Risk factors for progression from Clostridioides difficile colonization (NAAT+/toxin–) to infection (toxin+) following symptomatic retesting
Sophia Chang, Nicholas Turner, Michael Yarrington, Deverick Anderson

TL;DR
This study identifies risk factors for Clostridioides difficile infection progression from colonization in patients, highlighting the role of antibiotic use.
Contribution
The study reveals that sustained high-risk antibiotic use is a strong predictor of progression from colonization to infection.
Findings
High-risk antibiotic use was associated with a 2.70-fold increased odds of progressing to CDI.
Sustained antibiotic exposure is a significant risk factor for CDI progression.
Host and clinical factors were identified as predictors of infection development.
Abstract
To identify host and clinical risk factors contributing to the development of Clostridioides difficile infection (CDI) among colonized patients. Retrospective, matched case-control study. Duke University Health System, including 3 hospitals and affiliated outpatient clinics. Adult patients who underwent ≥2 two-step C. difficile tests (nucleic acid amplification test (NAAT) followed by toxin enzyme immunoassay) between 03/15/2020–12/31/2023. Cases were patients with C. difficile colonization (NAAT+/toxin–) who converted to CDI (NAAT+/toxin+) within 90 days; controls were colonized patients who remained toxin-negative. Cases were matched to controls by date of index testing (±1 year). Data collection encompassed a 90-day “pre-exposure” period preceding index testing and a ≤ 90-day “exposure” period between index and repeat testing. Antibiotic use was stratified by risk for each…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
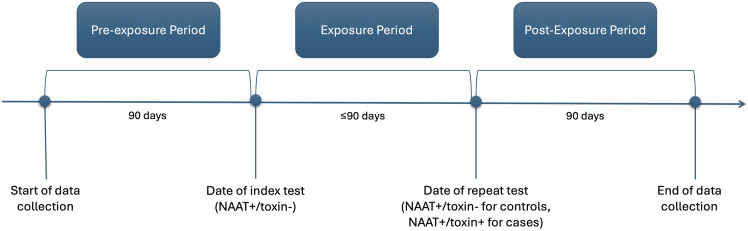 Figure 1
Figure 1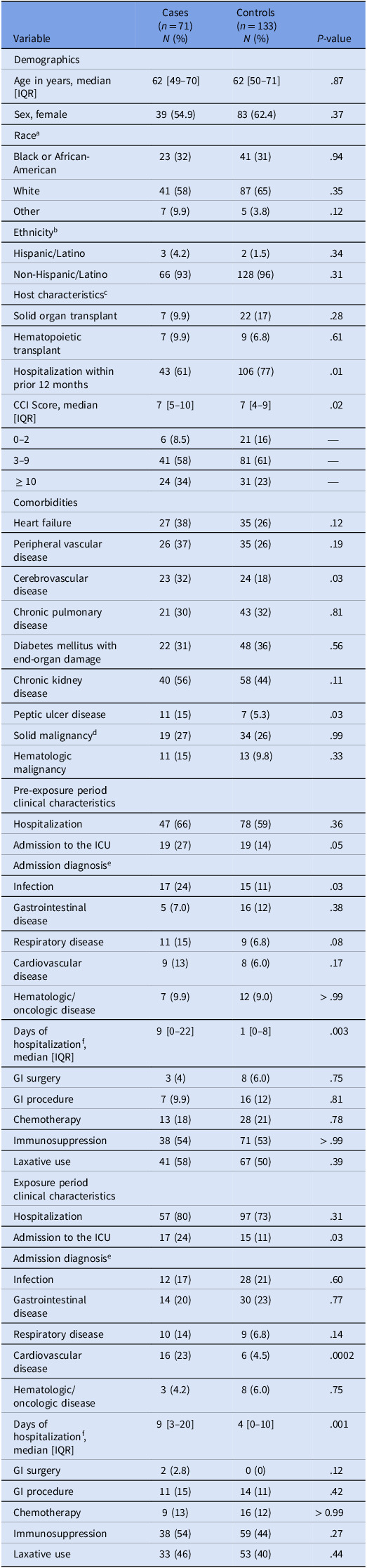 Figure 2
Figure 2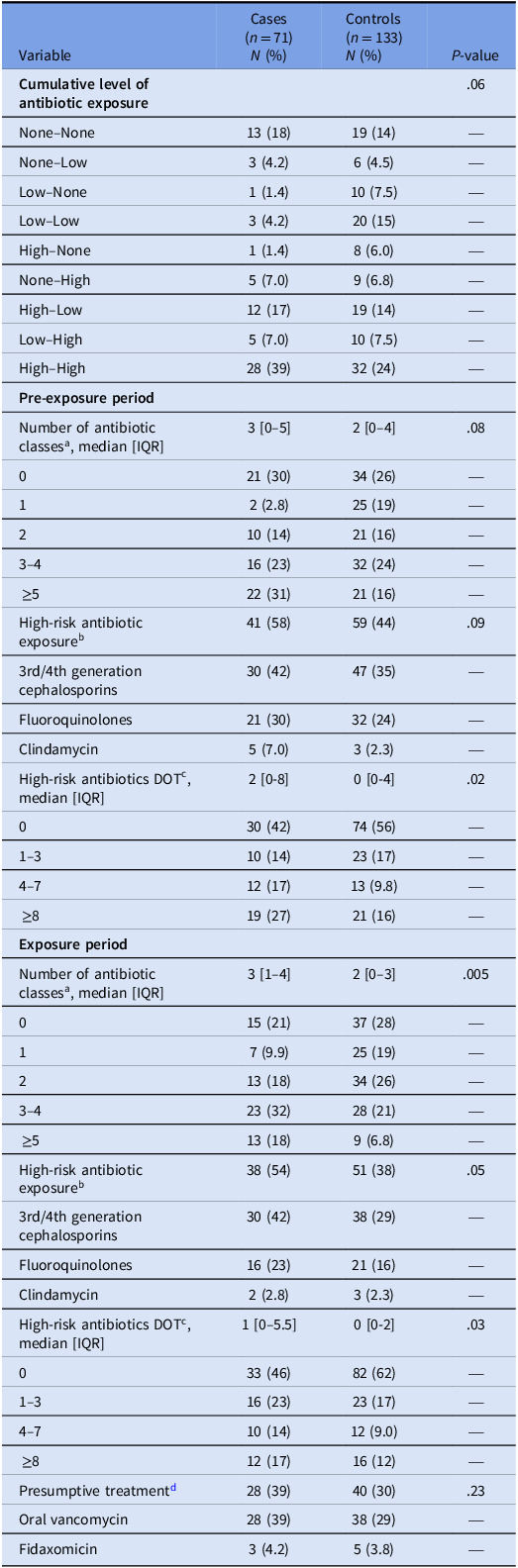 Figure 3
Figure 3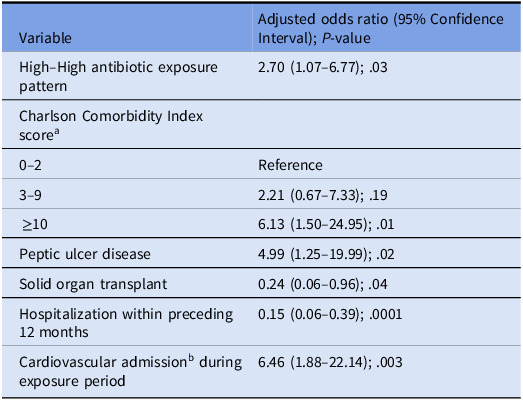 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Antibiotic Use and Resistance · Antimicrobial Resistance in Staphylococcus
Introduction
Clostridioides difficile infection (CDI) is the leading cause of healthcare-associated diarrhea and the most common cause of healthcare-associated infection.^1,2^ Antibiotic exposure is an established risk factor for the development of CDI. Other risk factors for CDI include older age, chemotherapy, gastrointestinal surgery, frequent healthcare exposures, and comorbidities such as cardiac disease, chronic kidney disease, and solid organ transplantation (SOT).^3–5^
Importantly, the presence of C. difficile in the intestine does not necessitate disease. C. difficile colonization is defined by C. difficile detection in stool in the absence of clinical symptoms. Previous studies have demonstrated colonization rates ranging from 4% to 15% among healthy individuals, 3% to 21% among hospitalized patients, and 4% to 51% among long-term care facility residents.^6^ Colonization was initially thought to confer protection against symptomatic C. difficile; however, more recent research has indicated that it may increase the risk of CDI.^6–8^ A meta-analysis of 19 studies published in 2015 found that patients colonized with toxigenic C. difficile on admission had a relative risk of 5.86 (95% confidence interval [CI], 4.21–8.16) of developing CDI compared to non-colonized patients.^9^
A 2025 study by our group expanded on these results. Using data collected between 2020–2023, Turner et al. found that C. difficile colonization was associated with progression to CDI (adjusted hazard ratio [aHR], 5.06 [95% CI, 3.61–7.10]), particularly in the setting of high-risk antibiotic receipt (aHR, 15.71 [95% CI, 9.85–25.06]). Despite this association, the absolute rate of progression remained relatively low at 5% (95% CI, 4%–6%).^10^
Thus, among individuals colonized with C. difficile, only a subset progress to disease.^9,10^ The factors that determine why some convert while others remain asymptomatic are not well understood. Many studies have examined risk factors for CDI in general patient populations, but relatively few have focused specifically on patients with known colonization who develop active infection. The objective of this study was to identify host and clinical risk factors associated with the progression from C. difficile colonization to infection.
Methods
Study design and patient population
This retrospective, matched case-control study was conducted in the 3 hospitals and affiliated outpatient clinics within Duke University Health System (DUHS). Patients were evaluated for inclusion if they underwent ≥2 two-step stool tests for C. difficile between 15 March 2020 and 31 December 2023. The two-step algorithm consisted of a nucleic acid amplification test (NAAT; Cepheid Xpert) with reflex to toxin enzyme-linked immunosorbent assay (TechLab Quik Chek Complete) when NAAT positive. Testing was restricted to unformed stool specimens. Reports with a NAAT+/toxin–result included the comment: “Likely represents colonization with alternative cause of symptoms. Treatment generally not indicated unless clinical signs of severe or fulminant C. difficile disease. Consider Infectious Disease consult in questionable cases.”
C. difficile colonization was defined as the detection of C. difficile in the absence of toxin (NAAT+/toxin−), while infection was defined as the simultaneous detection of pathogen and toxin (NAAT+/toxin+). NAAT– subjects were excluded.^4,6,11^ The index test was defined as an initial NAAT+/toxin− result indicating C. difficile colonization. Cases were patients with colonization on index testing who progressed to infection within 90 days, as evidenced by a repeat test yielding a NAAT+/toxin+ result. Controls were colonized patients who did not progress to infection and remained toxin-negative on all subsequent testing within the same follow-up window. Patients were excluded if their index toxin-negative test was preceded by a toxin-positive result in the 90 days prior. For cases with >1 toxin-positive assay within the 90-day follow-up window, the test closest in time to the index was selected for inclusion. Cases were matched to controls at a minimum ratio of 1:1 and maximum ratio of 1:3 based on date of index testing (±1 year). Study subjects were identified via the Duke Enterprise Data Unified Content Explorer (DEDUCE) database.^12^ DUHS institutional review board reviewed the study design and determined it to be exempt with a waiver of consent for data collection.
Definitions and data collection
To temporally distinguish risk factors influencing the progression from C. difficile colonization to infection, data collection for each patient was divided into three predefined intervals (Figure 1): a “pre-exposure” period, defined as the 90 days preceding the index colonization test; an “exposure” period, defined as the ≤90-day interval between the index test and the outcome event—the development of CDI for cases or the end of follow-up for controls; and a “post-exposure” period, defined as the 90 days following repeat testing.
Figure 1.Temporal segmentation of patient data for assessing progression from C. difficile colonization to infection. NAAT, nucleic acid amplification test **(**Figure in accompanying digital file per submission guidelines).
All data were obtained through the DUHS electronic health record and DEDUCE database. For each patient, data were collected on demographics, outcomes, comorbidities (identified via International Classification of Diseases, Tenth Revision codes), recent healthcare exposures, and inpatient and outpatient antibiotic administrations. For systemic antibiotics, the class and duration of therapy were recorded. Admission details were collected for patients who were hospitalized at any time during the pre-exposure, exposure, and/or post-exposure periods. Outcomes studied included evidence of fulminant disease among cases, readmission in the post-exposure period, and death 1 year from the date of index testing.
Antibiotic exposure classification
Given the central role antibiotics play in the pathogenesis of CDI, we applied a structured approach to represent patients’ time-varying antibiotic exposure profiles. Each systemic antibiotic administered to a patient was assigned a risk level. High-risk antibiotics were defined as clindamycin, fluoroquinolones, and third- or fourth-generation cephalosporins,^13^ while all other antibiotics were classified as low-risk. Each patient was then assigned a categorical exposure level for the pre-exposure period and the exposure period: no antibiotic exposure (“None”), only low-risk antibiotic exposure (“Low”), or any high-risk antibiotic exposure (“High”). From these two dimensions—risk level and timing—we classified patients’ cumulative antibiotic exposure profiles into nine mutually exclusive patterns: “None–None,” “None–Low,” “Low–None,” “Low–Low,” “High–None,” “None–High,” “High–Low,” “Low–High,” and “High–High.”
Data analysis
Categorical variables were reported as frequencies and percentages and compared between cases and controls using Pearson’s chi-square test or Fisher’s exact test, as appropriate. Continuous variables were reported as medians with interquartile ranges (IQRs) and compared using the Wilcoxon rank-sum test. All pre-exposure and exposure period variables with a bivariate P-value ≤ .2 were evaluated for inclusion in multivariate modeling.
We utilized multivariate conditional logistic regression modeling to identify factors independently associated with the progression from C. difficile colonization to CDI. Covariates were selected for inclusion using a stepwise forward selection approach, with retention based on statistical significance (P ≤ .05) and adherence to event-per-parameter guidelines.^14^
Other antibiotic-related variables—such as number of antibiotic classes, duration of antibiotic therapy, and use of specific antibiotic classes—were excluded from the final models due to high collinearity with the variables characterizing patients’ cumulative antibiotic exposure profiles. Sensitivity analyses were conducted to ensure that their exclusion did not meaningfully alter the associations of interest.
Statistical analyses were performed using R, version 4.2.1
Results
Cohort characteristics
Among 2,212 patients with C. difficile colonization identified during the study period, 71 cases and 133 matched controls met criteria for inclusion. The cohort was 60% female with a median age of 62 [50–71] years. Most of the patients identified as White (63%), followed by Black (31%), with 6% identifying as another race. Demographics of case and control patients were generally similar (Table 1). The median time from index to repeat testing was 28 [17–51] days. Most patients underwent both index and repeat testing in an inpatient setting (66% and 65% respectively). Repeat testing in an inpatient setting was significantly more common among cases than controls (79% vs 57%; P = .003), while outpatient repeat testing was significantly less frequent in cases (18% vs 33%; P = .04).
Table 1.Host and clinical characteristics across pre-exposure and exposure periodsVariableCases(n = 71) N (%)Controls(n = 133) N (%) P-valueDemographicsAge in years, median [IQR]62 [49–70]62 [50–71].87Sex, female39 (54.9)83 (62.4).37Race^a^ Black or African-American23 (32)41 (31).94White41 (58)87 (65).35Other7 (9.9)5 (3.8).12Ethnicity^b^ Hispanic/Latino3 (4.2)2 (1.5).34Non-Hispanic/Latino66 (93)128 (96).31Host characteristics^c^ Solid organ transplant7 (9.9)22 (17).28Hematopoietic transplant7 (9.9)9 (6.8).61Hospitalization within prior 12 months43 (61)106 (77).01CCI Score, median [IQR]7 [5–10]7 [4–9].020–26 (8.5)21 (16)—3–941 (58)81 (61)— ≥ 1024 (34)31 (23)—ComorbiditiesHeart failure27 (38)35 (26).12Peripheral vascular disease26 (37)35 (26).19Cerebrovascular disease23 (32)24 (18).03Chronic pulmonary disease21 (30)43 (32).81Diabetes mellitus with end-organ damage22 (31)48 (36).56Chronic kidney disease40 (56)58 (44).11Peptic ulcer disease11 (15)7 (5.3).03Solid malignancy^d^ 19 (27)34 (26).99Hematologic malignancy11 (15)13 (9.8).33Pre-exposure period clinical characteristicsHospitalization47 (66)78 (59).36Admission to the ICU19 (27)19 (14).05Admission diagnosis^e^ Infection17 (24)15 (11).03Gastrointestinal disease5 (7.0)16 (12).38Respiratory disease11 (15)9 (6.8).08Cardiovascular disease9 (13)8 (6.0).17Hematologic/oncologic disease7 (9.9)12 (9.0) > .99Days of hospitalization^f^, median [IQR]9 [0–22]1 [0–8].003GI surgery3 (4)8 (6.0).75GI procedure7 (9.9)16 (12).81Chemotherapy13 (18)28 (21).78Immunosuppression38 (54)71 (53) > .99Laxative use41 (58)67 (50).39Exposure period clinical characteristicsHospitalization57 (80)97 (73).31Admission to the ICU17 (24)15 (11).03Admission diagnosis^e^ Infection12 (17)28 (21).60Gastrointestinal disease14 (20)30 (23).77Respiratory disease10 (14)9 (6.8).14Cardiovascular disease16 (23)6 (4.5).0002Hematologic/oncologic disease3 (4.2)8 (6.0).75Days of hospitalization^f^, median [IQR]9 [3–20]4 [0–10].001GI surgery2 (2.8)0 (0).12GI procedure11 (15)14 (11).42Chemotherapy9 (13)16 (12) > 0.99Immunosuppression38 (54)59 (44).27Laxative use33 (46)53 (40).44IQR, interquartile range; CCI, Charlson Comorbidity Index; ICU, intensive care unit; GI, gastrointestinal. ^a^For cases, other race includes Asian (n = 2) and unknown (n = 5). For controls, other race includes American Indian/Alaska Native (n = 1), Asian (n = 3), and unknown (n = 1). ^b^Data were excluded for 2 cases and 3 controls where ethnicity was unknown. ^c^At time of index testing. ^d^Includes non-metastatic and metastatic disease. ^e^Admission diagnoses were not mutually exclusive; patients could be classified into more than 1 category. Additional admission diagnoses not shown in the table include renal disease, neurological disease, metabolic disorders, and miscellaneous. ^f^Includes subjects who were not hospitalized (0 days).
Antibiotic characteristics
During the pre-exposure period, patients were prescribed a median of 2 [0–4] antibiotic classes, with nearly half (n = 100, 49%) receiving at least one high-risk antibiotic (Table 2). During the exposure period, patients were prescribed a median of 2 [0–3] antibiotic classes, with 89 (44%) patients receiving at least one high-risk antibiotic. In contrast, 55 (27%) patients in the pre-exposure period and 52 (25%) patients in the exposure period had no antibiotic exposure. Cases were more likely to receive high-risk antibiotics across both periods (High–High) compared to controls (P = .02).
Table 2.Antibiotic characteristics across pre-exposure and exposure periodsVariableCases(n = 71) N (%)Controls(n = 133) N (%) P-value Cumulative level of antibiotic exposure .06None–None13 (18)19 (14)—None–Low3 (4.2)6 (4.5)—Low–None1 (1.4)10 (7.5)—Low–Low3 (4.2)20 (15)—High–None1 (1.4)8 (6.0)—None–High5 (7.0)9 (6.8)—High–Low12 (17)19 (14)—Low–High5 (7.0)10 (7.5)—High–High28 (39)32 (24)— Pre-exposure period Number of antibiotic classes^a^, median [IQR]3 [0–5]2 [0–4].08021 (30)34 (26)—12 (2.8)25 (19)—210 (14)21 (16)—3–416 (23)32 (24)— ≥522 (31)21 (16)—High-risk antibiotic exposure^b^ 41 (58)59 (44).093rd/4th generation cephalosporins30 (42)47 (35)—Fluoroquinolones21 (30)32 (24)—Clindamycin5 (7.0)3 (2.3)—High-risk antibiotics DOT^c^, median [IQR]2 [0-8]0 [0-4].02030 (42)74 (56)—1–310 (14)23 (17)—4–712 (17)13 (9.8)— ≥819 (27)21 (16)— Exposure period Number of antibiotic classes^a^, median [IQR]3 [1–4]2 [0–3].005015 (21)37 (28)—17 (9.9)25 (19)—213 (18)34 (26)—3–423 (32)28 (21)— ≥513 (18)9 (6.8)—High-risk antibiotic exposure^b^ 38 (54)51 (38).053rd/4th generation cephalosporins30 (42)38 (29)—Fluoroquinolones16 (23)21 (16)—Clindamycin2 (2.8)3 (2.3)—High-risk antibiotics DOT^c^, median [IQR]1 [0–5.5]0 [0-2].03033 (46)82 (62)—1–316 (23)23 (17)—4–710 (14)12 (9.0)— ≥812 (17)16 (12)—Presumptive treatment^d^ 28 (39)40 (30).23Oral vancomycin28 (39)38 (29)—Fidaxomicin3 (4.2)5 (3.8)—IQR, interquartile range; DOT, duration of therapy. ^a^Antibiotics were divided into the following classes: 3rd/4th generation cephalosporins; fluoroquinolones; clindamycin; aminoglycosides; 1st/2nd/5th generation cephalosporins; macrolides; penicillins; beta-lactamase inhibitor combinations; sulfonamides; carbapenems; IV vancomycin; tetracyclines; metronidazole; and miscellaneous (fosfomycin, nitrofurantoin, methenamine, linezolid, tedizolid, dapsone, daptomycin, isoniazid, rifampin, and rifaximin). ^b^The summed antibiotic count exceeds the number of patients exposed, as some individuals received multiple classes. ^c^Measured in days. Different antibiotic classes administered on the same day were each counted as separate antibiotic days. ^d^Administration of oral vancomycin or fidaxomicin at any time during the exposure period was considered presumptive treatment. The summed antibiotic count exceeds the number of patients treated presumptively, as some individuals received both antibiotics.
Table 3.Multivariate conditional logistic regression model for the progression from C. difficile colonization to infectionVariableAdjusted odds ratio (95% Confidence Interval); P-valueHigh–High antibiotic exposure pattern2.70 (1.07–6.77); .03Charlson Comorbidity Index score^a^ 0–2Reference3–92.21 (0.67–7.33); .19 ≥106.13 (1.50–24.95); .01Peptic ulcer disease4.99 (1.25–19.99); .02Solid organ transplant0.24 (0.06–0.96); .04Hospitalization within preceding 12 months0.15 (0.06–0.39); .0001Cardiovascular admission^b^ during exposure period6.46 (1.88–22.14); .003 ^a^At time of index testing. ^b^Identified by searching the admission diagnosis text for any of the following keywords: myocardial, heart, cardiac, cardiomyopathy, cardiovascular, vascular, circulatory, ECMO, or arrhythmia.
Outcomes
In the post-exposure period, readmissions occurred in nearly half of patients (n = 69, 34%) with no significant differences between cases and controls. A total of 62 (87%) cases received treatment, and oral vancomycin was the most frequently administered therapy (n = 58, 82%). A small proportion of cases did not receive therapy, for reasons that were not captured. Evidence of fulminant disease among cases was rare; only 2 cases (3%) required rectal vancomycin, and 1 case (1%) underwent a colectomy. Mortality at 1 year was similar between cases and controls at 26.76% and 27.07% respectively.
Risk factors for the progression from C. difficile colonization to infection
In bivariate analyses, several variables differed significantly between cases and controls (Table 1). Cases were more likely to have cerebrovascular disease, peptic ulcer disease (PUD), and a higher baseline Charlson Comorbidity Index (CCI) score.^15^ They were also less likely to have a history of hospitalization in the 12 months preceding colonization. In terms of clinical risk factors, cases experienced higher rates of intensive care unit (ICU) admission, longer hospital stays, and more cardiovascular-related admissions in the exposure period. Cases also received a greater number of antibiotic classes during the exposure period but had longer durations of high-risk antibiotic therapy in both time periods (Table 2). High-risk antibiotic use during the exposure period and across both periods was significantly more common among cases.
In our final multivariate model, high-risk antibiotic use across both the pre-exposure and exposure period was associated with progression to CDI in comparison to all other exposure patterns (adjusted odds ratio (aOR), 2.70 [95% CI, 1.07–6.77]; P = .03). Several non-antibiotic factors were also found to be contributing to or protective against CDI, including a CCI score ≥ 10, PUD, SOT, a cardiovascular-related admission during the exposure period, and a history of hospitalization within 12 months of index testing.
As a sensitivity analysis, an interaction model incorporating pre-exposure and exposure-period antibiotic risk profiles was constructed to assess whether sequential antibiotic use conferred greater risk than isolated use; to account for the temporal sequence of susceptibility; and to distinguish between isolated, sustained, and mixed-risk patterns (Supplementary Data Table 1). Patients who received low-risk followed by high-risk antibiotics (Low–High) demonstrated higher odds of CDI progression (aOR, 134.57; P = .02). Those with sustained high-risk antibiotic use (High–High) exhibited the greatest risk (aOR, 316.63; P = .01). A likelihood ratio test comparing the full interaction model to a nested main-effects-only model with identical covariates revealed that the addition of interaction terms improved model fit (χ^2^ = 11.12 on 4 df, P = .03), though findings were interpreted with caution given model instability and wide confidence intervals.
In an additional sensitivity analysis excluding controls who received presumptive treatment, results were consistent with the primary model (Supplementary Data Table 2). Sustained high-risk antibiotic use across the pre-exposure and exposure periods remained strongly associated with progression from colonization to infection (aOR 6.08, [95% CI, 1.80–20.6]; P = .004). Associations between non-antibiotic covariates were similar in direction and magnitude to those observed in the main analysis, though estimates were imprecise given reduced sample size.
To explore the unexpected protective association of prior hospitalization, we conducted a series of post hoc analyses. One hypothesis was that patients with more prior hospitalizations received more proactive intervention. However, when we analyzed rates of presumptive treatment, we found no meaningful differences across hospitalization strata. Differential treatment patterns alone are therefore unlikely to account for the observed association. We also explored whether patients with prior hospitalizations were less likely to receive high-risk antibiotics as a result of increased monitoring and antibiotic stewardship. Contrary to this hypothesis, patients with a history of recent hospitalization were significantly more likely to receive high-risk antibiotics during both the pre-exposure (χ² = 10.9, df = 1, P = .001) and exposure periods (χ² = 11.15, df = 1, P = .001). Thus, further investigation and validation of this finding is required.
Discussion
Our study provides novel information about potential risk factors for the development of CDI among patients previously identified with C. difficile colonization.^10,16^ Results of our multivariate model and sensitivity analyses revealed a potential dose-dependent trend in which earlier, prolonged, and higher-risk antibiotic exposure conferred progressively greater odds of CDI. These observations suggest that both the timing and class of antibiotic therapy contribute to CDI pathogenesis among colonized patients, with sequential exposure to higher-risk agents likely compounding microbiome disruption and contributing to loss of colonization resistance. These findings also underscore the importance of antibiotic stewardship not only after colonization is identified but also during preceding healthcare encounters, when early antimicrobial decisions may influence downstream infection risk.
In addition, several non-antibiotic factors emerged as independent predictors of progression to CDI. Consistent with prior research, hospitalization during the exposure period for cardiovascular-related conditions was strongly associated with conversion^17,18^; for example, Mamic et al. observed that patients admitted for heart failure had a 13% elevated risk of developing CDI.^17^ This risk may be related to increased systemic inflammation and sympathetic activity, and/or volume depletion and demand mismatch.^18^ This association may also reflect the increased clinical severity and complexity of cardiovascular admissions. Among all hospitalized patients in our cohort, cardiovascular admissions were 3.25-times (95% CI, 1.09–9.40) more likely to involve intensive care compared to non-cardiovascular admissions.
Additional independent predictors of progression in our study included a CCI score ≥ 10 and the presence of PUD at the time of index testing. A higher CCI score likely reflects greater systemic vulnerability due to disease burden and treatment, which may lower the threshold for colonization to transform into clinically significant infection.^19,20^ PUD may contribute further risk by compromising mucosal integrity, though its specific role in CDI pathogenesis warrants further investigation.^21^ Interestingly, in contrast to most existing literature, SOT was independently associated with a lower risk of progression in our study. The number of SOT recipients in our cohort was relatively small (n = 29, 14%), and the observed association may reflect unmeasured confounding, limited power, or center-specific practices. A 2020 retrospective cohort study reported relatively low rates of progression from colonization to infection in SOT cohorts, possibly reflecting early intervention and aggressive infection prevention protocols.^22^ While these findings offer a plausible explanation for our observed association, they are exceptions rather than the norm in the literature. Further investigation is needed to clarify whether certain clinical protocols in transplant care may influence risk of progression.
Several risk factors previously linked to CDI were not independent predictors in our cohort. Age, laxatives, chemotherapeutics, and immunosuppressants did not differ significantly between cases and controls.^3–5^ Presumptive treatment was also not associated with a lower risk of subsequent toxin positivity, despite being previously reported as protective in a similar study^16^ and by prior analyses conducted by our group.^10^
Healthcare exposure patterns in our study revealed a complex relationship with CDI risk. Most notably, a history of hospital admission in the preceding 12 months was associated with a strong protective effect in both bivariate and multivariate analyses—contrary to established literature that identifies prior hospitalization as a risk factor.^3–5^ Additionally, residence in skilled nursing facilities and other healthcare settings prior to admission were not significantly different among cases and controls.^4,5^ It is conceivable that these and the preceding patient-level risk factors described above may actually be more associated with colonization (which all included patients had by definition) as opposed to progression from colonization, but further investigation of this hypothesis will be required. Prolonged hospitalization and ICU admission were statistically associated with progression in bivariate analyses, suggesting that certain forms of healthcare utilization remain important risk factors for CDI.
Our study has limitations. While we operationalized NAAT+/toxin– as a proxy for colonization, some of these controls may have had early or partially treated CDI. As testing was limited to patients with unformed stool, the study cohort likely included a mixture of true infection and colonization with alternate causes of diarrhea. This distinction is a known limitation of NAAT-based testing algorithms and of retrospective designs relying on clinical, rather than surveillance, sampling. Further reflecting the diagnostic uncertainty inherent to this group, approximately one-third of controls received CDI-directed therapy. However, the robustness of results in our sensitivity analysis excluding presumptively treated controls suggests that this potential misclassification did not materially affect our conclusions. Additional limitations include data being restricted to encounters, prescriptions, and laboratory testing documented within DUHS. Moreover, while we adjusted for several known risk factors, the possibility of residual confounding from unmeasured or imperfectly measured variables remains. Repeat testing intervals were not standardized, and despite excluding periods >90 days, timing variability may have influenced exposure assessment. We were unable to fully adjust for the severity of acute illness that may influence CDI pathogenesis. Microbiological data such as C. difficile strain type, which could affect virulence, were also not available. Differences in clinician testing practices, care environments, or social determinants of health may have also influenced results in ways not fully captured in our data set. Next, the sample size of our cohort likely limited statistical power and our ability to detect associations for less common exposures or outcomes. Finally, the generalizability of our findings may be limited by the nature of the study setting, study population, and retrospective study design.
This retrospective, matched case-control study highlights the differential roles host factors and clinical characteristics play in the progression to CDI among patients identified with C. difficile colonization. We found that high-risk antibiotic use before and after the identification of colonization significantly influenced disease progression, reinforcing the need for vigilant antimicrobial stewardship across the continuum of care—not only after colonization is detected but also during routine healthcare encounters in at-risk populations. The period following colonization represents a particularly critical window during which avoiding high-risk antibiotics may offer the greatest opportunity for targeted stewardship interventions. Further prospective research is needed to refine risk stratification and identify colonized individuals most likely to benefit from early intervention.
Supporting information
Chang et al. supplementary materialChang et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Magill SS, O’Leary E, Janelle SJ, et al. Changes in prevalence of health care–associated infections in U.S. Hospitals. N Engl J Med 2018;379:1732–1744.30380384 10.1056/NEJ Moa 1801550 PMC 7978499 · doi ↗ · pubmed ↗
- 2Magill SS, Edwards JR, Bamberg W, et al. Multistate point-prevalence survey of health care-associated infections. N Engl J Med 2014;370:1198–1208.24670166 10.1056/NEJ Moa 1306801 PMC 4648343 · doi ↗ · pubmed ↗
- 3Kelly CR, Fischer M, Allegretti JR, et al. ACG clinical guidelines: prevention, diagnosis, and treatment of clostridioides difficile Infections. Am J Gastroenterol 2021;116:1124.34003176 10.14309/ajg.0000000000001278 · doi ↗ · pubmed ↗
- 4Kociolek LK, Gerding DN, Carrico R, et al. Strategies to prevent Clostridioides difficile infections in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol 2023;44:527–549.37042243 10.1017/ice.2023.18PMC 10917144 · doi ↗ · pubmed ↗
- 5Loo VG, Bourgault AM, Poirier L, et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med. 2011;365:1693–1703.22047560 10.1056/NEJ Moa 1012413 · doi ↗ · pubmed ↗
- 6Crobach MJT, Vernon JJ, Loo VG, et al. Understanding Clostridium difficile colonization. Clin Microbiol Rev 2018;31:e 00021–17.10.1128/CMR.00021-17PMC 596768929540433 · doi ↗ · pubmed ↗
- 7Baron S, Ostrowsky B, Nori P, et al. Screening of Clostridioides difficile carriers in an urban academic medical center: understanding implications of disease. Infect Control Hosp Epidemiol. 2020;41:149–153.31822302 10.1017/ice.2019.309PMC 7702293 · doi ↗ · pubmed ↗
- 8Gilboa M, Baharav N, Melzer E, Regev-Yochay G, Yahav D. Screening for asymptomatic Clostridioides difficile carriage among hospitalized patients: a narrative review. Infect Dis Ther. 2023;12:2223–2240.37704801 10.1007/s 40121-023-00856-4PMC 10581986 · doi ↗ · pubmed ↗