Advancing brain health equity with Indigenous peoples: A critical imperative
Antonia J. Clarke, Cliff Whetung, Astrid Suchy‐Dicey, Adrienne Withall, Kylie Radford, Diane C. Gooding, Louise Lavrencic, Makarena Dudley, Dina Lo Giudice, Leon Flicker, Arantxa Sanchez Boluarte, Sulakshna Aggarwal, Kyle R. Conniff, Amy G. Brodtmann, Monica M. Diaz

TL;DR
The paper argues that structural inequities and colonization, not biology, cause higher dementia rates in Indigenous communities and calls for culturally grounded approaches to brain health.
Contribution
It introduces a framework for decolonizing dementia research and policy by centering Indigenous leadership and cultural resilience.
Findings
Dementia disproportionately affects Indigenous populations due to structural inequities and colonization, not biological factors alone.
Cultural continuity and community leadership are vital for brain health and can serve as neuroprotective resources.
A shift toward culturally grounded, strengths-based models is needed to advance brain health equity for Indigenous peoples.
Abstract
Indigenous communities hold rich knowledges, cultural practices, and kinship networks that sustain cognitive resilience and nurture brain health across the life course. Yet these enduring strengths are often obscured by biomedical models that overlook the structural determinants of health—including the cumulative effects of colonization, educational inequity, and socioeconomic disadvantage—that diminish brain health. Accordingly, dementia disproportionately affects Indigenous populations globally, often presenting with earlier onset and higher prevalence compared to non‐Indigenous groups. This perspective synthesizes the current epidemiological evidence, situates dementia risk within its structural and historical context, and explores how Indigenous knowledges, cultural continuity, and community leadership can inform dementia research and care more broadly. Our global insights call for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1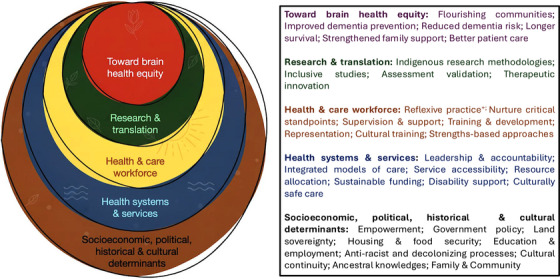 FIGURE 2
FIGURE 2| Name | Positionality |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- —NHMRC10.13039/501100000925
- —ANZAN Education and Research Fund
- —Eastern Health Foundation10.13039/100009717
- —Dementia Australia Research Foundation10.13039/100008710
- —Alzheimer's Association10.13039/100000957
- —National Institute on Aging10.13039/100000049
- —National Institutes of Health10.13039/100000002
- —American Indians
- —Strong Heart Study Oklahoma Field Center
- —Dementia Australia Research Foundation Post‐Doctoral Fellowship
- —Fogarty International Center of the National Institutes of Health
- —Northern Pacific Global Health Fellows Program
- —Interdisciplinary Cerebrovascular Diseases Training Program in South America
- —University of North Carolina at Chapel Hill10.13039/100007890
- —Universidad Cesar Vallejo
- —Madison Biology of Aging
- —University of Wisconsin
- —Madison All of Us Program
- —National Institute of Mental Health10.13039/100000025
- —Applied Research Collaboration
- —National Institute of Health and Care Research
- —AA‐FAIM
- —Wisconsin ADRC
- —ADRC10.13039/100006528
- —Fonds de recherche du Québec (FRQ) secteur Santé
- —WRAP
- —IDSMB
- —Scientific Advisory Board
- —National Institutes of General Medical Sciences
- —Avant Research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIndigenous Health, Education, and Rights · Indigenous Studies and Ecology · Indigenous Health and Education
INTRODUCTION
1
Dementia is increasingly recognized as a condition shaped across the life course, with its onset reflecting the accumulated imprint of socio‐economic, political, and biological forces. Cognitive resilience, the brain's capacity to adapt and thrive in the face of challenges, is also forged within these contexts.1 For Indigenous communities worldwide, cognitive resilience is deeply socio‐cultural, grounded in inter‐generational knowledge systems, land‐based practices, and the strength of community and kinship.2, 3 These tenets are believed to protect brain health and buffer the enduring impacts of colonization, yet they are often overlooked in dementia research and policy.4 Their omission contributes to a disproportionate burden of dementia for Indigenous peoples globally: in high‐income countries (HICs), dementia prevalence is reportedly up to threefold higher than the referent non‐Indigenous populations,5, 6 with onset occurring a decade or more earlier.7, 8 Evidence from low‐ and middle‐income countries (LMICs) also reveals marked variation shaped by geography and culture.9, 10, 11 The available data highlight both unique protective and risk factors, the consistent influence of structural inequities, and the cumulative effects of adverse social determinants of health. Advancing brain health equity for Indigenous peoples therefore demands more than biomedical risk reduction. It requires an approach rooted in dismantling systemic barriers to good health and recognizing that dementia risk is context specific and culturally situated. Indigenous leadership is an essential first step to integrating culturally grounded, holistic pathways of resilience into dementia prevention and care.
Box 1: Definitions of the key constructs identified within Indigenous health and well‐being frameworks, adapted from definitions provided by Chen et al., 2022,12 Joshi et al., 2022,13 and Udeh‐Momoh et al., 2025.1
- Brain health: A lifelong continuum of cognitive, socio‐emotional, and spiritual well‐being determined by intergenerational, ecological, psychological, social, and cultural influences.
- Cognitive reserve: A latent capacity built through lifelong and culturally grounded learning that enables compensation for pathology via flexible neural network recruitment.
- Cognitive resilience: The capacity to sustain cognitive functioning in the face of structural, social, historical, and health‐related stressors, supported by cultural continuity, kinship, and community strengths.
In this article, “Indigenous” refers to the first peoples of lands colonized predominantly by European powers— communities whose cultural, spiritual, and political identities are rooted in pre‐colonial histories and who endure despite centuries of dispossession and systemic marginalization. Globally, relationships between non‐Indigenous populations and Indigenous peoples in colonized countries remain shaped by colonial ideologies and dominant Western worldviews, sustaining historical and geopolitical inequities in health and well‐being. Yet Indigenous peoples are not passive in colonial contexts, and most, if not all, have never ceded sovereignty to lands, bodies, knowledge systems, culture, spirituality, and spirit. Indigenous people are reclaiming and restoring Indigenous knowledges to strengthen self‐determination and Indigenous human rights. These efforts support the well‐being of Elders and older people, communities, future generations, and a more responsive approach to dementia research, prevention, and care.3
This review represents the first global collaboration between Indigenous and non‐Indigenous researchers, educators, and clinicians to delineate the methodological and system‐level changes required to advance brain health equity with Indigenous populations (Figure 1). This perspectives piece arises from a collaboration at the 2025 Alzheimer's Association International Conference in Toronto, Canada. We demonstrate that prevailing epidemiological paradigms insufficiently account for the historical, geographical, and structural conditions that shape dementia risk, constraining both evidence and intervention design. By foregrounding Indigenous worldviews, rooted in relationality and holism, we identify conceptual pathways that could strengthen dementia prevention and care policies and advance lifelong brain health more broadly. Box 1 operationalizes this shift by situating the constructs of brain health, cognitive resilience, and cognitive reserve within Indigenous conceptualizations of health.
The coming together of many stories and many peoples, across many lands, unified for brain health equity with Indigenous peoples and for the next generation. This is an original artwork commissioned for this manuscript, created by Isla Sutherland, daughter of Associate Professor Adrienne Withall. The artwork incorporates motifs from Aboriginal and Torres Strait Islander, Māori, Canadian First Nations, Inuit, and Métis, American Indian and Alaska Native, Native African, and Native Hawaiian cultures, representing the diversity of voices and ideas that contributed to this manuscript. The curved linear imagery is reminiscent of the folds of the brain, made vibrant by upholding the tenets of Indigenous determinants of health—respect for Elders, cultural knowledge and spirituality, intergenerational connection to ancestors, and responsibility to care for Country. By combining several artistic aspects of each culture, every instroke is a wave of unity, integration, and cultural pride. The rich, earthy colors collide to create a work that is not only connected to people, but to land and all other Indigenous aspects. © 2025 Isla Sutherland. Reproduced with permission.
To support transparency and reflexivity, we present positionality statements from all contributing authors, outlining our cultural, professional, and geographic perspectives in relation to Indigenous knowledges and experiences (Table 1).
CURRENT EPIDEMIOLOGICAL EVIDENCE ON DEMENTIA AMONG INDIGENOUS POPULATIONS
2
Understanding the burden of dementia among Indigenous peoples requires interrogation of the existing epidemiological evidence and its methodological approach. Although emerging data demonstrate a disproportionately higher prevalence and earlier onset of dementia in many Indigenous populations, these patterns are shaped by the unique socio‐cultural and historical influences on data collection, diagnostic practices, and representation in research.
Although age‐standardized dementia prevalence estimates vary across studies, Indigenous populations consistently demonstrate higher dementia prevalence referent to the dominant national or regional non‐Indigenous population 60 years of age or older in very high Human Development Index (HDI) countries. This pattern has been reported among Aboriginal and Torres Strait Islander peoples in Australia; Māori in Aotearoa New Zealand; First Nations, Métis, and Inuit populations in Canada; and Native Hawaiian and American Indian and Alaska Native populations in the United States.5 Similar findings are also seen among Indigenous populations in Asia, including Singaporean Malay and Melanau groups in Malaysia.5 Evidence from LMICs suggests a disproportionately high burden of dementia among Indigenous communities, although the picture is more heterogeneous. In the Brazilian Amazon, prevalence among Indigenous groups such as the Mura, Mamirauá, and Amanã, has been reported as more than double the national estimate of 5.8% for older adults.9, 10, 14 Notably, very low prevalence has been observed among the Tsimane and Moseten of Bolivia, whose subsistence‐based agricultural lifestyles and limited exposure to urban risk factors are proposed to offer some protection.11, 14
The burden of dementia across younger age bands emerges as a consistent finding and may reflect the earlier accumulation of known dementia risk factors within Indigenous populations, as well as the resilient survival of older adults. For example, age‐specific prevalence is up to five times higher for remote‐living Aboriginal and Torres Strait Islander peoples younger than 60 years of age compared to national Australian estimates.15 Clinic‐based data show that Native Hawaiians younger than 60 years of age are nearly two times more likely to have dementia compared to non‐Indigenous populations.16 Earlier onset of dementia is also frequently reported across most LMIC studies, except for the Tsimane and Moseten, where cases primarily occur after age 80 years.11 Younger‐onset dementia confers unique challenges, including disruption of provider roles in family and community systems, thereby compounding financial disadvantage and adding urgency to the need for responsive engagement.17
Incidence rates of dementia are less well established among Indigenous populations. The evidence suggests higher incidence among Indigenous peoples relative to non‐Indigenous populations in Australia and the United States.18, 19, 20, 21 It is broadly accepted that the number of Indigenous peoples living with dementia is expected to rise due to increasing life expectancy, cohort flow from younger age groups into older age, and strengthened Indigenous identification.22, 23 Alongside these projected increases, diagnostics point to distinct patterns in dementia subtypes among Indigenous peoples.? Although Alzheimer's disease remains the most commonly diagnosed dementia, there is a higher frequency of mixed or unspecified dementia among Indigenous individuals, suggesting the possibility of more pronounced vascular contributions and the need for culturally specific assessment tools.5, 24 As disease‐modifying therapies gain regulatory approval worldwide, there is a pressing need to consider accurate diagnostic approaches for all peoples at risk of dementia.
Some of the variation seen in dementia epidemiology reflects the diversity of Indigenous experiences: Indigenous cultures, histories, social structures, and health outcomes differ across communities, regions, and contexts. Factors such as geography, social organization, political representation, and access to resources shape both dementia risk and cognitive resilience. Communities with stronger social and political organization may show lower prevalence. Framing prevalence solely at the national level risks masking these distinctions and highlights the need for more community‐level analyses capable of capturing place‐based determinants of dementia.
Refining epidemiological approaches
2.1
Longstanding methodological constraints limit robust understanding of dementia among Indigenous peoples. Indigenous populations remain underrepresented in dementia research, often amalgamated with disparate minoritized groups. This approach overlooks the unique positioning of Indigenous peoples as the traditional and rightful owners of lands who bear the impacts of colonization and historical and current policies that influence health equity. Within the context of dementia, Indigenous peoples may engage in differing health care practices, hold unique perspectives on cognitive decline, and rely more heavily on community‐based approaches to care, all of which can delay or obscure medical diagnoses of dementia.25, 26, 27
Administrative datasets, which require a documented diagnosis of dementia in medical records are likely to underestimate case numbers.28, 29, 30 Electronic health records amplify bias and misclassification of Indigenous peoples’ cultural identity, with providers variably categorizing patients and often assuming patients’ race or ethnicity.31 Similarly, community‐based epidemiological approaches that rely on standard neuropsychological approaches frequently lack cultural validity in Indigenous contexts. Persistent issues include epistemic racism, culturally inappropriate test items, language barriers, educational bias, and normative data derived from non‐Indigenous populations.32, 33 For instance, orientation questions such as naming the day or month may be unsuitable in communities where time is understood through environmental or seasonal cues.10 Incorporating sociocultural factors such as bilingualism and engagement in cultural practices, often excluded from conventional psychometric frameworks, is vital to understanding cognitive resilience among Indigenous peoples.34, 35
Several culturally tailored cognitive assessment tools have been developed. The Kimberley Indigenous Cognitive Assessment (KICA) in Australia,36, 37 the Canadian Indigenous Cognitive Assessment (CICA),38 the Māori Assessment of Neuropsychological Abilities (MANA),39 the American Indian Cognitive Assessment (AMICA),40 the Bharmour adaptation of the Mini‐Mental State Examination (BMSE),41 and the Brazilian Indigenous Cognitive Assessment (BRICA)10 are adaptations of cognitive assessments developed in partnership with Indigenous communities. These tools incorporate culturally relevant stimuli and account for educational contexts and traditional experiences. More research is needed on their suitability where Indigenous peoples have been moved due to harmful assimilation policies, including off reservations and to urban locations. Although it remains unexplored, the careful development of these tools may have generated cognitive assessments that are more accessible for all peoples, potentially creating opportunities for Indigenous‐centered tools to be the standard, rather than the exception.
Future epidemiological studies must build upon these culturally adapted instruments; they must embed diagnostic approaches within community settings. Such approaches strengthen community‐led diagnostic pathways, enhance local capacity for brain health promotion, and strengthen community–clinician relationships. To capture the impact of dementia more accurately, surveillance strategies should include governance by Indigenous organizations to enable trust and ensure reliable identification of Indigenous peoples, include younger cohorts and develop normative data derived from Indigenous persons.42
STRUCTURAL CONTRIBUTORS TO DEMENTIA RISK AND PREVENTION
3
Much of the observed variation in dementia epidemiology is attributed to the biomedical risk factors model that neglects the broader contextual determinants that build cognitive reserve and resilience across the life course and shape dementia vulnerability.43 Although Indigenous communities globally have made significant strides in asserting sovereign autonomy and reclaiming land rights and cultural heritage, non‐Indigenous systems and structures constrain the capacity of Indigenous peoples to enact meaningful changes to modify dementia risk.44, 45 We cannot ignore history in shaping the future.
Modifiable dementia risk factors and social determinants of brain health
3.1
The 2024 Lancet Commission on dementia prevention and care identified 14 potentially modifiable risk factors spanning early, mid‐, and late‐life stages, representing ≈45% of dementia cases that could theoretically be prevented or delayed through targeted lifestyle interventions.46 These lifespan risk factors—educational attainment, hearing loss, vision loss, traumatic brain injury, hypertension, high cholesterol, alcohol consumption, obesity, smoking, depression, social isolation, physical inactivity, diabetes, and air pollution—are fundamentally intertwined with structural determinants and socioeconomic conditions. Emerging research among Indigenous populations reveals both shared risk patterns and distinct community‐specific expressions shaped by historical, cultural, and environmental contexts.47, 48, 49
Educational attainment is generally viewed as a cornerstone of early‐life brain health protection, with each additional year of formal/Western education associated with a reduced risk of dementia.46 The inheritance of intergenerational cultural knowledge and practices such as journey‐based experiences, storytelling, medicinal plant knowledge, and craftsmanship is likely to strengthen cognitive resilience among Indigenous peoples.50 Yet, most dementia‐related literature and research continue to focus narrowly on the association between reduced years of formal education and elevated odds of dementia, including among Indigenous populations across Australia,51 Canada,52 Malaysia,53 the United States,54 Brazil,9, 10 and Bolivia.11
Using years of formal education as the metric, population attributable risk analyses reveal that educational limitations contribute disproportionately to dementia burden among Aboriginal and Torres Strait Islander peoples in Australia and Māori populations in Aotearoa New Zealand compared to respective non‐Indigenous populations,47, 48 and formal educational attainment is associated with better cognitive health among Indigenous older adults in the United States.55 Although culturally adapted cognitive screening tools represent important progress, many continue to reflect aspects of their original Western test design and task structure.56 This approach may advantage individuals with some level of formal education, potentially inflating the apparent protective effect of formal schooling. For example, among the Tsimane, an Indigenous Amazonian community in Bolivia, dementia prevalence is extremely low despite minimal formal education.11 In contrast, studies in multiethnic urban Indigenous communities in the Brazilian Amazon found no association between education and dementia prevalence, likely reflecting uniformly low education levels and high illiteracy.9 Educational attainment may therefore function more as an indicator of socio‐cultural advantage.
These studies highlight the importance of developing epistemologically valid approaches, including Indigenous research methodologies, that recognize local knowledge systems and pathways of cognitive resilience and actively decolonize research practices.57 Conventional education metrics may be a poor proxy for baseline cognitive function in many Indigenous contexts, where the quality of schooling has varied considerably due to culturally inappropriate curricula, histories of exclusion from and abuse in educational institutions, and the dispossession of intergenerational cultural knowledge.58 The impact of residential or boarding school attendance and the consequent trauma and anxiety when undergoing formal cognitive testing is underappreciated.59 Contemporary research suggests that improved access to stimulating employment opportunities, traditional knowledge acquisition, and generative volunteering activities may serve as more culturally relevant proxies for lifelong cognitive stimulation among Indigenous populations.19, 55, 60, 61
Employment security, adequate housing, and income stability lay the foundation for brain‐healthy behaviors by mitigating poverty‐related risks and enabling access to protective resources.62 Globally, Indigenous households experience poverty rates two to three times higher than national averages, with associated cascading effects on multiple dementia risk pathways.63 Economic disadvantage restricts access to nutritious food sources, safe environments for physical activity, and access to preventive health services. Geographic remoteness exacerbates health care accessibility barriers for many Indigenous communities in both HICs and LMICs.64 Concurrently, urban migration can reduce intergenerational caregiving networks, amplifying social isolation in older adults.65 For example, in a study of the Mura Indigenous Tribe in a remote area of Amazonas, Brazil, completing a full functional assessment for dementia was not possible due to a lack of reliable information from family or close community members, illustrating intergenerational challenges.9 These socioeconomic constraints contribute directly to the greater prevalence of established biomedical risk factors during midlife, including increased cardiometabolic disease burden, higher rates of alcohol and tobacco use, vision loss, and untreated hearing loss.6, 66, 67
Indigenous populations residing in LMICs confront additional structural barriers that limit risk‐reduction opportunities, including competing health priorities such as infectious diseases and systemic challenges in implementing prevention strategies.68 Resource extraction (oil, mining, logging) and large‐scale agricultural industries in the Amazon and parts of Africa displace communities, erode food sovereignty, and increase exposure to environmental toxins (e.g., heavy metals, pesticides) that directly affect brain health.69, 70, 71 Similar patterns have been documented in North America, where proximity of Indigenous groups to mining operations, industrial waste sites, and contaminated water sources has led to elevated exposures to neurotoxic metals among Indigenous communities.72 These LMIC‐specific and cross‐regional exposures necessitate inclusion of an environmental focus during history‐taking and resource‐appropriate prevention frameworks that acknowledge both universal risk factors and region‐specific determinants.
Colonial context and ongoing impacts on brain health
3.2
At the root of social and health equity considerations are Indigenous determinants of health.73 Colonial policies of dispossession, societal and language assimilation, religious missions, and cultural suppression created systematic disruptions that have direct implications for life course cognitive resilience for Indigenous peoples, with these impacts passed intergenerationally and enduring today.43
The forced removal of Indigenous people from ancestral territories represents a profound structural intervention that disrupted place‐based knowledge systems and collective identity, both critical elements of cognitive, social, and emotional well‐being.74 Historical and ongoing traumas establish chronic stress pathways beginning in early childhood and contribute to age‐related neuroinflammation and neurodegeneration.75, 76 Markers of childhood adversity, including separation from family and frequent relocation, have been associated with the development of Alzheimer's disease in Aboriginal and Torres Strait Islander people in Australia.77 Lifetime discrimination experiences have also been shown to contribute to lower baseline cognitive scores and progressive cognitive change over time among Indigenous older adults in the United States.78 Colonial legacies, although varying across contexts, consistently undermine Indigenous determinants of brain health and cognitive resilience, underscoring the need for systemic transformations at all levels of society. Emerging research highlights the importance of cultural and political determinants of health, including the ways Indigenous peoples assert self‐determination, as key to health and well‐being, including brain health.
INTEGRATING INDIGENOUS PERSPECTIVES INTO BRAIN HEALTH AND DEMENTIA CARE
4
For many Indigenous communities, cognitive changes in later life reflect holistic frameworks. As such, protective factors for brain health and dementia caregiving are often framed collectively, challenging Western biomedical frameworks and government‐funded systems of support that focus on the individual.
Indigenous brain health in the context of cognition, ageing, and dementia
4.1
There is growing recognition of cultural approaches to cognitive health and aging among Indigenous populations.26, 32, 79, 80, 81, 82 In some Indigenous cultures, these changes are interpreted as a form of transition that draws individuals closer to ancestral knowledge and spiritual continuity.83, 84, 85, 86 Accordingly, dementia may be accepted in Indigenous communities, with family and community members emphasizing inclusion of older Māori in cultural activities, for example.32 In some settings, preservation of brain health is approached collectively, reinforcing intergenerational responsibilities and sustaining cultural knowledge transmission.27 However, limited awareness of the pathological underpinnings of dementia, compounded by negative past experiences with health care systems, may contribute to underdiagnosis and feelings of shame and stigma surrounding cognitive decline.26, 80, 87 These dynamics are further complicated by the marginalization of Indigenous perspectives within health care services, which often fail to engage meaningfully with local cultural and linguistic frameworks.32, 43 Optimizing dementia prevention and care requires the development of educational and health policy approaches that sustain cognitive health for the collective.
Support for culturally protective approaches to brain health
4.2
Acknowledging the centrality of culture, kinship, and connection to land and community broadens perspectives on brain health beyond biomedical framings.88 A decisive move away from deficit‐based narratives also illuminates how cultural assets and inherent resilience within Indigenous communities can be leveraged as powerful neuroprotective resources.89
Indigenous perspectives and lived experience accentuate the relationship between social connection, holistic concepts of well‐being, and cognitive resilience.90 Evidence already demonstrates that social isolation is a major risk factor for neurodegeneration.46 Research among Māori peoples in Aotearoa New Zealand and Aboriginal and Torres Strait Islander peoples in Australia reveals significantly lower rates of social isolation than respective non‐Indigenous populations, reflecting the foundational importance of whānau (family) and community structures.47, 48 Strengthening these elements through cultural participation and intergenerational engagement challenges Western biomedical frameworks, which frequently isolate dementia as a disease of the individual.83, 87
Other avenues for promoting brain health among Indigenous populations, grounded in traditional knowledge and practices such as dance, language, and social connection show promise in reducing dementia risk globally. For example, in Brazil, federal initiatives arising from sustained Indigenous advocacy promote Indigenous languages and cultures through the adoption of bilingual and intercultural curricula and Indigenous teacher training.91 In the United States, the Strong Heart Study is collating evidence on how self‐perception, identity, and cultural factors influence cognitive health among American Indian adults.34 In Hawai'i, the Kā‐HOLO study used hula, a traditional Native Hawaiian dance and cultural practice, as the foundation for a culturally grounded lifestyle intervention that significantly improved hypertension, self‐care, and cardiovascular risk.92 This approach has since been adapted to target vascular and metabolic risk factors for dementia among Native Hawaiians and Pacific Islanders as part of the ‘IKE Kupuna (Elder Wisdom) project.93 Highlighting the importance of involving young people in brain health approaches, the Hā Kūpuna National Resource Center for Native Hawaiian Elders also developed a community‐informed dementia educational storybook for Native Hawaiian youth.94 In Australia, the Sharing the Wisdom of our Elders project enhances dementia prevention knowledge through cultural expression and intergenerational learning,95 while the first randomized controlled trials examining community‐led approaches to reduce dementia risk in Aboriginal communities are also underway.96, 97 Taiwan's “Dementia Classrooms” and “Intergenerational Learning Programs” integrate Indigenous language education with Elder‐led cultural activities, preserving cultural heritage while supporting cognitive health.98 Indigenous‐led innovations like these demonstrate culturally grounded pathways to dementia prevention and underscore the leadership of Indigenous communities in advancing global brain health equity.
Quality and cultural propriety of dementia care
4.3
Within Indigenous communities, caregiving often occurs collectively, with decision‐making shared across family or kinship networks.32 These relational approaches challenge Western egocentric norms in health care, such as individual consent and autonomy, which may be culturally incongruent.27 Indigenous‐led, strengths‐based models of care offer clinicians, policymakers, and researchers pragmatic strategies to engage respectfully and collaboratively with Indigenous peoples.99, 100 Such models prioritize social and cultural reconnection, for example, enabling Elders to age in place,101 rather than defaulting to institutionalization or exclusively medical management.102, 103
Across the world, Indigenous‐led and collaborative initiatives are transforming dementia care. In Canada, the Peter Ballantyne Cree Nation's Integrated Care Model offers valuable lessons in shared caregiving for First Nations Elders,104 whereas in the United States, research collaborations such as the Northwest Tribal Elders Project105 and the ‘Auamo Kuleana O Nā Maʻi Poina in Hawai'i106 provide important models for culturally appropriate training and resource development for caregivers and providers. The longstanding Strong Heart Study exemplifies how enduring partnerships between American Indian communities and research institutions can produce both scientific insight and tangible community benefit.107 In Australia, the Let's CHAT (Community Health Approaches To) Dementia program represents a significant national initiative that co‐designed models of care within Aboriginal and Torres Strait Islander health services, demonstrating early promise in improving dementia diagnosis and management.108, 109 The partnership between Te Hau Ora o Ngāpuhi and the University of Auckland in Aotearoa New Zealand demonstrates meaningful integration of Māori cultural values and practices into dementia care,110 while partnerships in Manaus, Brazil, are informing national dementia policy through community‐based research.111
These initiatives show that culturally responsive dementia care is achievable when it is based on genuine partnership between Indigenous communities and research institutions. Yet they also underscore the sustained time, resources, and trust required to build and maintain such collaborations, challenges often at odds with short‐term funding cycles. Ensuring sustainability demands evaluation frameworks that pair Indigenous‐defined measures of success, such as community well‐being, cultural continuity, and family resilience, alongside conventional biomedical or clinical outcomes.
Integrating Indigenous approaches alongside biological advances
4.4
It is equally critical that Indigenous peoples are included in advances in understanding the genetic and biomarker signatures of dementia alongside culturally aligned approaches to prevention and care. Inclusion enables identification of both shared and unique risk and protective factors for cognitive ageing. Currently, the relationship between biomarkers and ethnoracial background remains poorly studied. A recent review found that investigations of Alzheimer's disease biomarkers in Indigenous groups is scarce, with most work focused on the apolipoprotein E (APOE) ε4 allele.6 Findings were inconsistent with half of the identified studies (n = 12) reporting no association between APOE ε4 and dementia and wide variation in allele prevalence (4.6%–24%) among Indigenous populations.112 Evidence from neuroimaging is similarly limited, with no positron emission tomography (PET) imaging or cerebrospinal fluid (CSF) biomarker research to date.
The lack of robust biomarker data underscores the need for more inclusive research approaches. Blood‐based biomarkers may be particularly valuable for their accessibility and cultural acceptability.113 However, biomarker thresholds must be validated in Indigenous populations rather than relying on cut‐points derived from predominantly non‐Hispanic White samples. The genetics of Alzheimer's disease in peruvian populations study in Peru, which included participants with an average of 80% Native American ancestry demonstrated that plasma phosphorylated tau‐217 (p‐tau217) was significantly associated with Alzheimer's disease, an important extension of the literature in this field.114 In the United States, the Strong Heart Study examined plasma markers in older American Indian adults and found significantly lower amyloid (amyloid beta [Aβ]42 and Aβ42/40) levels compared to non‐Hispanic White and other groups, suggesting a distinct trajectory of Alzheimer's disease pathology.115 The authors propose that American Indian individuals may experience earlier or accelerated amyloid accumulation, further highlighting that current dementia risk estimates may be understated.
Although the promise of biomarkers is clear, their application must be guided by robust ethical responsibility that ensure Indigenous research governance and adherence to relevant Indigenous ethics protocols. Research benefits must extend beyond typical Western scientific outputs to include tangible investments that reflect Indigenous peoples’ aspirations. These benefits may include culturally safe services to address prevention of brain health issues, health, education, and training of future Indigenous clinicians and researchers.
Advancing Indigenous leadership in dementia research and management
4.5
Many Indigenous communities are justifiably skeptical of health researchers given overwhelming histories and continuation of abuse and exploitation.116, 117 Despite this, older Indigenous peoples and advocates consistently express interest in collaborative research partnerships.83, 118, 119, 120 A new generation of Indigenous scientists is also growing in power within the academy, and is actively engaged in mentorship of the next generation.121, 122 In the United States, more than 12,000 American Indian and Alaska Native individuals have been awarded doctoral degrees since 2007, with similar trends emerging globally. These scholars are leading efforts to interrogate, decolonize, and embed Indigenous research methods. For example, one approach to advancing Indigenous health centers on analyzing unused data from Indigenous research participants whose contributions to science are often erased by limited efforts to disaggregate “other” racial and ethnic categories in longitudinal data.123
Modern statistical approaches allow meaningful inferences from smaller sample sizes, enabling more granular, population‐specific analyses. Yet researchers can be deterred by stringent data‐protection measures that slow research pipelines and impose strict security and reporting protocols.124 Informed by data sovereignty principles of ownership and access, these safeguards are essential for ensuring participant protection but can inadvertently limit Indigenous representation in dementia research. Indigenous scientists, however, are increasingly leading this work, supported by networks of Indigenous and non‐Indigenous mentors experienced in navigating these challenges. For example, the International Indigenous Dementia Research Network, founded in 2009, exemplifies such collaboration, bringing together over 200 scholars from Australia, Aotearoa‐New Zealand, Brazil, Canada, and the United States in 2024 to share scientific advances and mentorship. Initiatives like this strengthen Indigenous leadership in policy, research, and intervention development while fostering the next generation of Indigenous scholars.
Research and health policy implications
4.6
Developing Indigenous‐specific approaches to dementia prevention and care requires a paradigm shift in both research and health policy. Traditional biomedical models often fail to account for the political, sociocultural, and structural determinants that shape cognitive resilience in Indigenous communities. Rather than frame these approaches as “racialization” of dementia research,125 we advocate for the recognition and embedding of cultural frameworks, relational worldviews, and community engagement within health systems, research design, and publication standards (Figure 2).126, 127, 128 Strengths‐based community‐led models that prioritize cultural connection, community knowledge, and environmental stewardship have the potential to build cognitive reserve, and are highly relevant for everyone, yet remain underrepresented in national dementia strategies.129, 130
Achieving brain health equity with Indigenous peoples requires addressing the intersecting layers that shape cognitive resilience. These include structural determinants, environmental influences, health systems and service design, the quality of clinical, aged and disability care, and active engagement in decolonizing research and clinical practices. +The process of examining one's own cultural identity, biases, positioning and power, and reflecting on the potential influence on relationships. 128
Collecting data on structural and sociocultural determinants of health in Alzheimer's Disease Research Centers is a crucial step toward addressing inequities in dementia research.131 Integrating these approaches to knowledge creation will advance our understanding of population‐level dementia risks and improve our ability to quantify resilience against dementia. With enough advocacy, such approaches may create the opportunity to include data on the Indigenous determinants of health. The findings of the Lancet commission, alongside the broader literature of lifespan risk and protective factors for dementia, make it clear that the origins of dementia inequities are structural.49 They are also historical. Without robust frameworks for capturing the influence of systemic racism, colonial dispossession, and environmental injustice on cognitive health, health policies risk reinforcing existing disparities.
Effective implementation of preventative policies requires integrating Indigenous governance structures into policy development and respecting community protocols around data sovereignty.132 Research partnerships must be built on long‐term relationships, capacity strengthening, and co‐design principles that involve community leadership from the outset. Investment in culturally adapted diagnostic tools and education materials can enhance early detection and reduce stigma.10 Health workforce development is also critical, including training Indigenous clinicians and health scientists, and embedding cultural safety practices across all levels of dementia care and research.133
More broadly, holistic, community‐anchored, and strengths‐based strategies—long practiced in Indigenous contexts—point to preventive pathways that emphasize connection, identity, emotional well‐being, and the structural conditions that enable people to thrive. While any cross‐population application must remain grounded in Indigenous sovereignty, articulating how these principles may inform more responsive models of dementia risk reduction at the community level presents an important conceptual contribution to this field. Future work should therefore continue to prioritize Indigenous leadership while exploring the wider relevance of these approaches to reimagined brain health globally.
KEY RECOMMENDATIONS
5
It is not uncommon for well‐intentioned researchers and clinicians to seek guidance on how to “help” Indigenous communities. A central aim of this article is to demonstrate that Indigenous communities and their allies are already leading efforts to preserve brain health globally. What is needed now is genuine partnership. The pain that dementia inflicts on Indigenous communities is magnified by the disproportionate loss that occurs when the memories of Elders fade—each life story represents an irreplaceable link to collective histories, languages, and cultural knowledge. The urgency to prevent and treat dementias stems not only from a commitment to health equity, but from the existential threat these diseases pose to cultural continuity. The challenge before all scholars and practitioners is to act as respectful partners: to listen, learn, and support community‐driven solutions in the pursuit of brain health equity.
- Invest in Indigenous‐led brain health initiatives. Direct flexible funding to Indigenous‐controlled health services and Indigenous‐led research teams to develop culturally appropriate cognitive assessment, support programs, and dementia prevention initiatives.
- Address structural determinants of health through intersectoral approaches. Brain health equity requires policies that address Indigenous peoples’ sovereignty, education, housing, food security, environmental protection, and economic opportunity.
- Broaden health prevention programs, including evidence‐based science, to optimize cognitive resilience. Support for cultural continuity, language revitalization, access to traditional foods, intergenerational knowledge transfer, and ceremonial participation represent novel approaches to prevention aligned with Indigenous values.
- Include Indigenous peoples as researchers, leaders, stewards, and participants in clinical trials and cohort studies to develop appropriate normative data, informed by Indigenous determinants of health and data sovereignty principles.
- Implement culturally safe, trauma‐informed, and strengths‐based dementia care models that privilege Indigenous healing practices, honor Indigenous human rights, respect cultural protocols surrounding aging and end‐of‐life care, and are supported by sustainable, long‐term funding.
- Build the clinical and research workforce capacity. Increase pathways for Indigenous participation in health professions, sciences and leadership through scholarships, mentorship programs, and curriculum reform in health professional and health sciences education. Support non‐Indigenous clinicians and researchers to be critically reflective and engage in decolonizing practices.
APPENDIX: COLLABORATORS
AUTHOR CONTRIBUTIONS
Antonia J Clarke: Conceptualization; visualization; writing—original draft; writing—review and editing. Cliff Whetung: Conceptualization; writing—original draft; writing—review and editing. Astrid Suchy‐Dicey: Conceptualization; visualization; writing—review and editing. Adrienne Withall: Visualization; writing—review and editing. Kylie Radford: Conceptualization; visualization; writing—review and editing. Diane C Gooding: Conceptualization; writing—review and editing. Louise Lavrencic: Writing—review and editing. Makarena Dudley: Conceptualization; writing—review and editing. Dina Lo Giudice: Writing—review and editing. Leon Flicker: Writing—review and editing. Arantxa Sanchez Boluarte: Conceptualization; writing—review and editing. Sulakshna Aggarwal: Conceptualization; writing—review and editing. Kyle Conniff: Conceptualization; writing—review and editing. Amy G Brodtmann: Conceptualization; writing—review and editing. Monica M Diaz: Conceptualization; writing—review and editing. Stéfanie Tremblay: Conceptualization; writing—review and editing. Emmanuel S Nwofe: Conceptualization; writing—review and editing. Carey E Gleason: Conceptualization; writing—review and editing. Kristen Jacklin: Writing—review and editing. Joseph Keawe'aimoku Kaholokula: Writing—review and editing. Chontel Gibson: Conceptualization; writing—original draft; writing—review and editing. Juliana Souza‐Talarico: Conceptualization; writing—original draft; writing—review and editing. Pamela Roach: Conceptualization; writing—original draft; writing—review and editing.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest arising from the research, authorship and/or publication of this article. Any author disclosures are available in the Supporting Information.
Supporting information
Supporting Information
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Udeh‐Momoh CT , Migeot J , Blackmon K , et al. Resilience and brain health in global populations. Nat Med. 2025;31:2518–2531. doi:10.1038/s 41591-025-03846-w 40731089 · doi ↗ · pubmed ↗
- 2Lambrou NH , Blind MJ , Ketcher D , et al. Indigenous cultural understandings of Alzheimer's disease and related dementias – research and engagement (ICARE): relationships between cultural strengths, education and stigma. Alzheimers Dement. 2022;18:e 066094. doi:10.1002/alz.066094 · doi ↗
- 3Lowitja Institute . Social and emotional wellbeing: a review. Lowitja Institute; 2025. doi:10.48455/4F 9E-3V 29 · doi ↗
- 4Furlano JA , Okada De Oliveira M , Pintado‐Caipa M , Röhr S . Dementia prevalence and dementia risk in Indigenous Peoples: recent findings, current developments, and future directions. Curr Opin Psychiatry. 2025;38:119–125. doi:10.1097/YCO.0000000000000987 39804216 · doi ↗ · pubmed ↗
- 5Clarke AJ , Christensen M , Balabanski AH , et al. Prevalence of dementia among Indigenous populations of countries with a very high Human Development Index: a systematic review. Lancet Healthy Longev. 2024;5:100658. doi:10.1016/j.lanhl.2024.100658 39709981 · doi ↗ · pubmed ↗
- 6Nguyen HXT , Bradley K , Mc Namara BJ , Watson R , Malay R , Lo Giudice D . Risk, protective, and biomarkers of dementia in Indigenous peoples: a systematic review. Alzheimers Dement. 2024;20:563–592. doi:10.1002/alz.13458 37746888 PMC 10917055 · doi ↗ · pubmed ↗
- 7Warren LA , Shi Q , Young K , Borenstein A , Martiniuk A . Prevalence and incidence of dementia among indigenous populations: a systematic review. Int Psychogeriatr. 2015;27:1959–1970. doi:10.1017/S 1041610215000861 26088474 · doi ↗ · pubmed ↗
- 8de Souza‐Talarico JN , de Carvalho AP , Brucki SMD , Nitrini R , de Ferretti‐Rebustini RE . L. dementia and cognitive impairment prevalence and associated factors in indigenous populations: a systematic review. Alzheimer Dis Assoc Disord. 2016;30:281–287. doi:10.1097/WAD.0000000000000140 26840546 · doi ↗ · pubmed ↗