Renal Cell Carcinoma: Characteristics of Patients, Treatment, and Disease Progression Based on Real-World Data From a Cancer Center in Medellín, Colombia
Mauricio Lema, Camila Lema, Diego Morán, Mateo Pineda, Beatriz Preciado, Emilio Pérez

TL;DR
This study analyzes real-world data from a Colombian cancer center to describe the characteristics, treatment patterns, and survival outcomes of 208 renal cell carcinoma patients.
Contribution
The study provides the first real-world data on RCC in Colombia, including treatment patterns and survival outcomes in a Latin American context.
Findings
More than half of patients had metastatic disease at diagnosis or developed it later.
Non-metastatic status, low-risk classification, and first-line tyrosine kinase inhibitors were associated with better survival.
Only one-third of metastatic patients received second-line therapy, indicating treatment access challenges.
Abstract
Introduction Data on demography, stage distribution, treatment, and survival rates of renal cell carcinoma (RCC) in Colombia is not known. This study aims to describe a cohort of patients with RCC treated at the Clínica de Oncología Astorga, in Medellín, Colombia. Methods This retrospective study included all consecutive RCC patients treated at the institution between 2008 and 2023. Clinical, treatment, and survival data were collected from medical records. For metastatic and recurrent patients, risk was dichotomized as low-risk or non-low risk. The latter included those classified as intermediate/high risk in medical records, or cases with de novo metastatic disease or progression within 12 months of initial diagnosis. Event-free survival (EFS), progression-free survival (PFS), and overall survival (OS) were estimated using the Kaplan-Meier method and subgroup analysis was performed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1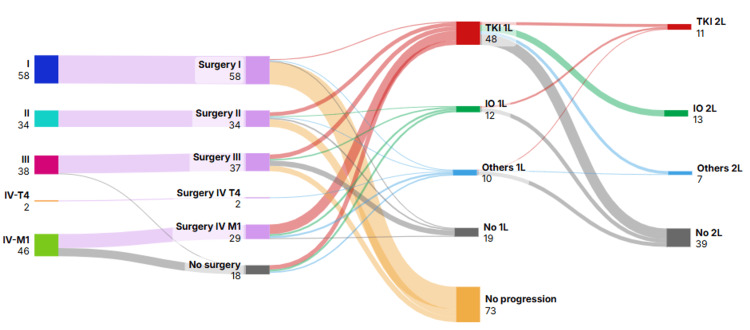 Figure 2
Figure 2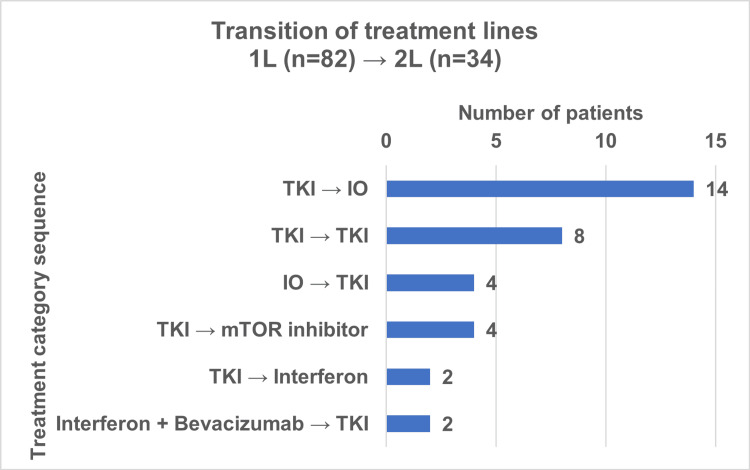 Figure 3
Figure 3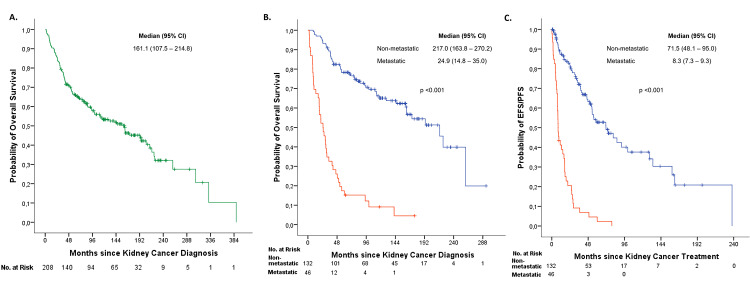 Figure 4
Figure 4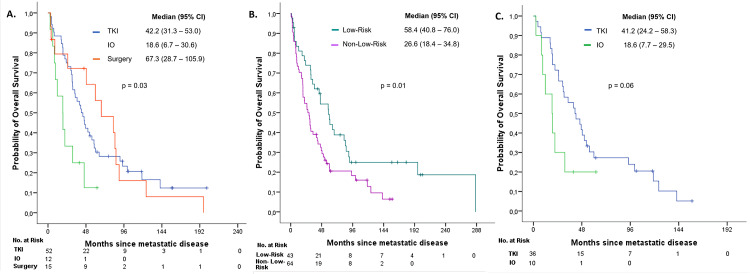 Figure 5
Figure 5| Characteristics | n (N=208) | % |
| Age (median (IQR)) | 60.4 years (51.9-69.8) | |
| Sex | ||
| Women | 94 | 45.2 |
| Men | 114 | 54.8 |
| Affiliation type to the healthcare system* | ||
| Contributive regime | 132 | 63.5 |
| Subsidized regime | 5 | 2.4 |
| Special regime | 4 | 1.9 |
| Private insurance | 67 | 32.2 |
| Histology | ||
| Clear cell | 167 | 80.3 |
| Clear cells with sarcomatoid features | 9 | 4.3 |
| Papillary | 12 | 5.8 |
| Sarcomatoid | 1 | 0.5 |
| Other† | 13 | 6.3 |
| Non-classified | 6 | 2.9 |
| Stage at diagnosis | ||
| I | 58 | 27.9 |
| II | 34 | 16.3 |
| III | 38 | 18.3 |
| IV (T4) | 2 | 1 |
| Unknown | 30 | 14.4 |
| Risk classification in metastastic disease | (n=107) | 51.4 |
| Low risk | 43 | 40.2 |
| Non-low risk | 64 | 59.8 |
| Second primary malignancy | ||
| Yes | 38 | 18.3 |
| Breast cancer | 7 | 3.4 |
| Prostate cancer | 6 | 2.9 |
| Colorectal cancer | 5 | 2.4 |
| Thyroid cancer | 4 | 1.9 |
| Lung cancer | 3 | 1.4 |
| Stomach cancer | 2 | 1 |
| Contralateral kidney cancer | 2 | 1 |
| Bladder cancer | 2 | 1 |
| Other§ | 7 | 3.4 |
| No | 170 | 81.7 |
| Treatment modality | Early-stage / locally advanced disease | Metastatic disease | Unknown stage at diagnosis | Complete cohort | ||||
| n | % | n | % | n | % | n | % | |
| (n=132) | (n=46) | (n=30) | (n=208) | |||||
| Nephrectomy followed by surveillance | 126 | 95.4 | 3 | 6.5 | 30 | 100 | 159 | 76.4 |
| Partial | 17 | 13.5 | 0 | 0.0 | 0 | 0.0 | 17 | 10.7 |
| Radical | 86 | 68.3 | 2 | 66.7 | 16 | 53.3 | 104 | 65.4 |
| Unknown | 23 | 18.3 | 1 | 33.3 | 14 | 46.7 | 38 | 23.9 |
| Nephrectomy followed by systemic therapy | 5* | 3.8 | 26† | 56.5 | 0 | 0 | 31 | 14.9 |
| TKI | 5 | 100 | 18 | 69.2 | 0 | 0 | 23 | 74.2 |
| IO | 0 | 0 | 3 | 11.5 | 0 | 0 | 3 | 9.7 |
| IO with TKI | 0 | 0 | 1 | 3.8 | 0 | 0 | 1 | 3.2 |
| Interferon with BVCZ | 0 | 0 | 2 | 7.7 | 0 | 0 | 2 | 6.5 |
| Chemotherapy | 0 | 0 | 2 | 7.7 | 0 | 0 | 2 | 6.5 |
| Systemic therapy alone | 1 | 0.8 | 15 | 33.3 | 0 | 0 | 16 | 7.7 |
| TKI | 1 | 100 | 8 | 53.3 | 0 | 0 | 9 | 56.3 |
| IO | 0 | 0 | 3 | 20 | 0 | 0 | 3 | 18.8 |
| IO with TKI | 0 | 0 | 1 | 6.7 | 0 | 0 | 1 | 6.3 |
| Interferon with BVCZ | 0 | 0 | 1 | 6.7 | 0 | 0 | 1 | 6.3 |
| mTOR inhibitor | 0 | 0 | 2 | 13.3 | 0 | 0 | 2 | 12.5 |
| Supportive care‡ | 0 | 0 | 2 | 4.4 | 0 | 0 | 2 | 1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal cell carcinoma treatment · Multiple and Secondary Primary Cancers · Biological Research and Disease Studies
Introduction
According to GLOBOCAN 2022, renal cell carcinoma (RCC) ranks as the 13th most common cancer worldwide [1]. In Colombia, RCC incidence was estimated as 2.0% and 1.5% of cancer-related deaths, corresponding to approximately 2,374 new cases and 829 deaths annually [1].
The risk factors for sporadic RCC are nonspecific and include smoking, obesity, high blood pressure, alcohol consumption, and occupational exposure to carcinogens. Hereditary RCC syndromes have also been described, accounting for a small fraction of cases. Due to its low relative frequency and the nonspecific nature of its risk factors, there is currently no established strategy for the early detection of RCC. This explains why approximately one in three cases of RCC is diagnosed at a locally advanced or metastatic stage [2]. The median age at diagnosis of RCC is 64 years. The five-year survival rates for RCC detected at localized, regional extension, and metastatic disease are 92.7%, 71.0%, and 13.9%, respectively [2].
This study aims to describe the demographic and clinical characteristics, as well as survival outcomes of 208 consecutive patients with RCC treated at Clínica de Oncología Astorga, an outpatient cancer care center in Medellín, Colombia.
Materials and methods
This is an observational, longitudinal, retrospective study of patients with RCC in a real-world setting at the Clínica de Oncología Astorga, in Medellín, Colombia. All RCC patients treated between January 1, 2008 and January 30, 2023 at the institution were considered for inclusion.
The medical records were reviewed to identify the eligible cases. Patients aged ≥18 years were included. Patients were excluded if they did not have a histological diagnosis, if clinical data related to diagnosis or treatment were insufficient, or if they had a confirmed diagnosis of urothelial carcinoma or metastatic involvement of the kidneys originating from other primary tumors.
Data was extracted from medical records. Demographic variables were collected. Clinical data included histological type (e.g., clear-cell, papillary, sarcomatoid, etc.) and stage at initial diagnosis. Information on treatment modalities, such as surgery, systemic therapies and/or supportive care, was also gathered.
Risk classification in metastatic disease was inconsistently reported. Therefore, patients were dichotomized into low-risk and non-low-risk categories. When risk classification was unavailable, patients were assigned to the non-low-risk category if they presented with de novo metastatic disease or if progression occurred within 12 months of the initial RCC diagnosis. The non-low-risk group included patients classified as intermediate or high risk in the medical records. The remaining patients were classified as low risk.
Survival outcomes assessed included the following: Event-free survival (EFS), defined as the time from initiation of treatment with curative intent to either disease progression or death, whichever occurred first. Progression-free survival (PFS), defined as the time from the start of treatment for metastatic disease to either disease progression or death, whichever occurred first. Overall survival (OS) is defined as the time from diagnosis to death from any cause. May 30, 2025, was defined as the cut-off date for collecting information on survival outcomes. Patients whose vital status could not be confirmed were censored at the date of their last clinical contact.
The date of death was obtained from reliable sources, including medical records, ADRES (Administradora de los Recursos del Sistema General de Seguridad Social en Salud) database, or Registraduría Nacional del Estado Civil database (another governmental institution).
Data from qualitative variables were summarized using absolute and relative frequencies. Quantitative variables were expressed as median and interquartile range (IQR), depending on their distribution. Survival was estimated using Kaplan-Meier method. Subgroup analysis was carried out according to metastatic disease and treatment; differences were assessed with the log-rank test. ESMO-GROW (European Society for Medical Oncology Guidance for Reporting Oncology real-World evidence) criteria were applied [3]. All analyses were conducted using SPSS version 22 statistical software (IBM Corp, Armonk, NY).
Ethical considerations
In accordance with Resolution 8430 of 1993, which establishes the scientific, technical, and administrative standards for health research in Colombia, this study is classified within the category of research without risk. Informed consent was not required since the study was a review of medical records, and patients were not subjected to any study-based intervention. Confidentiality was guaranteed by using data masking during the analysis process.
The study was approved by the Comité de Ética para la Investigación Clínica (CEIC) of the Fundación Centro de Investigación Clínica (CIC) on October 26, 2023, as documented in Act 467.
Results
Baseline characteristics
From 2008 to 2024, 283 patients with RCC were treated at the institution. Of these, 208 patients with RCC met the inclusion criteria (Figure 1).
Patient selection for renal cell carcinoma study in Medellín, Colombia.
In our cohort, 114 (54.8%) patients were men, and the median age was 60.4 years (IQR 51.9-69.8 years) at diagnosis. Clear cell renal cell carcinoma (ccRCC) was the histological diagnosis in 167 (80.3%) cases. Stage I and stage IV were assigned to 58 (27.9%) and 48 (23.1%) of cases, respectively. A second primary malignancy was found in 38 (18.3%) patients. Of these, the most common was breast cancer in seven (18.4%) patients (Table 1).
Treatment
Among patients with early-stage or locally advanced disease (stages I to IV - T4), 126 (95.4%) were treated with nephrectomy followed by surveillance. Nephrectomy followed by surveillance was the treatment for all 30 patients with unrecorded stage. Tyrosine kinase inhibitor (TKI) was the adjuvant therapy in five (100%) cases (Table 2). No patient underwent adjuvant pembrolizumab therapy because it was not approved in Colombia at that time.
Patients’ distribution according to initial stage and their pathway through different scenarios of disease are represented in Figure 2.
Treatment sequences in patients with renal cell carcinoma by stage.TKI: Tyrosine kinase inhibitor. IO: Immunotherapy. 1L: First line. 2L: Second line. Others: included chemotherapy, interferon plus bevacizumab, mTOR inhibitors, and interleukin-2.
Treatment for metastatic disease
In the total cohort, 46 patients presented with synchronous disease, while 61 developed metastases following the initial diagnosis (metachronous) (Table 1). Among the synchronous group, 29 (63.0%) patients underwent surgery with curative intent, all of whom subsequently experienced recurrence (Table 2).
Of the 107 patients with metastatic disease, 82 received first-line therapy. Among them, 58 (70.7%) patients were treated with TKI, 12 (14.6%) with immunotherapy (IO), and 12 (14.6%) with other systemic treatments, including chemotherapy, mTOR inhibitors, or interferon. A second line of treatment was administered to 34 patients (31.8%). In this scenario, 14 (41.2%) patients received TKI, 14 (41.2%) IO, four (11.7%) mTOR inhibitors, and two (5.9%) interferon.
Among the 34 patients who received a second-line regimen, the most common sequences were TKI followed by IO (n=14, 41.2%) and TKI followed by TKI (n=8, 23.5%). The aforementioned factors were responsible for approximately two-thirds of all treatment transitions (Figure 3).
Transition from first- to second-line therapy in metastatic renal renal cell carcinoma.TKI: Tyrosine kinase inhibitor; IO: immunotherapy; mTOR: mammalian target of rapamycin.
Outcomes
The median follow-up was 84.6 months (IQR 37.7-161.8) from diagnosis. At the time of analysis, 97 patients (46.6%) were alive. Median OS for the entire cohort was 161.1 months (95% confidence interval (CI): 107.5-214.8) (Figure 4A). Based on the stage at diagnosis, median OS was 217.0 months (95% CI: 163.6-270.4) for patients with early-stage or locally advanced disease (classified as non-metastatic). In contrast, patients presenting with metastases at diagnosis had a median OS of 24.9 months (95% CI: 14.3-35.5) (Figure 4B). A significant difference in OS was found between stage groups (p <0.001).
Among the 132 patients in the non-metastatic group, 59 (44.7%) experienced disease progression, whereas 45 (97.8%) of the 46 patients in the synchronous group experienced progression. Median EFS and PFS were 71.5 months (95%CI: 45.2-97.9) and 8.3 months (95%CI: 6.7-9.9), respectively (Figure 4C). A significant difference in EFS/PFS was observed between groups (p<0.001).
Kaplan–Meier curves for: (A) overall survival of the entire patient cohort, (B) overall survival by subgroups according to initial stage (non-metastatic vs. metastatic), (C) event-free survival (EFS) and progression-free survival (PFS) in patients with renal cell carcinoma..
Overall survival was assessed in patients who developed metastases (either synchronous or metachronous) and was stratified by first-line treatment for metastatic disease: TKI, IO, or surgery. Median OS was 42.2 months (95% CI: 31.3-53.0), 18.6 months (95% CI: 6.7-30.6), and 67.3 months (95% CI: 28.9-105.9), respectively. The differences observed among the groups were found to be statistically significant (p=0.03) (Figure 5A).
When further stratified by risk category, median OS was 58.4 months (95% CI: 40.8-76.0) in the low-risk group versus 26.6 months (95% CI: 18.4-34.8) in the non-low-risk group (p=0.01) (Figure 5B). Within the non-low-risk group, median OS was 41.2 months (95% CI: 24.2-58.3) for TKI and 18.6 months (95% CI: 7.7-29.5) for IO (p=0.06) (Figure 5C).
Kaplan–Meier curves for: (A) overall survival in patients according to the type of treatment received in metastatic disease, (B) overall survival by risk category in metastatic disease, and (C) overall survival within the non-low-risk group in metastatic disease by treatment (TKI vs. IO).
Discussion
This study provides one of the largest real-world descriptions of RCC in Colombia, providing insight into the demographic, clinical, and survival characteristics of patients treated at a specialized outpatient oncology center.
The median age at diagnosis in our cohort (60.4 years) was lower than the global median of 75 years reported in international registries [5,6]. This finding may reflect regional demographic patterns, potential differences in risk factor exposure, or earlier access to specialized care in a proportion of patients. In accordance with international data, the majority of cases were identified as clear cell RCC, which remains the most prevalent histological subtype worldwide [7].
In our cohort, the male-to-female distribution was nearly balanced (~55% men and ~46% women), which contrasts with the global epidemiological trend, which has been shown to exhibit a clear male predominance, with reported ratios of approximately 2:1 [8,9].
The proportion of patients diagnosed with advanced or metastatic disease in our cohort (22.1%) was comparable to figures reported in the literature, ranging from 17% in some series to approximately 25%-30% in others [8,10].
Treatment patterns in this study reflect the evolution of therapeutic availability in Colombia over the past decade. Nearly all patients with localized disease underwent nephrectomy, consistent with international standards of care [11,12]. In contrast, systemic therapy for metastatic disease was dominated by TKIs, with relatively limited use of immunotherapy. This pattern differs from current global practice, where immune checkpoint inhibitors (ICI), either alone or in combination with TKIs, are standard first-line therapy for advanced disease [13-15]. Many of the patients included in this analysis were treated in the TKI era prior to the ICI era. Additionally, delays in regulatory approvals in Colombia restricted access to ICIs. For example, in Colombia, there is still no regulatory approval of adjuvant pembrolizumab for resected high-risk RCC.
In our data, 46.3% of the patients did not receive a second-line agent for advanced RCC. The limited access to second-line therapy in our study is similar to that reported in two cohorts of patients with advanced kidney cancer in the United States and Rumania, where second-line treatment was reported in 48.4% and 51.3% of cases, respectively [16,17]. Given that a substantial proportion of patients may not have the opportunity to receive second-line therapy, the careful selection of the initial treatment strategy acquires even greater clinical relevance. It is imperative to underscore the recommendation of administering very active RCC treatments as a primary course of action, given that approximately half of the patients will only receive a first-line therapy.
Survival outcomes in our cohort are generally consistent with those reported in international series, although median OS in non-metastatic patients was notably long. This phenomenon may be partially attributed to several factors, including a relatively younger population, the high rate of surgical management, and the long follow-up period achieved in this study. In the metastatic subgroup, the median PFS of 8.3 months with first-line therapy is comparable to outcomes reported in the pre-immunotherapy era with TKIs alone [18,19].
A statistically significant discrepancy was identified in survival outcomes between patients with low-risk and non-low-risk disease. The median overall survival was 58.4 months versus 26.6 months, respectively. Among patients in the non-low-risk group, those treated with TKIs exhibited a numerically longer median survival of 41 months compared with 18.6 months in those treated with immunotherapy, although this difference did not reach statistical significance. Both results may be attributable to the small sample size within immunotherapy group.
An additional relevant observation was the occurrence of second primary malignancies in nearly one-fifth of patients, with breast cancer being the most frequent. While this phenomenon has been described in other series [20], its clinical implications remain uncertain. It raises questions regarding potential shared risk factors, genetic predispositions, or treatment-related effects that warrant further exploration in larger, multicenter studies.
This study has several limitations inherent to its retrospective and single-center design. Missing data in some variables, particularly stage and treatment details, could have introduced bias. Furthermore, therapeutic options have changed substantially over the long study period, limiting the direct comparability of survival outcomes with current international standards. Nonetheless, the strengths of this work include the relatively large sample size, accurate characterization of the patient population in terms of demographic variables and TNM stage, long follow-up, and robust survival data verified through national registries.
Another limitation of the study is that, due to the retrospective nature of the data, information on prognostic risk status according to the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) was not consistently available in the medical records. This prognostic classification is essential to better understand and accurately interpret treatment selection strategies in metastatic disease. We tried to minimize the impact of this shortcoming by creating the low- and non-low-risk categories for metastatic and recurrent disease to provide a rough estimate of risk distribution.
In Colombia, epidemiological statistics can be obtained from government sources and population-based registries (incidence, prevalence, and mortality) for patients with RCC [21,22]. However, to the best of our knowledge, there is an absence of other comprehensive description of RCC in Colombia, and it can be a reference point for future studies as a baseline. Navarro et al. published a description of 40 consecutive stage I-III RCC patients treated in Barranquilla, Colombia [23]. In this study, five-year follow-up was available in only 15 patients, and there were no stage IV patients included. In contrast, our dataset has a median follow-up of 85.6 months, which can accurately depict the long-term survival patterns of the patient population. It also included 45 stage IV RCC patients, adding valuable information on the outcome of this critically important subgroup for the clinical oncologic community.
Conclusions
In conclusion, this study found that demographic and clinical features of RCC patients in Colombia mirror global patterns. Therapeutic limitations, particularly restricted access to modern immunotherapy, continue to represent a major gap in the management of metastatic disease. Future efforts should focus on expanding access to contemporary systemic therapies, exploring strategies for earlier detection, and generating multicenter data to better characterize outcomes in the region.
This institution-based real-world study of patients with RCC diagnosis, treated at a single outpatient oncology center in Colombia, provides a comprehensive characterization of demographics, data, stage distribution, treatment patterns, and survival outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lyon, France: International Agency for Research on Cancer 1 2025 Ferlay J Ervik M Laversanne M e al.Lyon France: International Agency for Research on Cancer 2024 https://gco.iarc.who.int/today
- 2Epidemiology of renal cell carcinoma World J Oncol Padala SA Barsouk A Thandra KC 79871120203249431410.14740/wjon 1279 PMC 7239575 · doi ↗ · pubmed ↗
- 3ESMO Guidance for Reporting Oncology real-World evidence (GROW)Ann Oncol Castelo-Branco L Pellat A Martins-Branco D 109711123420233784816010.1016/j.annonc.2023.10.001 · doi ↗ · pubmed ↗
- 4Ministerio de Salud y Protección Social. Aseguramiento al sistema general de salud 8 2025 20252025 https://minsalud.gov.co/proteccionsocial/Regimensubsidiado/Paginas/aseguramiento-al-sistema-general-salud.aspx?utm_
- 5A population-based study on incidence trends of kidney and renal pelvis cancers in the United States over 2000-2020 Sci Rep Mousavi SE Najafi M Aslani A Fazlollahi A Yekta Z Sadri M Nejadghaderi SA 112941420243876039910.1038/s 41598-024-61748-2PMC 11101446 · doi ↗ · pubmed ↗
- 6Epidemiology of renal cell carcinoma: 2022 update Eur Urol Bukavina L Bensalah K Bray F 5295428220223610048310.1016/j.eururo.2022.08.019 · doi ↗ · pubmed ↗
- 7Renal cell carcinoma: ESMO clinical practice guideline for diagnosis, treatment and follow-up Ann Oncol Powles T Albiges L Bex A 6927063520243878890010.1016/j.annonc.2024.05.537 · doi ↗ · pubmed ↗
- 8A global trend analysis of kidney cancer incidence and mortality and their associations with smoking, alcohol consumption, and metabolic syndrome Eur Urol Focus Huang J Leung DK Chan EO 200209820223349513310.1016/j.euf.2020.12.020 · doi ↗ · pubmed ↗