Subacute pacemaker lead migration with cardiac perforation and extracardiac extension into lung parenchyma with associated pneumothorax
Alyssa Liang, Vanessa L. Starr, Snehal Adodra, Praveen Anchala, Mohammad H. Madani

TL;DR
A rare case of pacemaker lead migration causing heart and lung complications is presented with detailed imaging.
Contribution
The paper presents a unique case of subacute pacemaker lead migration with extracardiac extension and pneumothorax.
Findings
Pacemaker lead migrated subacutely, perforating the heart and extending into lung tissue.
The complication resulted in a left-sided pneumothorax.
Imaging confirmed involvement of multiple cardiac and thoracic structures.
Abstract
Cardiac perforation with extracardiac extension by a pacemaker lead is a rare but serious complication of pacemaker placement. We present a unique case with imaging of a patient who underwent pacemaker placement complicated by subacute migration of the pacemaker lead, resulting in perforation involving interventricular septum, right ventricular apex, pericardium, epicardial fat, pleura and left upper lobe parenchyma with left-sided pneumothorax.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
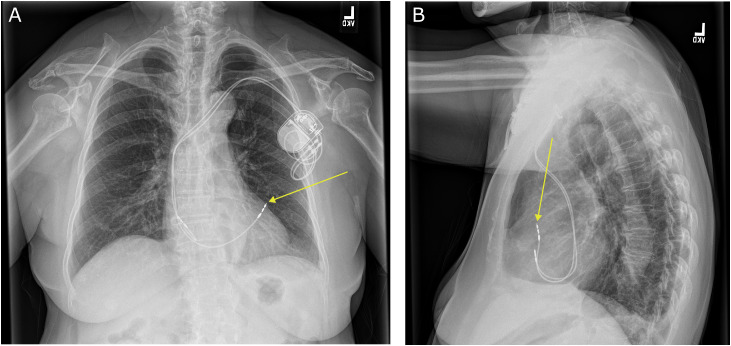 Figure 1
Figure 1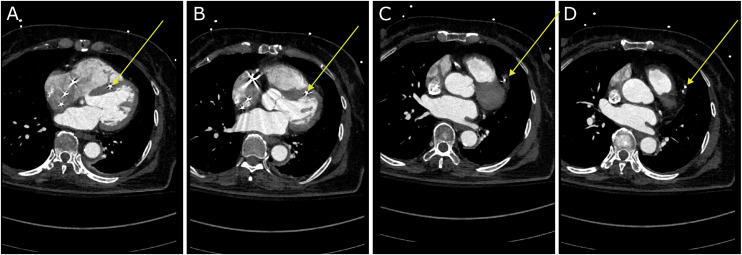 Figure 2
Figure 2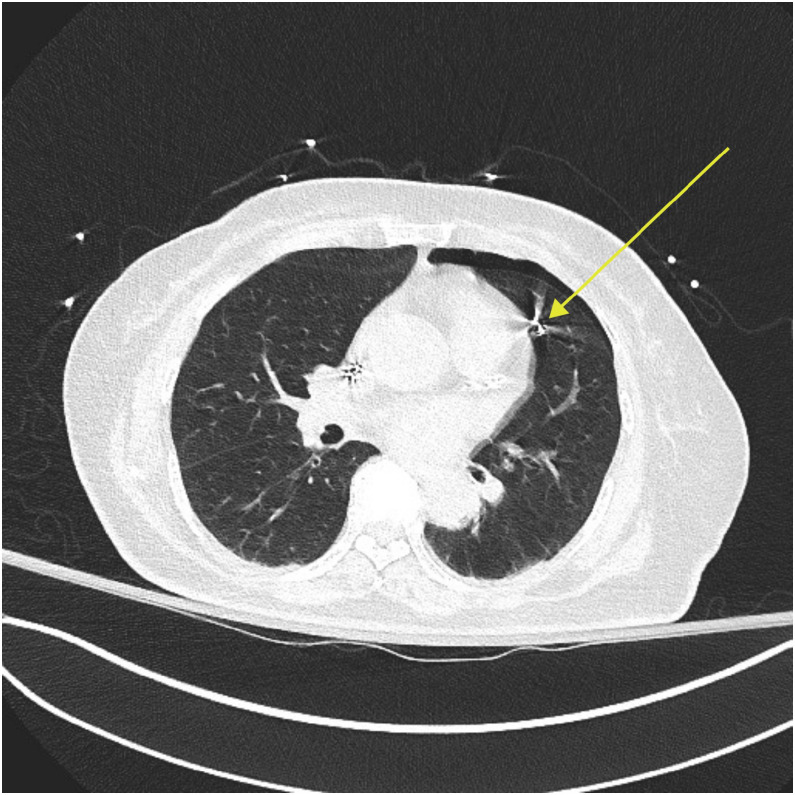 Figure 3
Figure 3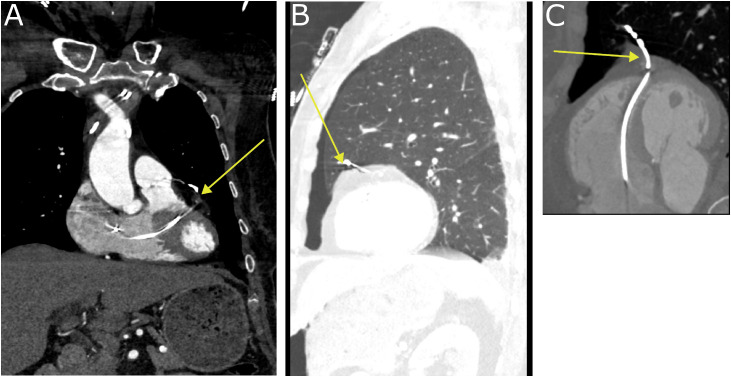 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphatic Disorders and Treatments · Trauma Management and Diagnosis · Pericarditis and Cardiac Tamponade
Introduction
Cardiac perforation and pneumothorax are both rare but potentially life-threatening complications of pacemaker placement, with an approximately 0.4% incidence of cardiac perforation [1] and a 1.3% incidence of pneumothorax [2]. While pneumothorax is more commonly typically seen as a complication of pacemaker placement due to complication of venous access during the pacemaker placement [2,3], cases of right ventricular [4] and right atrial perforation [[5], [6], [7], [8]] due to pacemaker lead migration have been reported with resulting contralateral pneumothorax. Right ventricular perforation may occur as an acute complication within 24 hours of pacemaker placement [4] or as a subacute to chronic complication occurring days to months after pacemaker placement [[9], [10], [11], [12], [13], [14]].
We present a case of a 78-year-old female patient who underwent pacemaker placement complicated by pacemaker lead migration, resulting in the second reported case of subacute right ventricular perforation with extracardiac extension of perforation and left-sided pneumothorax.
Case presentation
A 78-year-old woman with a history of hypertension, hyperlipidemia, type 2 diabetes, nonischemic cardiomyopathy, sick sinus syndrome, and tachy-brady syndrome, underwent dual-chamber pacemaker placement. She tolerated the procedure well without immediate complications and was discharged 2 days later.
14 days after pacemaker placement, she presented for follow-up at the cardiac device clinic, and reported a cough and sensation of chest pressure. Device interrogation of the pacemaker revealed a malfunction of the right ventricular lead, with greater than 2000 ohms of impedance and noncapture at the highest threshold in both unipolar and bipolar modes of the pacemaker. There was an initial concern for lead fracture. A chest radiograph showed intact pacemaker leads, but it also showed right ventricular lead migration and a small left pneumothorax (Fig. 1), and she was directed to proceed to the emergency department for further evaluation and management.Fig. 1. Posteroanterior (A) and lateral (B) radiograph of the chest. The dual chamber pacemaker generator is seen in the left upper chest wall. Pacemaker leads are intact. The atrial lead appears to be in placed in the right atrium. On frontal posteroanterior projection the tip of the right ventricular lead appears to project slightly beyond the cardiac border which is not evident on lateral view (yellow arrow). Small left apical pneumothorax is present.Fig 1 dummy alt text
In the emergency department, she reported continued cough, pain at the pacemaker placement site, and a sensation of substernal chest pressure, but denied shortness of breath. Her vital signs were within normal limits. Her EKG showed an atrial paced rhythm without other abnormalities. Cardiology was consulted, and recommended admission to the progressive care unit for cardiac monitoring.
She underwent a gated CT angiogram of the chest for further evaluation, which revealed that the right ventricular pacemaker lead had perforated through the interventricular septum and out through the apex of the right ventricle, passing through the myocardium, pericardium, and epicardial fat to continue through the pleural space and into the parenchyma of the left upper lobe with resulting left sided pneumothorax (Figs. 2, 3, and 4). In addition to the Cardiology service, Cardiothoracic Surgery was also consulted for removal of the perforating right ventricular lead. She was treated with supplemental oxygen through a nonrebreather mask to promote reabsorption of the pneumothorax, which spontaneously resolved 1 day later, and she remained hemodynamically stable throughout the admission.Fig. 2. Gated CT angiogram of the chest, showing the right ventricular lead migration through the (A) and (B) interventricular septum towards the apex, (C) through the apex, and (D) into the left upper lobe (yellow arrow).Fig 2 dummy alt textFig. 3Lung window of the same gated CT angiogram of the chest, showing the left-sided apical pneumothorax. The right ventricular lead can be seen traversing through the pericardium and passing into the left upper lobe of the lung (yellow arrow).Fig 3 dummy alt textFig. 4Multiplanar reconstructions from the above gated CT angiogram of the chest, showing the course of the right ventricular lead (yellow arrow) in coronal plane (A), sagittal plane (B), and along the plane of the interventricular septum (C).Fig 4 dummy alt text
3 days after admission, the right ventricular lead was successfully extracted transvenously in the catheter lab by the Cardiology service, with the Cardiothoracic Surgery team on standby in case of complications. The atrial lead was left in place to continue atrial pacing. The patient was closely monitored overnight in the Cardiac Care Unit. Her postoperative course was unremarkable, and she was ultimately discharged 5 days after admission.
Discussion
We represent a rare case of subacute right ventricular perforation with extracardiac extension of lead perforation through the epicardial fat, pleura and into lung parenchyma as a complication of pacemaker lead placement in an elderly female patient.
Cardiac perforation and pneumothorax are both rare but potentially life-threatening complications of pacemaker placement, with the incidence of cardiac perforation reported as 0.4% [1] and the incidence of pneumothorax as a complication of pacemaker placement to be 1.3% [2]. Cases of atrial perforation are more common than ventricular perforation due to the thinner muscular walls of the atria as compared to the ventricles [15]. Cases of right ventricular perforation occur must commonly at the apex, which is thinner and thus more easily perforated than the interventricular septum or right ventricular outflow tract [16]. This has led to suggestions that the thicker interventricular septum or right ventricular outflow tract should be used as alternate sites of lead placement in high-risk patients [14]. As with other cases of right ventricular perforation [4,9,[11], [12], [13], [14]], in this case the perforation also occurred at the apex of the right ventricle.
Women have a higher overall risk of all complications from pacemaker placement, and higher risk of pneumothorax and cardiac perforation in particular [17]. Risk factors for cardiac perforation include older age, steroid use within 1 week of implantation, use of a temporary transvenous pacemaker, BMI<20, use of helical screw ventricular leads, and longer fluoroscopy times [18]. Risk factors for pneumothorax include age>80 years, history of COPD, dual-chamber pacemaker implantation, and subclavian venous access [19]. In this case, this patient’s risk factors for cardiac perforation and pneumothorax included her age, sex, and dual-chamber pacemaker placement.
In previous cases of right ventricular perforation, 1 case of acute right ventricular perforation was associated with contralateral pneumothorax due to extracardiac pacemaker lead migration into lung parenchyma [4], and only 1 out of 9 cases of subacute to chronic ventricular perforation [[9], [10], [11], [12], [13], [14]] was associated with contralateral pneumothorax also due to extracardiac pacemaker lead migration into lung parenchyma. This case represents a second case of subacute right ventricular perforation with associated contralateral pneumothorax as a complication of pacemaker placement.
Of note, although the pneumothorax was initially identified on chest radiograph, the right ventricular perforation was not well visualized on radiography. However, CT clearly demonstrated the cardiac perforation with extracardiac extension. Prior cohort studies suggest that CT imaging has significantly higher accuracy, sensitivity, and specificity as compared to TTE or chest radiography for diagnosis of cardiac perforation, with an accuracy of 92.9% and a sensitivity of 97%-100% as compared to an accuracy of 61.1% and sensitivity 27.7% for chest radiography and an accuracy of 62.7% and sensitivity of 41.2% for transthoracic echocardiography [20,21]. Similarly to a previous case of lead migration where cardiac perforation was not evident on radiograph and only visualized on CT [10], this case demonstrates the superior sensitivity and anatomic detail of CT compared with radiography in diagnosing cardiac perforation and defining the extent of extracardiac lead migration.
Conclusion
Cardiac perforation with extracardiac extension into lung is a rare but potentially life-threatening complications of pacemaker placement, and the risk for these complications is higher in female patients and in the elderly. Cardiac perforation may not be well visualized on chest radiograph, and CT imaging is the gold standard in diagnosis of this rare complication. Awareness of this potential complication would allow for expedited management thereby reducing morbidity and mortality.
Ethical statement
This study did not require institutional review board approval.
Patient consent
Written informed consent was obtained from the patient for the publication of this article and accompanying imaging.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vamos M.Erath J.W.Benz A.P.Bari Z.Duray G.Z.Hohnloser S.H.Incidence of cardiac perforation with conventional and with leadless pacemaker systems: a systematic review and meta-analysis J Cardiovasc Electrophysiol 283201733634610.1111/jce.1314027925339 · doi ↗ · pubmed ↗
- 2Ogunbayo G.O.Charnigo R.Darrat Y.Morales G.Kotter J.Olorunfemi O.Incidence, predictors, and outcomes associated with pneumothorax during cardiac electronic device implantation: a 16-year review in over 3.7 million patients Heart Rhythm 141220171764177010.1016/j.hrthm.2017.07.02428735733 · doi ↗ · pubmed ↗
- 3Olesen L.L.Bilateral pneumothorax complicating pacemaker implantation, due to puncture of the left subclavian vein and electrode perforation of the right atrium Cureus 12112020 e 1130210.7759/cureus.11302 PMC 771638533282579 · doi ↗ · pubmed ↗
- 4Iwata S.Hirose A.Furui I.Matsumoto T.Ozaki M.Nagasaka Y.Right ventricular perforation, pneumothorax, and a pneumatocele by a pacemaker lead: a case report JA Clin Rep 7120216910.1186/s 40981-021-00470-834505188 PMC 8429537 · doi ↗ · pubmed ↗
- 5Nantsupawat T.Li J.M.Benditt D.G.Adabag S.Contralateral pneumothorax and pneumopericardium after dual-chamber pacemaker implantation: mechanism, diagnosis, and treatment Hear Case Rep 46201825625910.1016/j.hrcr.2018.03.001PMC 600648329922585 · doi ↗ · pubmed ↗
- 6Hegwood E.Burkman G.Maheshwari A.Risk for contralateral pneumothorax, pneumopericardium, and pneumomediastinum in the elderly patient receiving a dual-chamber pacemaker: a case report of 2 patients with acute and chronic atrial lead perforation Hear Case Rep 99202368068410.1016/j.hrcr.2023.07.004PMC 1051191937746575 · doi ↗ · pubmed ↗
- 7Srivathsan K.Byrne R.A.Appleton C.P.Scott L.R.P.Pneumopericardium and pneumothorax contralateral to venous access site after permanent pacemaker implantation EP Eur 54200336136310.1016/S 1099-5129(03)00093-X 14753631 · doi ↗ · pubmed ↗
- 8Sebastian C.C.Wu W.C.Shafer M.Choudhary G.Pa℡P.M.Pneumopericardium and pneumothorax after permanent pacemaker implantation Pacing Clin Electrophysiol 285200546646810.1111/j.1540-8159.2005.40063.x 15869684 · doi ↗ · pubmed ↗