Non-infectious skeletal complications in the lower extremity after treatment with a transfemoral bone-anchored prosthesis: a retrospective observational study
Karin Svensson Malchau, Henrik Malchau, Peter Thomsen, Kerstin Hagberg

TL;DR
This study examines the risk of fractures and arthroplasty surgery in patients using a bone-anchored prosthesis for lower limb amputations.
Contribution
The study provides new data on the frequency of skeletal complications in transfemoral bone-anchored prosthesis users.
Findings
16% of patients experienced fractures or arthroplasty surgery in the lower limb after BAP surgery.
11% of patients had femur fractures, and 6% underwent arthroplasty due to osteoarthritis.
Prosthetic use was not affected by these complications.
Abstract
The use of bone-anchored prostheses (BAPs) has greatly increased quality of life for lower limb amputees. However, the long-term frequency of skeletal fractures and the need for arthroplasty surgery in the lower extremities following BAP use is scarce. The current study aimed to investigate the frequency of fractures and arthroplasties in the lower limb after BAP surgery with the Osseointegrated Prosthesis for the Rehabilitation of Amputees (OPRA) system. Retrospective cohort study using the OPRA database and medical record review for data collection. A single-centre study at a tertiary hospital. All patients with a transfemoral BAP (OPRA system) who underwent surgery between 1999 and 2019, and had completed at least 2 years of follow-up were included in the study. Patients with bilateral transfemoral amputations were excluded. A total of 100 patients were included. The primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
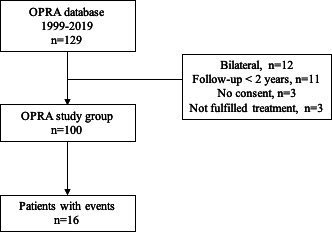 Figure 1
Figure 1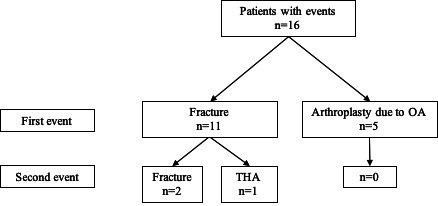 Figure 2
Figure 2 Figure 3
Figure 3| All patients n=100 | No events in lower limb n=84 | Events in lower limb n=16 | |
|---|---|---|---|
| Age, mean (SD) | 59 (14) | 58 (13) | 64 (15) |
| Sex, n (%) | |||
| Female | 34 (34) | 30 (36) | 4 (25) |
| Male | 66 (66) | 54 (64) | 12 (75) |
| Side, n (%) | |||
| Left | 49 (49) | 46 (55) | 3 (19) |
| Right | 51 (51) | 38 (45) | 13 (81) |
| Residency, n (%) | |||
| Europe, other than Sweden | 39 (39) | 33 (39) | 6 (38) |
| Sweden, other region | 52 (52) | 45 (54) | 7 (44) |
| Sweden, Western region | 9 (9) | 6 (7) | 3 (19) |
| Cause for TFA, n (%) | |||
| Trauma | 70 (70) | 61 (73) | 9 (57) |
| Tumour | 19 (19) | 16 (19) | 3 (19) |
| Embolism | 3 (3) | 3 (4) | 0 (0) |
| Infection | 8 (8) | 4 (5) | 4 (25) |
| ASA at surgery S1, n (%) | |||
| 1 | 42 (42) | 37 (44) | 5 (31) |
| 2 | 26 (26) | 22 (26) | 4 (25) |
| 3 | 2 (2) | 2 (2) | 0 (0) |
| Missing | 30 (30) | 23 (27) | 7 (43) |
| BMI at BAP surgery, mean (SD) | 26 (4) | 26 (4) | 25 (4) |
| Age completed BAP, mean (SD) | 44 (13) | 45 (13) | 43 (13) |
| Years between TFA and S1, mean (SD) | 11 (10) | 10 (10) | 13 (13) |
| Baseline prosthetic use score, mean (SD) | 44 (36) | 43 (35) | 51 (41) |
| Latest prosthetic use score, mean (SD) | 69 (35) | 69 (35) | 69 (37) |
| Cases of fixture reoperation, n (%) | 13 (13) | 10 (8) | 3 (19) |
| Sex | Age amp | Time to BAP | Event | Time from BAP to event (years) | Side | Treatment | Event 2 and side | Treatment 2 |
|---|---|---|---|---|---|---|---|---|
| M | 46 | 13 | fx | 4 | IL | ORIF | – | – |
| F | 14 | 33 | fx | 13 | IL | MIS | fx, IL | ORIF |
| M | 21 | 18 | fx | 3 | IL | ORIF | – | – |
| M | 30 | 43 | fx | 13 | IL | ORIF | – | – |
| F | 46 | 12 | fx | 2 | IL | ORIF | oa, CL | THA |
| M | 63 | 2 | oa | 3 | CL | TKA | – | – |
| M | 32 | 1 | fx | 13 | IL | MIS | fx, IL | ORIF |
| M | 31 | 3 | fx | 1 | IL | No surg | – | – |
| F | 47 | 6 | oa | 13 | CL | TKA | – | – |
| M | 34 | 4 | fx | 10 | CL | Extraction | – | – |
| M | 25 | 31 | oa | 6 | CL | TKA | – | – |
| F | 17 | 5 | fx | 2 | IL | No surg | – | – |
| M | 37 | 23 | oa | 1 | CL | THA | – | – |
| M | 65 | 5 | oa | 3 | CL | TKA | – | – |
| M | 23 | 9 | fx | 8 | IL | ORIF | – | – |
| M | 60 | 1 | fx | 1 | IL | HHA | – | – |
| Patient | Baseline PUS | PUS before event | PUS after event | Difference PUS before and after event | Latest recorded PUS |
|---|---|---|---|---|---|
| 1 | 61 | 100 | 100 | 0 | 71 |
| 2 | 100 | 90 | 90 | 0 | 71 |
| 3 | 32 | 100 | 90 | −10 | 71 |
| 4 | 90 | 90 | 90 | 0 | 90 |
| 5 | 0 | 52 | 90 | +38 | 100 |
| 6 | 100 | 100 | 100 | 0 | 100 |
| 7 | Missing | 3 | 18 | +15 | 18 |
| 8 | 90 | Missing | Missing | Missing | 100 |
| 9 | 71 | 90 | Missing | Missing | 90 |
| 10 | 4 | 100 | Missing | Missing | 100 |
| 11 | 90 | 100 | 100 | 0 | 90 |
| 12 | 0 | 23 | 0 | −23 | 0 |
| 13 | 90 | 90 | 90 | 0 | 90 |
| 14 | 6 | 10 | 10 | 0 | 10 |
| 15 | 1 | 100 | 100 | 0 | 100 |
| 16 | 37 | 71 | 100 | +29 | 10 |
- —ALF
- —http://dx.doi.org/10.13039/501100015662Johan Jansson Foundation
- —Hjalmar Svensson Foundation
- —Eivind or Elsa K:son Sylvan Foundation
- —IngaBritt and Arne Lundberg Foundation
- —Area of Advance Materials of Chalmers and GU Biomaterials within the Strategic Research Area Initiative launched by the Swedish government
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProsthetics and Rehabilitation Robotics · Total Knee Arthroplasty Outcomes · Orthopaedic implants and arthroplasty
Introduction
Osseointegration was first described in the 1950s and implies the structural connection between the implant and bone.1 This discovery paved the way for the use of bone-anchored prostheses (BAP) for clinical use. In orthopaedics, transcutaneous BAPs are used in patients who have undergone amputations, often due to trauma or tumours, who have experienced severe problems functioning with a socket-mounted type artificial limb. The recent advances within this medical field have enabled amputees to regain physical function with an artificial limb without the pain and skin-related problems a socket prosthesis may imply.2 3 One such implant system is the Osseointegrated Prosthesis for the Rehabilitation of Amputees system (OPRA Implant System) which has been in use since the 1990s.4 5
The OPRA system consists of three main parts: a bone-anchored fixture in which the percutaneous abutment is connected through the abutment screw. Thereafter, an external prosthesis can be attached via a safety device, so-called Axor II, which protects the osseointegrated implant parts if the external prosthesis is made subject to great forces. The OPRA system requires two surgeries: stage 1 (S1) for fixation of the fixture, and stage 2 (S2) 3–6 months later for insertion of the abutment once the fixture has been integrated in bone.6 Rehabilitation is commenced after S2 with a gradual and structured increase of weight bearing and further rehabilitation during 6–12 months postoperatively.7 8
Percutaneous BAPs, such as the OPRA system, have substantially improved the functional outcome and quality of life for many patients with amputations.9 The OPRA system has been described as revolutionary in the life of amputees,10 and treated patients have reported increased prosthetic usage, also in the long term.11 Other implant systems used in patients with lower limb amputations have been evaluated with similar increases in prosthetic usage.12 13
However, there are issues with mechanical and non-infectious complications after percutaneous BAP. As there is great stress at the fixture-abutment site, exchange of the abutment and/or abutment screw occurred in 29% of patients with an OPRA system due to implant fractures 5 years postoperatively.5 14 Moreover, prospective studies of the transfemoral OPRA implant system have revealed a 17% revision-free survival rate for mechanical complications after 10 years.11 Further, individuals with lower limb amputations are more prone to develop osteoarthritis (OA) in the longer term of the contralateral hip and knee,15 and osteoporosis in the ipsilateral extremity.1618
The OPRA system is considered a stable system with well-fixated implants.19 As patient satisfaction among those treated with BAP devices is high as compared with their previous situation using conventional socket prostheses, the need for this kind of implant system may increase in the future.4 Nevertheless, the frequencies of fractures and arthroplasty surgery in the lower extremities following long-term OPRA treatment remain unknown. In the present study, we aimed to investigate the frequency of femoral fractures and arthroplasties, as well as the impact of these complications on the prosthetic use after OPRA surgery.
Methods and materials
All patients registered with an OPRA Implant System due to a transfemoral amputation (TFA) in the OPRA database at the Sahlgrenska University hospital (SU) were screened. Patients who had their S1 between 31 December 1998 and 31 December 2019, and who had completed their treatment (S1, S2 and rehabilitation) at SU were included in the study. Patients operated on with an OPRA system at SU were invited to standardised follow-ups at 1, 2, 3, 5, 7, 10, 15 and 20 years after treatment.
Medical records were reviewed and assessed until 31 December 2021. Patients who did not have at least 2 years follow-up at that time point were excluded. Further exclusion criteria were missing consent and the presence of bilateral TFAs. Bilateral TFAs were excluded as these patients were considered to have a different risk for events following surgery.
Medical records were reviewed, and the following variables were retrieved: age, sex, body mass index, American Society of Anesthesiologists Physical Status score, laterality, date of amputation, cause of amputation, number of fixture revisions, new injuries in the lower extremity and mortality. Complete medical records were available for patients from the Western Region in Sweden (n=9, 9%) and, in remaining cases (other regions in Sweden (n=52, 52%), other European citizenship (n=39, 39%), complications, if any, were disclosed by the patient during follow-ups organised by the Sahlgrenska University multidisciplinary treatment team. Any experience of a fracture or arthroplasty surgery in the lower extremities was referred to as an event. To evaluate prosthetic usage, the Q-TFA Prosthetic Use Score (PUS, 0–100) was retrieved from the database. The PUS is a patient-reported outcome combining the number of days/week and number of hours per day the prosthesis is normally used. A figure of 0 means not using the prosthesis at all during a week and 100 means it is used daily for >15 hours.20
Objectives
The current study aimed to investigate the prevalence of events in the form of fractures and arthroplasties as well as the prosthetic use in patients treated with an OPRA implant.
Statistical analysis
Data were analysed descriptively with frequency counts and percentages (n and %) for categorical variables. Software IBM SPSS V.29 was used for data analysis.
Patient and public involvement
Patients and public were not involved in the study.
Results
A total of 100 patients met the inclusion criteria (figure 1). Patients were followed for a mean of 13.2 (±5.2) years after S2 and 56% had been followed for 10 years or more. The average age after completed surgical treatment (both S1+S2) was 44 years and the most common cause for TFA was trauma (n=70, 70%), followed by tumour (n=19, 19%) (table 1).
A flow diagram of study inclusion. OPRA, Osseointegrated Prosthesis for the Rehabilitation of Amputees.
16 patients experienced a lower limb skeletal event, either arthroplasty surgery due to OA or a femur fracture (table 1, figure 2). There were more male patients in the group with lower limb skeletal events (n=12, 75%) compared with patients without lower limb events (n=54, 64%). Patients with these events had a higher baseline prosthetic usage, that is, increased use prior to BAP surgery, than those who later had no events (mean PUS of 51 vs 43. However, at the latest follow-up, patients reported on similar prosthetic usage regardless of lower limb events (mean PUS 69 in both groups). Revisions, that is, exchange, of the bone-anchored fixture was more common in the group with events (n=3, 19%) compared with those who did not experience any lower limb events (n=10, 8%).
Distribution of postoperative events, grouped as either a fracture or arthroplasty due to OA, for patients with a transfemoral OPRA system. OA, osteoarthritis; OPRA, Osseointegrated Prosthesis for the Rehabilitation of Amputees; THA, total hip arthroplasty.
Patient with lower limb events
Patients with skeletal complications of the lower limb, referred to as ‘event’, had their TFA at a range of ages between 14 and 65 years and the time from amputation to event was from 1 to 43 years (table 2). A larger proportion of the patients (75%) were male. On average, patients experienced their event 6 (4.7 SD) years after their S2 and the most common first event was a fracture (n=11, 69%). All fractures were of the femur and on the ipsilateral side as the BAP fixture. Figure 3 illustrates an X-ray of a patient with BAP and ipsilateral osteosynthesis. The main reason for fracture was fall trauma (trauma mechanism was not described for all patients, however, at least 79% of fractures were due to falls). Patients with an arthroplasty due to OA as their first event (n=5) presented with contralateral OA most commonly of the knee (n=4, 80%). Three patients experienced yet another event after their first one in the form of a femur fracture (n=2) or total hip arthroplasty (THA) due to OA (n=1).
An example of a X-ray image of a pertrochanteric femur fracture fixated with osteosynthesis on the ipsilateral side as the BAP. BAP, bone-anchored prosthesis.
One patient underwent a definitive extraction of the fixture. This was due to a fixture fracture and associated stress fracture of the femur. An additional two patients underwent a revision of their fixture, independent of their femur fracture. These two revisions occurred several years after the patients’ first event.
In regard to PUS, 50% of the patients (n=8) were not affected by their event and used their external prosthesis in the same manner as prior to their fracture/OA treatment at the latest recorded follow-up (table 3). Three patients (19%) reported an increased use of their prosthesis after their event and two patients (12.5%) reported a decrease.
Discussion
Little is known with regard to the long-term situation for patients with an OPRA system in terms of postoperative skeletal events of the lower limb. The current study aimed to evaluate postoperative lower limb events and found an incidence rate of 11% fractures and 6% arthroplasties due to OA in the years following the treatment. Two patients who had a fracture suffered a second fracture. However, the average prosthetic usage was the same in patients who had an event compared with those who did not.
Although the treatment team has had continuous contact with included patients and noted whether they have had complications at each follow-up, the fact that complete medical records were unavailable in the majority of patients is a limitation. There may be patients who have suffered lower limb complications unknown to the authors. Furthermore, there may be patients who have had issues with OA prior to their BAP treatment. Evaluating the presence of OA would have been more reliable if screening of symptoms of OA and radiographs had been a standard procedure before the OPRA treatment was initiated.
The number of patients in the current study is limited as BAP treatment is not vastly used. The number of events was too small to conduct any further rigorous analysis. Factors such as time from amputation to BAP treatment may affect the outcome and whether socket prostheses have been used in the meantime. Such factors would be interesting to analyse as well as rehabilitation details and motivation, as they most likely affect functional performance. Furthermore, it would have been of interest to have an age-matched control group to compare the prevalence of events in the BAP group to that of the general population.
The greatest strength of the present study lies in its volume of BAP patients and a follow-up time of at least 10 years among more than half of the study cohort and its long follow-up time. To the authors’ knowledge, it is the first study to describe the situation in regard to lower limb complications that patients with a TFA OPRA system face.
Örgel et al studied the rate of fractures after surgery with the endo-exo-prosthesis (EEP) system, a press-fit implant for amputees. Assuming Örgel et al found no bilateral fractures, comparing the rate of postoperative fractures, Örgel et al found a rate of 6% and Hoellwarth et al found a 5% rate, whereas the current study established a rate of 11%.4 21 Hoellwarth et al included BAPs in the femur, tibia and the upper extremity, making direct comparisons difficult. Additionally, the BAP systems of the three studies differ, and the OPRA system is constructed to spare the fixture in cases of excessive loading leading to fractures; hence, the abutment and abutment screw are more prone to fracturing. These can be exchanged without hampering the osseointegrated (fixture) component.22 However, the current study reports on a higher rate of femur fractures compared with the use of the EEP. The aim of the current study was not to compare the two systems, so the results should be interpreted with caution. Furthermore, Örgel et al employed a 12-month follow-up, whereas the current study had an average follow-up time of 13.2 years after S2. The average age of patients with EEP was 49 years compared with 59 years in the current study. The risk for femur fractures and OA increases with age, and the group of patients with events was older than those with no events (64 compared with 58 years of age). Higher age and especially longer follow-up time may explain the greater number of postoperative fractures in the current study.
Total knee arthroplasty (TKA) was most common in the group of patients who underwent arthroplasty surgery due to OA. Norvell et al reported on a higher rate of contralateral knee OA and knee pain in amputees compared with non-amputees.23 The increased prevalence of OA has previously been suggested to be due to the increased load amputees may put on the contralateral side after their amputation. Gait analyses have reported that amputees present with asymmetrical gait, and increased loads can be detected at the contralateral knee during weightbearing.24 In a recent systematic review, contralateral OA (66.7%) was found more common than ipsilateral.25 Surprisingly, few THAs due to OA were identified in the current study (n=1). In patients with TFA, OA of the hips is a known complication affecting both the amputated and contralateral side to a greater extent than non-amputees.26 The review by Walton et al suggests that the number of patients with THA should be higher, as THA (195/265) was more common than TKA (51/265).25 However, the current result should be interpreted with great caution as several patients may have been affected by hip OA and a full hip assessment with screening for OA symptoms and radiographs was not conducted.
An important finding in the present study was that prosthetic usage was similar regardless of whether an event had occurred. This is also supported by the findings of Örgel et al reporting that periprosthetic fractures in BAP treated amputees did not worsen functional outcome.21 In both studies, implant-preserving osteosyntheses of fractures were used, apart from one case in the current study which required implant extraction. Planning osteosynthesis of a hip fracture or periprosthetic fracture may be challenging as the implant may obstruct the preferred method of fracture fixation. Likewise, possibilities to treat OA with THA may be limited and pose a challenge for the surgical team, although there are successful reports of combinations of BAP and THA of the same side.27 28 Although BAP patients may require longer rehabilitation, physical function seems similar for patients with a BAP and THA compared with those undergoing THA.25
Nearly half of the fractures reported by Örgel et al were caused intraoperatively. No intraoperative fractures were identified in the current cohort, and all fractures of the current study were postoperative and mainly fall related (at least 79% were due to falls). Osteopenia and osteoporosis of the ipsilateral femur is a known complication after amputation,18 26 as is the increased risk for falls.29 Therefore, an elevated risk of postoperative fractures is not surprising. However, an increased risk for falls has been reported in association with the use of socket prostheses, where some falls have been perceived as a direct cause of the prosthesis as such.30 The current study does not include a proper fall evaluation. Future studies on BAPs are recommended to include information if a fall was while wearing or not wearing the prosthesis and details of prosthetic knee components. A BAP may offer better stability and thereby reduce the fall risk and perhaps increase prosthetic usage, in turn increasing bone mineral density due to increased weight-bearing.
The current study, including non-Scandinavian patients, reports on an increased incidence of hip fractures (11%) compared with the age-standardised hip fracture incidence in Scandinavia of 5%–6%, which is the highest in the world.31 When compared with the incidence of hip fractures in the general population, there are several factors to account for. Ethnicity, genetics, age and comorbidities greatly influence the risk and the overall risk for females is greater than for males.32 Interestingly, more males than females experienced lower leg events in the current study; this tendency was also present in the study by Örgel et al.21 The prevalence of THA or TKA in the general Swedish population is 3.2%, compared with 6% in the current study.33 The numbers are not directly comparable and are not age-matched; however, they suggest that there may be a higher prevalence of arthroplasties in BAP patients. This may be due to an increase in activity levels after BAP34 hypothetically also combined with a somewhat abnormal kinematic and kinetic gait.35
Conclusions
Although larger comparative studies need to be conducted, patients with BAP may be at a higher risk for femur fractures and arthroplasty than the general population. This is important to consider when rehabilitating after BAP. Also, the presence of BAP may require special attention when planning ipsilateral osteosynthesis or arthroplasty. Prosthetic usage seems similar regardless of the patient has experienced a femur fracture or arthroplasty surgery of the lower limb. This is encouraging, however, further prospective studies with larger cohorts and control groups need to be conducted to compare functional outcomes and patient satisfaction in BAP patients with the general population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brånemark PI Osseointegration and its experimental background J Prosthet Dent 19835039941010.1016/s 0022-3913(83)80101-26352924 · doi ↗ · pubmed ↗
- 2Ghoseiri K Safari MR Prevalence of heat and perspiration discomfort inside prostheses: literature review J Rehabil Res Dev 2014518556810.1682/JRRD.2013.06.013325356571 · doi ↗ · pubmed ↗
- 3Hagberg K Brånemark R Consequences of non-vascular trans-femoral amputation: a survey of quality of life, prosthetic use and problems Prosthet Orthot Int 2001251869410.1080/0309364010872660111860092 · doi ↗ · pubmed ↗
- 4Hoellwarth JS Tetsworth K Rozbruch SR et al Osseointegration for Amputees: Current Implants, Techniques, and Future Directions JBJS Rev 20208 e 004310.2106/JBJS.RVW.19.0004332224634 PMC 7161721 · doi ↗ · pubmed ↗
- 5Brånemark R Berlin O Hagberg K et al A novel osseointegrated percutaneous prosthetic system for the treatment of patients with transfemoral amputation: A prospective study of 51 patients Bone Joint J 201496-B 1061310.1302/0301-620X.96B 1.3190524395320 · doi ↗ · pubmed ↗
- 6Li Y Brånemark R Osseointegrated prostheses for rehabilitation following amputation : The pioneering Swedish model Unfallchirurg 20171202859210.1007/s 00113-017-0331-428229193 PMC 5371647 · doi ↗ · pubmed ↗
- 7Li Y Felländer-Tsai L The bone anchored prostheses for amputees – Historical development, current status, and future aspects Biomaterials 202127312083610.1016/j.biomaterials.2021.12083633894405 · doi ↗ · pubmed ↗
- 8Hagberg K Brånemark R One hundred patients treated with osseointegrated transfemoral amputation prostheses--rehabilitation perspective J Rehabil Res Dev 2009463314419675986 · pubmed ↗