0.65490.0078 − 0.55130.01270.52210.00850.5462Right lung volume0.0041 − 0.58660.0284 − 0.46720.09490.36490.03560.4501Left lung volume0.0063 − 0.56390.0170 − 0.50300.00690.55860.01480.5122Right upper lobe volume0.0768 − 0.36800.1019 − 0.34200.04890.40610.02770.4490Right middle lobe volume0.1196 − 0.32640.0734 − 0.37210.07640.36850.03230.4380Right lower lobe volume0.0446 − 0.43200.1834 − 0.29450.35900.20550.14710.3196Right upper lobe combined right middle lobe volume0.0018 − 0.62720.0250 − 0.47630.04300.43500.01510.5110Left upper lobe volume0.0112 − 0.52990.0303 − 0.46230.00310.60020.00830.5479Left lower lobe volume0.0007 − 0.66830.0016 − 0.63080.01650.50520.00440.5827Diameter of trachea0.2058 − 0.28070.0121 − 0.52500.23460.26430.07190.3911Diameter of Left main bronchi0.4062 − 0.18640.0318 − 0.45870.35960.20520.11070.3496Diameter of right main bronchi0.1175 − 0.34350.0020 − 0.62230.07760.38410.02740.4697
Discussion
Severe scoliosis negatively affects pulmonary function, potentially leading to significant morbidity and mortality [21, 22]. Restrictive ventilatory dysfunction is defined as reduced LV, which constrains respiratory capacity and results in decreased oxygen saturation. In contrast, obstructive ventilatory dysfunction is marked by constricted airway diameters and increased airway resistance [23, 24]. Previous studies have estimated pulmonary function based on anterior–posterior and lateral radiographic deformities [25–27]. However, scoliosis is a complex 3D spinal and rib cage deformity, and 2D images provide only limited information. The CT scan method is useful for accurately measuring LV in patients with deformities [11, 12]. PSF not only provides a strong corrective force but also has the potential to maintain or even improve pulmonary function [28, 29]. In this study, TLV, as well as the right and left LVs, increased significantly after PSF. Notably, CT reconstruction allows separation of the right and left lungs and further segmentation into five distinct lobes. The volumes of the right upper, left upper, and left lower lobes increased significantly after PSF. Although the volumes of the right upper and middle lobes did not individually change significantly, their combined volumes showed a significant increase.
Pulmonary complications are common because congenital spine deformities decrease not only the volume but also the function of the lungs [30]. Severe scoliosis significantly affects respiratory function. This effect is most often restrictive owing to severe anatomical distortion of the chest, leading to reduced LV, limited diaphragmatic excursion, and chest wall muscle inefficiency. Bronchial compression by a deformed spine may also occur but is rarer [31]. This study successfully reconstructed pre- and postoperative three-dimensional bronchial trees. Morphological metrics, such as the diameter and lumen area of the left and right main bronchi, were increased following posterior corrective surgery.
Various previous studies have reported conflicting results, ranging from mild improvement to worsening of the condition [32–34]. In this study, the total lung and lobe volumes, as well as the diameter of the central bronchi, improved after PSF. Based on the available evidence, it is reasonable to state that the main goal of scoliosis surgery is to preserve or improve lung function.
The Cobb angle is commonly used to describe the geometric severity of scoliosis. It is approximately correlated with overall clinical severity [35–38], although the exact relationship between scoliosis and lung function is highly complex [31]. Although these problems are more common or severe among patients with severe scoliosis, there is no direct correlation between them and the degree of scoliosis [25, 32, 39–41]. In this study, the main thoracic Cobb angle was correlated with LV parameters. As the Cobb angle was corrected using PSF, the volumes of all five lobes increased. However, the lumbar area and bronchial tree diameter did not correlate with the main thoracic Cobb angle. Prior research has shown a reduction in kyphosis in patients with thoracic scoliosis, which is characterized by spinal encroachment into the thoracic cavity, constricting the airway [8, 25]. Therefore, hypokyphosis is considered a relevant factor for airway obstruction. In this study, thoracic kyphosis was correlated with airway parameters. As kyphosis decreases with PSF, the bronchial airway tree expands. However, lobe volume did not correlate with thoracic kyphosis.
Although these findings offer insights into the anatomical and functional effects of PSF in severe scoliosis, certain limitations must be acknowledged. First, the small sample size may have prevented some comparisons from reaching statistical significance. Second, pulmonary function tests are considered the gold standard for measuring pulmonary impairment. This study only provided static morphological data. Further studies should focus on the relationship between static morphological data and functional data pre- and postoperatively. Various factors such as age, gender, and etiology may affect pulmonary function changes in severe scoliosis after PSF. Large sample size and detailed supplement information are necessary in further studies.
In conclusion, 3D CT reconstruction could be a surrogate method to quantify pulmonary morphological parameters in patients with severe scoliosis. PSF may effectively correct the curve, relieve airway obstruction, and expand the lungs of patients with severe scoliosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1N MJIJOT. Histochemical and physiological studies in idiopathic scoliosis. 1990;16(1).2116383 · pubmed ↗
- 2Farrell J, Garrido E. Effect of idiopathic thoracic scoliosis on the tracheobronchial tree. BMJ Open Respir Res. 2018;5(1).10.1136/bmjresp-2017-000264 PMC 587868129616140 · doi ↗ · pubmed ↗
- 3Laroia AT. Modern imaging of the tracheo-bronchial tree. World Journal of Radiology. 2010;2(7).10.4329/wjr.v 2.i 7.237PMC 299885521160663 · doi ↗ · pubmed ↗
- 4Aziz R, Nachiappan C, Peter D, et al. Movement analysis of scoliotic subjects using Fastrak. 2004;91(0).15457716 · pubmed ↗
- 5G C, V T, N MJJBJSB. Variability in Cobb angle measurements. 1996;78(2).8666658 · pubmed ↗
- 6G C, N M, V TJAOB. The validity and reliability of measurements in spinal deformities: a critical appraisal. 1992;58(2).1632212 · pubmed ↗