Unmasking Parasitic Colitis Mimicking Inflammatory Bowel Disease
Ethan Shamsian, Kranthi K Mandava, Joshua E Pagán-Busigó, Michael Bebawy, Ahmed Al-Khazraji

TL;DR
A rare case of parasitic infections mimicking inflammatory bowel disease and liver cirrhosis highlights the need for careful diagnosis in endemic regions.
Contribution
Highlights the diagnostic challenge of parasitic colitis mimicking IBD and AIH-related cirrhosis.
Findings
A patient with autoimmune hepatitis-related cirrhosis was found to have co-infections with Schistosoma mansoni and Strongyloides stercoralis.
Antiparasitic therapy led to significant clinical improvement, suggesting the parasites contributed to hepatic fibrosis.
The case emphasizes the importance of migration history and freshwater exposure in diagnosing parasitic infections.
Abstract
Parasitic infections may clinically mimic inflammatory bowel disease (IBD), particularly in patients with underlying liver cirrhosis, creating substantial diagnostic uncertainty. We describe a 27-year-old Egyptian male with presumed autoimmune hepatitis (AIH)-related cirrhosis who presented with abdominal pain and bloody diarrhea. Endoscopic evaluation suggested IBD; however, histopathology demonstrated eosinophilic colitis. Subsequent stool and serologic testing confirmed co-infection with Schistosoma mansoni and Strongyloides stercoralis. Treatment with antiparasitic therapy resulted in marked clinical improvement. This rare case of dual parasitic infection underscores the importance of detailed migration and residence history in endemic regions and freshwater exposure history, as these parasites can cause presinusoidal portal hypertension and progressive hepatic fibrosis. Parasitic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
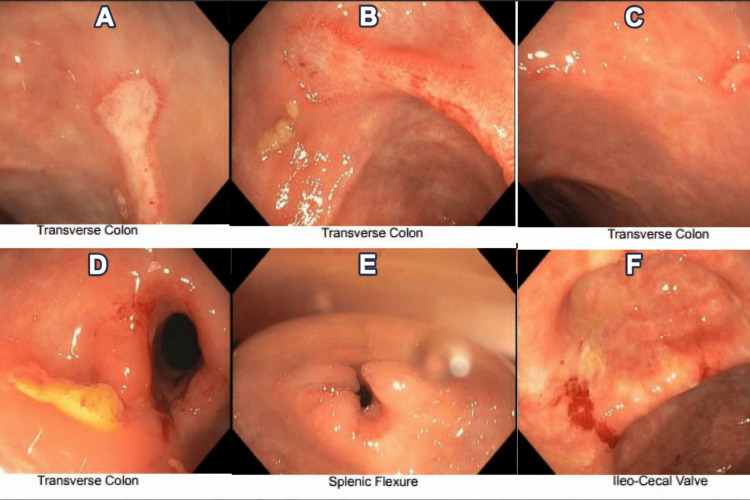 Figure 1
Figure 1| Laboratory Test | Patient Value | Reference Range |
| Hemoglobin (g/dL) | 9.9 | 13.5-17.5 |
| Mean Corpuscular Volume (fL) | 68.5 | 80-100 |
| Serum Iron (µg/dL) | 12 | 60-170 |
| Ferritin (ng/mL) | 12 | 30-400 |
| Alanine Aminotransferase (U/L) | 61 | 7-56 |
| Aspartate Aminotransferase (U/L) | 80 | 10-40 |
| Alkaline Phosphatase (U/L) | 376 | 44-147 |
| Albumin (g/dL) | 2.4 | 3.5-5.0 |
| Peripheral Eosinophils | Normal | 0-500 cells/µL |
| Immunoglobulin G (mg/dL) | >3000 | 700-1600 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Liver Diseases and Immunity · Eosinophilic Esophagitis
Introduction
Patients with liver cirrhosis frequently develop cirrhosis-associated immune dysfunction, a state of immune dysregulation that increases susceptibility to bacterial, viral, and parasitic infections [1]. Parasitic infections such as schistosomiasis and strongyloidiasis may clinically resemble inflammatory bowel disease (IBD), often creating significant diagnostic and therapeutic challenges [2-7]. Additionally, schistosomiasis itself can cause hypergammaglobulinemia and autoantibody positivity, which may confound diagnostic testing and contribute to the misdiagnosis of autoimmune hepatitis (AIH) in cirrhotic patients. Importantly, cirrhosis-associated immune dysfunction and portal hypertension may also blunt peripheral eosinophilic responses through splenic sequestration, immune exhaustion, and altered cytokine signaling, further obscuring the diagnosis of parasitic disease.
Hepatic schistosomiasis is characterized by granulomatous inflammation surrounding schistosome eggs within the portal venous system, leading to elevated presinusoidal portal pressure and portal hypertension in the absence of established cirrhosis. Persistent inflammation may ultimately progress to periportal fibrosis and the development of true cirrhosis. In patients with pre-existing liver disease, superimposed parasitic infection can further exacerbate hepatic dysfunction and precipitate clinical decompensation [8].
We report a case of poly-parasitic infection in a male patient with presumed AIH-related cirrhosis whose clinical presentation mimicked IBD and was complicated by progressive cirrhotic decompensation.
Case presentation
A 27-year-old male originally from Egypt with a history of liver cirrhosis presumed secondary to AIH presented with several days of persistent abdominal pain and bloody diarrhea. He reported being diagnosed with AIH in 2016 after testing positive for antinuclear antibody (ANA) and anti-smooth muscle antibody (ASMA) with an immunoglobulin G (IgG) level >3,000 mg/dL; specific ANA and ASMA titers were not available for review. A liver biopsy performed in 2016 demonstrated grade 4 severe widespread interface hepatitis with grade II focal hepatocellular necrosis and stage I portal fibrosis, supporting the diagnosis of AIH at that time; no schistosome ova or pipestem fibrosis were identified. He was subsequently diagnosed with cirrhosis in 2022 in Egypt after developing ascites, hemorrhoids, abdominal pain, and gastrointestinal bleeding.
On admission, laboratory evaluation demonstrated elevated liver enzymes, hypoalbuminemia, and iron-deficiency microcytic anemia (Table 1). Peripheral eosinophil count was within normal limits.
Esophagogastroduodenoscopy (EGD) demonstrated grade I esophageal varices without stigmata of active bleeding. Colonoscopy revealed moderate strictures in the mid and distal transverse colon, multiple ulcerations within the mid-transverse colon, including within a stricture, and friable mucosa with contact bleeding extending from the transverse colon to the cecum (Figure 1).
Colonoscopy findings in a 27-year-old cirrhotic male with parasitic colitis mimicking IBDColonoscopy images showing large ulcerations within strictures in the mid-to-distal transverse colon (A-D), a stricture at the splenic flexure (E), and a friable ileocecal valve (F).IBD, inflammatory bowel disease
Given the presence of skip lesions, colonic strictures, and a reported history of oral ulceration, IBD was initially considered. Targeted biopsies were obtained, and serum and stool studies were performed to evaluate alternative infectious and inflammatory etiologies, including a viral hepatitis panel, Epstein-Barr virus serologies, cytomegalovirus testing, and stool PCR for common enteric pathogens. All of these studies were negative, making common bacterial and viral causes of colitis less likely and prompting further evaluation for parasitic infection. Histopathology demonstrated chronic active eosinophilic colitis with crypt architectural distortion and marked eosinophilic infiltration of up to 80 eosinophils per high-power field; however, no ova or parasites were visualized in the colonic biopsy specimens. Inflammatory markers, QuantiFERON-Gold testing, and human leukocyte antigen B27 (HLA-B27) were all negative, lowering suspicion for IBD and spondyloarthropathy-associated colitis.
Given the patient’s childhood exposure to freshwater lakes in schistosomiasis-endemic regions of Egypt, additional parasitic evaluation was pursued, including stool ova and parasite examination and Strongyloides serology, which confirmed infection with Schistosoma mansoni and Strongyloides stercoralis. He was treated with praziquantel and albendazole, with adjunctive corticosteroids administered after initiation of antiparasitic therapy to control severe eosinophilic colitis and inflammatory symptoms, resulting in significant clinical improvement. He was scheduled for repeat EGD with endoscopic ultrasound (EUS) and colonoscopy with biopsy to monitor treatment response.
Discussion
This case describes a 27-year-old Egyptian male with presumed AIH-related cirrhosis who presented with abdominal pain and bloody diarrhea. Colonoscopy revealed friable mucosa with moderate stricturing and segmental ulceration, initially raising concern for IBD. However, histopathology demonstrated marked eosinophilic infiltration, and stool and serologic testing confirmed dual infection with S. stercoralis and S. mansoni. These findings prompted reconsideration of the underlying etiology of his chronic liver disease. Although AIH was initially believed to be the primary cause of cirrhosis, the identification of schistosomiasis, together with the known association of chronic schistosomiasis with hypergammaglobulinemia and autoantibody positivity, raises the possibility that his liver disease was at least partially driven by schistosomiasis and may have been misclassified as autoimmune. While the 2016 liver biopsy demonstrated interface hepatitis consistent with AIH, the later recognition of endemic exposure and dual parasitic infection supports reappraisal of the original diagnostic attribution and suggests that schistosomiasis may have contributed significantly to portal hypertension and hepatic fibrogenesis.
This dual parasitic infection is exceedingly rare and, to our knowledge, represents the first reported case in which co-infection with S. stercoralis and S. mansoni produced significant colonic strictures and ulcerations mimicking IBD in the setting of portal hypertension and cirrhosis. The overlapping gastrointestinal manifestations created a substantial diagnostic challenge, particularly in the presence of advanced liver disease. Notably, the absence of peripheral eosinophilia may have delayed diagnosis, as eosinophilic responses are often blunted in patients with cirrhosis or immunosuppression [9].
Parasitic infections are well-recognized mimickers of chronic gastrointestinal disorders. Several features may help distinguish parasitic colitis from idiopathic IBD. Parasitic infections often demonstrate patchy or segmental involvement with relative rectal sparing, marked eosinophilic infiltration on histology, and submucosal granulomas centered on ova or larvae, whereas IBD more typically shows crypt architectural distortion, basal plasmacytosis, and continuous mucosal inflammation in ulcerative colitis or transmural lymphoid aggregates in Crohn’s disease [10]. Strongyloidiasis has been mistaken for IBD or carcinoid syndrome, amebiasis for colorectal malignancy or Crohn’s disease, and schistosomiasis for IBD or cryptogenic cirrhosis [2-7]. These diagnostic pitfalls are especially relevant in cirrhotic patients, whose susceptibility to infection is heightened by cirrhosis-associated immune dysfunction, including impaired reticuloendothelial clearance, decreased hepatic protein synthesis, and dysfunction of gut-associated lymphoid tissue [11,12].
Among parasitic pathogens, Schistosoma species play a particularly well-established role in hepatic fibrogenesis. In hepatosplenic schistosomiasis, chronic immune activation in response to egg deposition promotes granuloma formation and periportal fibrosis. Even before established cirrhosis, egg-mediated inflammation increases presinusoidal resistance, leading to early portal hypertension. Continued egg deposition stimulates a Th2-dominant immune response with production of interleukin (IL)-33 and IL-4, activation of M2 macrophages and hepatic stellate cells, and downstream profibrotic signaling through mediators such as IL-13, transforming growth factor beta-1 (TGF-β1), and vascular endothelial growth factor (VEGF) [8]. This cascade results in progressive collagen deposition and architectural distortion, eventually culminating in cirrhosis and increased risk of hepatocellular carcinoma. Additional profibrotic mechanisms, including microRNA dysregulation and damage-associated molecular patterns, may further amplify liver injury [8]. In this patient, schistosomiasis likely accelerated fibrosis in conjunction with AIH, contributing to early portal hypertension and cirrhosis.
Simultaneous infection with multiple parasites is exceptionally uncommon. Bhattacharyya et al. reported a 50-year-old Yemeni man with chronic gastrointestinal and respiratory symptoms who was ultimately found to have Entamoeba histolytica, S. mansoni, Fasciola hepatica, and S. stercoralis infections [13]. That diagnosis required repeated testing in the setting of eosinophilia and hepatosplenomegaly. In contrast, our patient lacked dermatologic or pulmonary manifestations of strongyloidiasis, suggesting that cirrhosis-associated immune dysfunction may have facilitated parasitic persistence or reactivation. His childhood exposure to freshwater sources in an endemic region and prior diarrheal illness further support the possibility of latent infection reactivating with immune compromise.
Importantly, in patients with suspected or confirmed S. stercoralis infection, corticosteroid therapy poses a unique and well-documented risk of precipitating hyperinfection syndrome, a potentially fatal complication characterized by uncontrolled autoinfection, disseminated larvae, and secondary gram-negative sepsis [14]. For this reason, antiparasitic therapy with ivermectin or albendazole must be initiated before or concomitantly with corticosteroids when immunosuppression is clinically necessary. In the present case, corticosteroids were administered only after antiparasitic coverage was established, specifically to manage severe eosinophilic colitis and inflammatory symptoms, thereby mitigating the risk of Strongyloides hyperinfection while allowing symptomatic control.
Finally, this case mirrors observations from endemic regions where patients presenting with IBD-like symptoms were ultimately diagnosed with parasitic colitis on histopathologic evaluation [15,16]. These reports emphasize the importance of a detailed travel and environmental exposure history and highlight that negative stool studies do not exclude invasive parasitic disease. In patients from endemic areas, parasitic infection should remain a critical consideration before initiating immunosuppressive therapy.
Conclusions
This case underscores the critical importance of considering parasitic infections in the differential diagnosis of IBD-like presentations, particularly in patients with chronic liver disease originating from endemic regions. Dual infection with S. mansoni and S. stercoralis can produce severe colonic inflammation, stricturing disease, and progressive hepatic fibrosis, closely mimicking autoimmune and inflammatory etiologies. Failure to recognize these infections may lead to inappropriate initiation of immunosuppressive therapy without adequate antiparasitic coverage, with potentially life-threatening consequences.
In the era of global migration, we recommend that patients from schistosomiasis- or strongyloidiasis-endemic regions who are labeled with AIH, cryptogenic cirrhosis, or IBD-like colitis undergo targeted parasitic screening. This is particularly critical prior to initiating or escalating immunosuppressive therapy. A careful exposure history combined with early parasitic testing should be incorporated into diagnostic algorithms in non-endemic, high-resource settings to avoid diagnostic delay, guide appropriate therapy, and prevent irreversible liver injury or Strongyloides hyperinfection syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liver cirrhosis and immune dysfunction Int Immunol Hasa E Hartmann P Schnabl B 4554663420223579276110.1093/intimm/dxac 030PMC 9447994 · doi ↗ · pubmed ↗
- 2Jejunal strongyloidiasis mimicking crohn's colitis: a diagnostic dilemma!Indian J Pathol Microbiol Goyal S Barman S Sakhuja P Sachdeva S Narang P Nag HH 1611646820253876981810.4103/ijpm.ijpm_298_23 · doi ↗ · pubmed ↗
- 3Strongyloidiasis mimicking carcinoid syndrome in an immunocompetent host Cureus Latta S Kasti K Almuinas de Armas S Krishnaswamy S Reyes-Corcho A 015202310.7759/cureus.48608 PMC 1071133938090419 · doi ↗ · pubmed ↗
- 4Entamoeba histolytica-associated proctitis and ileitis mimicking Crohn's disease—a case report Clin Case Rep Griemert T Siegel E Brandstetter M Straub BK Kreft A Galle PR Sprinzl MF 011202310.1002/ccr 3.6833 PMC 1019980837220511 · doi ↗ · pubmed ↗
- 5Caecal amoebic colitis mimicking a colorectal cancer J Surg Case Rep Sinharay R Atkin G Mohamid W Reay-Jones N 12011201110.1093/jscr/2011.11.1PMC 364933024972391 · doi ↗ · pubmed ↗
- 6Amebic colitis Stat Pearls Taherian M Samankan S Cagir B Treasure Island, FL Stat Pearls Publishing 42025 https://pubmed.ncbi.nlm.nih.gov/31194394/31194394 · pubmed ↗
- 7Human schistosomiasis Lancet Gryseels B Polman K Clerinx J Kestens L 1106111836820061699766510.1016/S 0140-6736(06)69440-3 · doi ↗ · pubmed ↗
- 8Host regulators of liver fibrosis during human schistosomiasis Front Immunol Kamdem SD Moyou-Somo R Brombacher F Nono JK 2781920183054636410.3389/fimmu.2018.02781 PMC 6279936 · doi ↗ · pubmed ↗