Resolution of long-standing persistent atrial fibrillation after coronary revascularization: a case report on this rare reversible cause of atrial fibrillation
Suresh Kumar Sukumaran, Rahul Aziz Seena, Sasinthar Rangasamy, Sathish Kumar Subbaraj, Kannan BRJ

TL;DR
A man with long-term atrial fibrillation and heart disease regained normal heart rhythm after a procedure to improve blood flow to the heart, suggesting that heart artery blockage can cause atrial fibrillation.
Contribution
This case report presents a rare instance where atrial fibrillation was reversed through coronary revascularization without ablation or antiarrhythmic drugs.
Findings
A patient with long-standing atrial fibrillation spontaneously converted to sinus rhythm after PCI for coronary artery disease.
Left ventricular function normalized within a month following the procedure.
The case suggests ischaemia may be a reversible cause of atrial fibrillation in some patients.
Abstract
Atrial fibrillation (AF) commonly coexists with coronary artery disease (CAD) due to overlapping risk factors. Although ischaemia can promote atrial arrhythmogenesis, sustained restoration of sinus rhythm after revascularization alone is unusual. A 55-year-old man with hypertension and long-standing persistent AF (three years) was referred for pulmonary vein isolation. Echocardiography showed mild LV dysfunction (LVEF 48%) and basal septal thinning. Rest 99mTc-sestamibi myocardial perfusion SPECT (MPS) demonstrated moderate apical and mild to moderate inferior wall defects; 18F-FDG PET/CT with myocardial suppression showed no focal myocardial FDG uptake to suggest active inflammation. Coronary angiography demonstrated critical proximal LAD stenosis (95%) and minor RCA disease (30%). Following LAD PCI (3 mm × 15 mm DES), the patient spontaneously converted to sinus rhythm within two…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
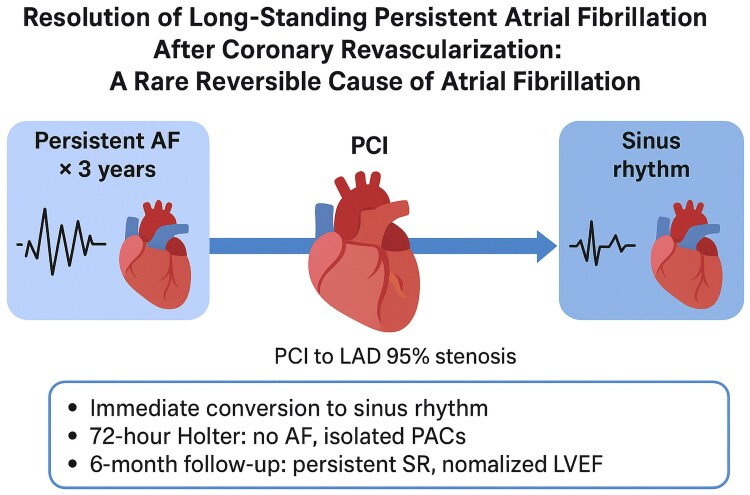 Figure 1
Figure 1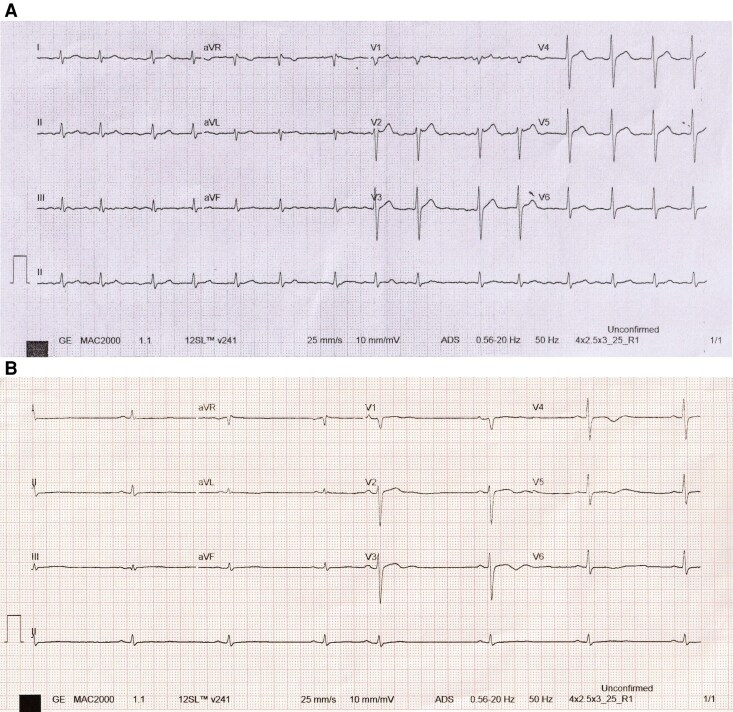 Figure 1
Figure 1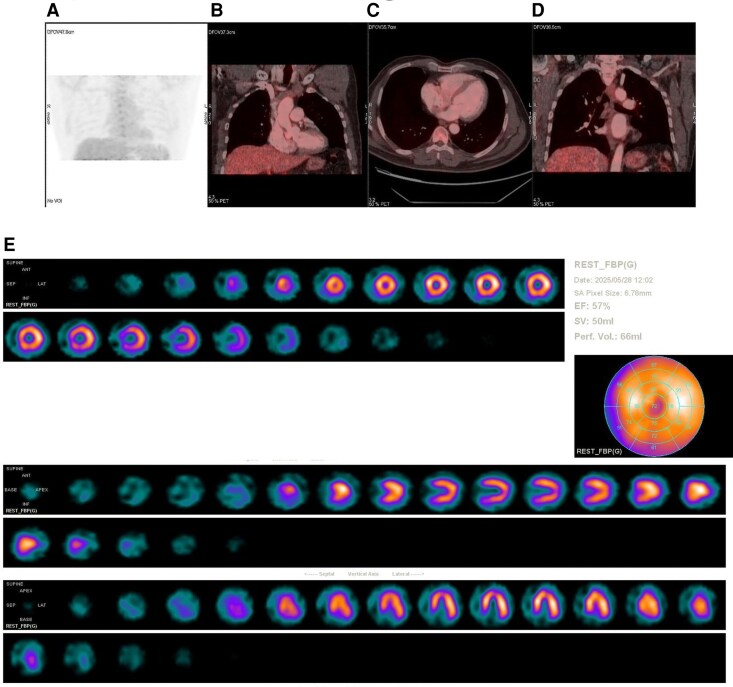 Figure 2
Figure 2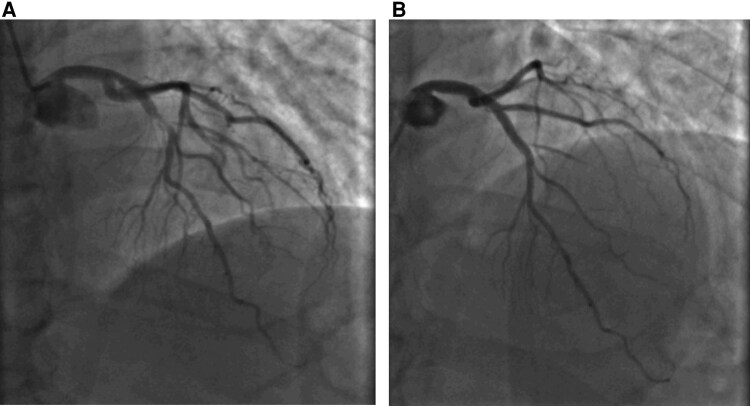 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Pericarditis and Cardiac Tamponade · Cardiac Arrhythmias and Treatments
Introduction
AF is the most common sustained arrhythmia, with major morbidity from stroke and heart failure.^1^ Mechanistically, AF reflects an interaction of focal triggers and atrial substrate remodelling under autonomic influence.^1–3^ Coronary artery disease (CAD) commonly coexists with AF due to shared risk factors,^2–4^ and observational studies report CAD in 17–46.5% of AF patients.^4–7^ While ischaemia can promote atrial electrical instability,^8^ durable restoration of sinus rhythm after coronary revascularization without ablation is rarely documented. We present a case of long-standing persistent AF reverting to sinus rhythm within hours of PCI, highlighting ischaemia as a potentially reversible cause.
Summary figure
**
Case presentation
A 55-year-old man with hypertension and persistent AF for three years (initially detected during pre-operative assessment) was referred for pulmonary vein isolation after pharmacologic cardioversion with amiodarone had failed. He was currently taking metoprolol 25 mg once daily, reported dyspnoea only at maximal exertion, and had no other limiting symptoms.
Examination revealed irregular rhythm; ECG showed atrial fibrillation with controlled ventricular rate (Figure 1A). Echocardiography showed mild global LV hypokinesia (LVEF 48%) and basal septal thinning (6.9 mm). Initially, he was planned for elective cardioversion, but concern for cardiac sarcoidosis prompted further advanced imaging, including Myocardial Perfusion Scintigraphy (MPS) and 18F-FDG PET scan before elective cardioversion.
Electrocardiogram. (A) Preoperative electrocardiogram demonstrates fine atrial fibrillation at approximately 90 bpm, with a normal QRS axis and duration, and without significant ST–T segment abnormalities. (B) Immediate postoperative electrocardiogram shows restoration of sinus rhythm at around 48 bpm, with occasional premature atrial contractions.
The myocardial suppression two-day protocol was used. 99mTc-sestamibi 8 mCi (≈296 MBq) was administered at rest with imaging at 60 min. For FDG PET, 18F-FDG 5.2 mCi (≈192 MBq) was injected after a 24-hour high-fat, very-low-carbohydrate diet and a 17-hour fasting period. Unfractionated heparin 4050 IU (≈50 IU/kg) was given 20 min before FDG, and fasting blood glucose was 105 mg/dL (≈5.8 mmol/L).^9^
Rest MPS demonstrated a moderate apical perfusion defect and mild to moderate mid—and basal-inferior wall defects. Limited cardiac 18F-FDG PET performed under a myocardial suppression protocol showed no focal or diffuse myocardial FDG uptake, arguing against active inflammatory/infective aetiology (Figure 2).^9,10^ Given the LAD-territory location of the apical abnormality and the equivocal nature of the inferior defects (where diaphragmatic attenuation is common), the nuclear medicine imaging impression favoured ischaemia —warranting invasive coronary evaluation.^11^
Nuclear medicine imaging. (A) Maximum-intensity projection (MIP) of cardiac 18F-FDG PET/CT after a myocardial-suppression protocol shows no focal or diffuse myocardial FDG uptake. (B–C) Fused PET/CT coronal and axial images with the heart in the field of view demonstrate physiologic myocardial FDG suppression. (D) Fused PET/CT coronal image focused on the mediastinum shows no FDG-avid lymphadenopathy. (E) Rest 99mTc-sestamibi myocardial perfusion scintigraphy (MPS): short-axis (SA), polar map, vertical long-axis (VLA), and horizontal long-axis (HLA) views demonstrate a moderate apical perfusion defect with mild–moderate mid- and basal-inferior defects.
Hence, coronary angiography was done first before elective cardioversion to avoid any potential complications, and that revealed a tight proximal LAD stenosis (95%) (Figure 3A) and a minor proximal RCA lesion (30%). The patient underwent PCI with implantation of a 3 × 15 mm drug-eluting stent in the LAD (Figure 3B). Two hours post-PCI, he spontaneously converted to sinus rhythm (Figure 1B). A 72-hour Holter recording in the immediate postoperative period revealed no atrial fibrillation, with only isolated premature atrial contractions (<0.1%). Over 6 months of follow-up, he has remained in sinus rhythm without antiarrhythmics, and the LV systolic function normalized within 1 month, and he is asymptomatic.
Coronary angiogram. (A) AP cranial coronary angiographic view demonstrating a critical 95% stenosis in the proximal left anterior descending artery. (B) AP cranial coronary angiographic view following deployment of a 3 mm × 15 mm stent across the proximal left anterior descending artery stenosis.
Discussion
Fundamentals of AF pathophysiology emphasize pulmonary-vein triggers operating on an atrial substrate shaped by fibrosis, dilatation, and metabolic/inflammatory stressors.^1–3^ Chronic hypertension and other cardiometabolic risks accelerate adverse remodelling, making long-standing persistent AF particularly resistant to spontaneous conversion; definitive rhythm control typically requires ablation or antiarrhythmic drugs.^1,5^
CAD is common among AF patients.^4–7^ In the AFFIRM cohort and other epidemiologic datasets, coexistence reflects shared risks and possibly direct ischaemic effects on atrial tissue.^4–6^ The atrial blood supply derives from the sinoatrial nodal/atrial branches—arising from the RCA in around 50–60% and the LCX in 40–50%—creating susceptibility to supply-demand mismatch and micro-ischaemia.^6^ Experimental studies elucidate mechanisms: Short-term atrial ischaemia via ionic/acid–base shifts (Na⁺/H⁺ exchange) shortens atrial refractoriness and fosters heterogeneity^12^; chronic coronary occlusion models increase AF triggers and maintenance.^13^
99mTc-sestamibi is a lipophilic cation that localizes in viable myocytes proportionally to blood flow and mitochondrial density, with minimal redistribution.^14^ On rest-only imaging, perfusion defects may reflect infarction/scar, prior ischaemic injury, or artefact; without attenuation correction or stress comparison, inferior wall artefact (e.g. diaphragmatic attenuation) and apical thinning cannot be excluded.^11,14^ 18F-FDG PET detects glucose-avid myocardial inflammation when physiological myocardial uptake is suppressed by dietary manipulation and fasting. Typical interpretive patterns include: (i) focal or focal-on-diffuse FDG uptake (± reduced perfusion) suggesting active inflammation; (ii) regions with reduced perfusion and absent FDG uptake suggesting scar; and (iii) reduced perfusion with preserved FDG uptake indicating viable hibernating myocardium.^9,10^ Rest perfusion defects on MPS together with absent myocardial FDG uptake argued against active inflammatory cardiomyopathy and, in the clinical context, suggested that ischaemia was also a contributor to both AF persistence and LV dysfunction—an inference supported by immediate post-PCI sinus rhythm restoration and rapid LVEF recovery.^9–11,14,15^
Clinical data on CAD’s impact on AF rhythm-control outcomes are mixed. The Leipzig registry (1310 patients) found no independent relationship between CAD presence/extent and post-ablation recurrence,^16^ and coronary stenosis location/severity did not predict outcomes in another imaging-guided study.^17^ Conversely, Hiraya et al. observed higher AF recurrence in CAD vs. non-CAD, with lower recurrence when PCI preceded PVI.^18^ Chen et al. similarly reported that obstructive CAD predicted poorer ablation success, while revascularization was associated with improved AF-free survival.^7^ Percutaneous transluminal coronary angioplasty may restore sinus rhythm in atrial fibrillation associated with acute coronary syndromes affecting the right or left circumflex coronary arteries.^19–21^ These divergent findings likely reflect heterogeneity in CAD severity, ischaemia burden, and whether revascularization addressed the active ischaemic driver of AF.
Our case is instructive in several respects. First, temporal proximity: conversion to sinus rhythm occurred within 2 hours of LAD revascularization, strongly suggesting ischaemia as the proximate mechanism rather than delayed remodelling.^7,12^ Second, durability: maintenance of sinus rhythm for 6 months without antiarrhythmics parallels observations that treating ischaemia can improve rhythm stability in selected CAD patients.^7,18^ Third, ventricular recovery: rapid LVEF normalization indicates reversible ischaemic cardiomyopathy rather than primary myopathic remodelling, aligning with an ischaemia-mediated atrial substrate or AF mediated cardiomyopathy.^12,13^ Finally, although atrial branches often originate from the RCA,^6^ LAD revascularization could still relieve atrial ischaemia via improved global perfusion, collateral flow, anatomical variability in atrial branch contribution, and reduced LV wall stress/left-atrial pressure, thereby stabilizing atrial electrophysiology.^12,13^
In contrast to cohorts showing no effect of CAD on ablation outcomes,^16,17^ this patient never required ablation; at least for the first 6 months, correcting the ischaemic supply–demand mismatch alone sufficed. Compared with series demonstrating benefit from PCI before ablation,^7,18^ our observation is an even stronger proof-of-principle that in a subset with ischaemia-driven AF, revascularization can be definitive. Pragmatically, these data support a work-up for occult ischaemia in AF patients with suggestive symptoms, LV dysfunction, perfusion defects, or high atherosclerotic risk, before committing to ablation.^4–7,16–18^
Certain constraints may affect the validity of this observation. Although the restoration of sinus rhythm occurred immediately after PCI, suggesting that myocardial ischaemia may have been a precipitating factor for AF, the contribution of rhythm restoration itself to LV function recovery cannot be excluded. AF-mediated cardiomyopathy may have also played a role in the initial LV dysfunction, and its reversal with sinus rhythm maintenance could have contributed to the observed improvement. Given the absence of a stress perfusion study, the relative impact of revascularization vs. rhythm normalization remains uncertain. While sinus rhythm was restored immediately following PCI and maintained during the 6-month follow-up, this temporal association alone does not establish causality. The possibility of spontaneous cardioversion cannot be excluded, and a longer follow-up period would be required to confirm durable rhythm stability.
Conclusion
In atrial fibrillation patients with coexisting CAD, ischaemia may be a reversible driver of arrhythmia. This case demonstrates immediate and sustained restoration of sinus rhythm after PCI without antiarrhythmics or ablation. Incorporating ischaemia evaluation into pre-ablation assessment may avert invasive procedures and optimize outcomes in selected individuals.^4–7,16–18^
Lead author biography
Dr. Suresh Kumar Sukumaran, MBBS, MD (General Medicine), DM (Cardiology), PDF (Cardiac Electrophysiology and Pacing), CCDS (IBHRE, USA), is a Consultant Cardiac Electrophysiologist and Interventional Cardiologist at Vadamalayan Hospitals and Postgraduate Institute of Medical Sciences, Madurai, Tamil Nadu, India. He completed his Fellowship in Cardiac Electrophysiology and Pacing (2022–2024) and DM in Cardiology (2019–2021) at JIPMER, Pondicherry, following his MD (2014–2017) and MBBS (2007–2013). Hosts a robust portfolio of research and clinical insights, evidenced across high-impact publications and advanced procedural expertise.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lip GY, Beevers DG. ABC of atrial fibrillation. History, epidemiology, and importance of atrial fibrillation. BMJ 1995;311:1361–1363.7496293 10.1136/bmj.311.7016.1361 PMC 2551280 · doi ↗ · pubmed ↗
- 2Krahn AD, Manfreda J, Tate RB, Mathewson FA, Cuddy TE. The natural history of atrial fibrillation: incidence, risk factors, and prognosis in the Manitoba follow-up study. Am J Med 1995;98:476–484.7733127 10.1016/S 0002-9343(99)80348-9 · doi ↗ · pubmed ↗
- 3Hohnloser SH, Crijns HJ, van Eickels M, Gaudin C, Page RL, Torp-Pedersen C, et al Effect of dronedarone on cardiovascular events in atrial fibrillation. N Engl J Med 2009;360:668–678.19213680 10.1056/NEJ Moa 0803778 · doi ↗ · pubmed ↗
- 4AFFIRM Investigators . Baseline characteristics of patients with atrial fibrillation: the AFFIRM study. Am Heart J 2002;143:991–1001.12075254 10.1067/mhj.2002.122875 · doi ↗ · pubmed ↗
- 5Crijns HJ, van Gelder IC, van Gilst WH, Hillege H, Gosselink AM, Lie KI. Serial antiarrhythmic drug treatment to maintain sinus rhythm after electrical cardioversion for chronic atrial fibrillation or atrial flutter. Am J Cardiol 1991;68:335–341.1907089 10.1016/0002-9149(91)90828-9 · doi ↗ · pubmed ↗
- 6James TN, Burch GE. The atrial coronary arteries in man. Circulation 1958;17:90–98.13511627 10.1161/01.cir.17.1.90 · doi ↗ · pubmed ↗
- 7Chen X, Zhao J, Zhu K, Qin F, Liu H, Tao H. Association between recurrence of atrial fibrillation and revascularization in patients with coronary artery disease after catheter ablation. Front Cardiovasc Med 2021;8:756552.34869668 10.3389/fcvm.2021.756552 PMC 8639697 · doi ↗ · pubmed ↗
- 8Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. J Am Coll Cardiol 2014;63:2335–2345.24613319 10.1016/j.jacc.2014.02.555 · doi ↗ · pubmed ↗