Derivation of an updated brief multivariable prediction model to detect panic-related anxiety in emergency department patients with cardiopulmonary complaints
Sharon C. Sung, Felicia J.L. Ang, Arul Earnest, Leslie E.C. Lim, Shreshtha Jolly, Gilaine Ng, A. John Rush, Marcus E.H. Ong

TL;DR
This study created a new model to detect panic-related anxiety in emergency patients with heart or lung symptoms, improving diagnosis and reducing repeat visits.
Contribution
A novel symptom-based prediction model for identifying panic-related anxiety in ED patients with cardiopulmonary complaints.
Findings
The model achieved 88% AUC with a cutoff of ≥3 symptoms.
It correctly classified 82.9% of patients with 78.4% sensitivity and 85.7% specificity.
Implementation could reduce ED revisits and improve patient outcomes.
Abstract
Patients with panic related-anxiety (i.e., panic attacks or panic disorder) frequently present to emergency departments (EDs) with cardiopulmonary complaints but are often undiagnosed, which can lead to recurrent visits and prolonged distress. This study aimed to derive a new symptom-based multivariable diagnostic prediction model to detect panic-related anxiety in ED patients with cardiopulmonary symptoms. We conducted a single-blind prospective derivation study over 15 months in the ED of a major tertiary hospital in Singapore. Patients presenting with symptoms of palpitations, chest pain, dizziness, or difficulty breathing were assessed using the Structured Clinical Interview for DSM Disorders (SCID) to diagnose panic-related anxiety. A stepwise multivariable prediction model was constructed using 13 SCID-defined panic symptoms as predictors, with the diagnosis of panic-related…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
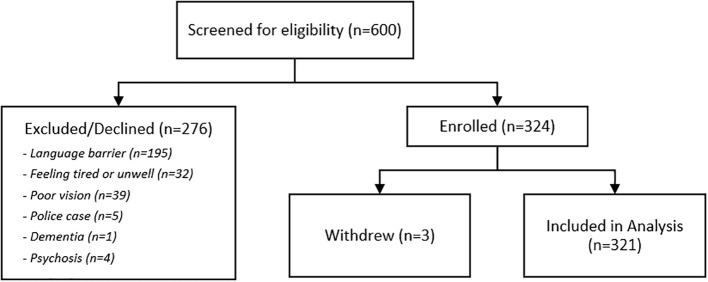 Figure 1
Figure 1| Demographic & Clinical Features | External validation sample n=321 |
|---|---|
| Age in years (mean ± SD) | 52.3 ± 12.4 |
| Gender, n(%) | |
| Male | 221(68.9) |
| Female | 100(31.1) |
| Marital status, n(%) | |
| Single | 43(13.4) |
| Married/living with partner | 249(77.6) |
| Divorced/separated/widowed | 29(9.0) |
| Race/ethnicity, n(%) | |
| Chinese | 197(61.4) |
| Malay | 44(13.7) |
| Indian | 62(19.3) |
| Eurasian | 2(0.6) |
| Other race/ethnicity | 16(5.0) |
| Education, n(%) | |
| Primary or below | 35(10.9) |
| Secondary/Vocational | 155(48.3) |
| Pre-university/Polytechnic | 68(21.2) |
| University/Postgraduate | 63(19.6) |
| Occupational status, n(%) | |
| Managerial/Professional | 82(25.6) |
| Executive/Sales | 35(10.9) |
| Clerical/Technical | 44(13.7) |
| Self-employed | 29(9.03) |
| Retired | 29(9.03) |
| Not working | 17(5.30) |
| Others | 85(26.5) |
| SCID diagnosis, n(%) | |
| Panic attack(s) | 93(29.0) |
| Panic disorder | 32(10.0) |
| Primary discharge diagnosis, n(%) | |
| Chest pain | 282(87.9) |
| Angina or myocardial infarction | 7(2.2) |
| Dizziness and giddiness | 16(5.0) |
| Palpitations | 9(2.8) |
| General symptoms | 3(0.9) |
| Other ICD diagnosis | 3(0.9) |
| Anxiety state* | 3(0.9) |
| ED referral, n(%) | |
| Psychiatry | 2(0.6) |
| Cardiology | 190(59.2) |
| Respiratory medicine | 7(2.2) |
| Gastroenterology | 8(2.5) |
| Internal medicine | 10(3.1) |
| Other specialist outpatient clinic(s) | 8(2.5) |
| Original prediction model | ||||||
|---|---|---|---|---|---|---|
| Panic symptoms: Paresthesia, Derealization or depersonalization, Chills or flushes, Fear of losing control or going crazy, * | ||||||
| Score | Sensitivity | Specificity | Classified Correctly | LR+ | LR- | Youden Index |
| ≥ 1 | 98.40% | 34.70% | 59.50% | 1.5068 | 0.0461 | 33.10% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| ≥ 4 | 36.80% | 93.90% | 71.70% | 6.0107 | 0.6732 | 30.70% |
| ≥ 5 | 22.40% | 98.50% | 68.90% | 14.6347 | 0.7881 | 20.90% |
| ≥ 6 | 6.40% | 99.50% | 63.20% | 12.5441 | 0.9408 | 5.90% |
| ≥ 7 | 0.80% | 100% | 61.30% | -{{-}}- | 0.992 | 0.80% |
- —National Medical Research Council10.13039/501100001349
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnxiety, Depression, Psychometrics, Treatment, Cognitive Processes · Cardiac Health and Mental Health · Music Therapy and Health
Introduction
1
Patients with panic-related anxiety (i.e., panic attacks or panic disorder) use primary healthcare services more frequently than the general population (1, 2) and generate the highest use of emergency department (ED) services among patients with anxiety disorders (3). Even when recognized and treated, panic disorder is often chronic and recurrent, contributing to repeated healthcare use over time. These patients frequently present to the ED with cardiopulmonary complaints such as palpitations, chest pain, dizziness, and shortness of breath, mimicking symptoms of cardiopulmonary emergencies (i.e. myocardial infarction, acute bronchoconstriction) (4). Indeed, panic attacks account for a substantial proportion of ED visits for non-cardiac chest pain, and longitudinal studies show that approximately 70–80% of patients diagnosed with panic disorder in the ED experience recurrent ED visits (5, 6). This symptom overlap often complicates timely diagnosis, leading to repeated ED visits, increased healthcare costs, and poorer long-term outcomes for these patients (1, 2, 7).
Despite high rates of ED presentation among individuals with panic-related anxiety, diagnosis is frequently missed at discharge (6, 8, 9), with many patients left untreated for their underlying anxiety condition. Consequently, there is a need to improve the ability of ED personnel to efficiently identify panic-related anxiety among ED patients. Our team previously developed an initial multivariable prediction model consisting of seven common panic attack symptoms (palpitations, derealization, paresthesia, shortness of breath, chills or hot flushes, dizziness, and fear of losing control or going crazy). This brief interview demonstrated potential in accurately identifying panic-related anxiety in patients with cardiopulmonary complaints, successfully identified panic-related anxiety in a sample of 200 adult ED patients with cardiopulmonary complaints at an accuracy rate of 85% (area under the curve (AUC) = 0.90, sensitivity = 82%, specificity = 88%) (8).
Our objective in the current study is to derive an improved predictive model that would offer more robust diagnostic accuracy in identifying panic-related anxiety among ED patients. By improving screening accuracy, we aim to support ED clinicians in making faster, more accurate diagnoses, thereby reducing the risk of misdiagnosis, decreasing repeat ED visits, and ensuring that patients receive appropriate treatment and follow-up care for anxiety-related conditions.
Materials and methods
2
Study design
2.1
This single-blind, prospective derivation study was conducted over a 15-month period in the ED of a major tertiary care hospital in Singapore. This study followed the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) guidelines for derivation studies.
Study setting
2.2
Participants were recruited between 8:00 a.m. and 6:00 p.m., Monday through Friday, from a high-volume ED serving approximately 200,000 patients annually in Singapore. As an ethnically and linguistically diverse city-state located in Southeast Asia, this setting provided a diverse patient population with varied linguistic and ethnic backgrounds. Singapore has a resident population of 4.04 million, made up of ethically Chinese (74.3%), Malay (13.5%), Indian (9%), and other ethnic groups (3.2%) (10). Over 97% of the population is literate in one (25.7%) or more than one (74.3%) languages. The most common first language spoken by residents is English (48.3%) followed by Mandarin Chinese (29.9%) (10).
Participants
2.3
Eligible participants were English or Mandarin-speaking patients with mild to moderate symptoms on the Patient Acuity Category Scale (11) who were not in danger of acute collapse or in need of resuscitation, aged at least 21 years (the legal age of consent in Singapore), with a chief complaint of palpitations, chest pain, dizziness or difficulty breathing. These symptoms often overlap with both panic-related anxiety and more acute cardiopulmonary conditions, making them critical for the model’s screening utility.
Patients allocated to the most severe triage category were excluded due to the need for acute management. Police cases, patients who were unwilling or unable to complete study procedures, and those who presented with altered mental status, dementia, or psychosis were also excluded.
Procedures
2.4
Upon triage, clinical research coordinators identified potential participants through chief complaints documented in the electronic medical records. Following an initial assessment by the ED physician to ensure clinical stability, coordinators provided study details to patients and obtained written informed consent prior to initiating study procedures. All procedures were approved by the hospital’s Institutional Review Board.
Following consent, participants underwent a structured diagnostic interview to establish the diagnosis of panic disorder and the presence of panic attacks using a modified version of the Panic Disorder Module the Structured Clinical Interview for DSM Disorders (SCID) (12). The SCID is a well-validated semi-structured interview used to diagnose lifetime and current (past month) Axis I psychiatric disorders. For the present study, the SCID was modified to assess all 13 panic attack symptoms. Instead of ending the interview if the participant answered no to the first screening item (“Have you ever had a panic attack, when you suddenly felt frightened, or anxious or suddenly developed a lot of physical symptoms?”), the interviewer proceeded to assess the presence or absence of each of the panic attack symptoms individually. This modification was made to address the fact that ED patients frequently present early in the course of illness with non-fearful panic attacks (13). Hence they may not be aware that their symptoms panic-related when they first present to the ED.
The SCID Panic Disorder module was administered by trained bilingual clinical interviewers fluent in English and Mandarin following a rigorous forward and back translation process, using standardized translated prompts to ensure conceptual consistency across languages. The interviewers administered the SCID and documented each symptom as either present or absent (scored 1 or 0), in addition to coding a diagnosis of panic attack(s), panic disorder, or no panic-related anxiety. All interviewers were blind to the clinical diagnosis provided by the ED physician, which was obtained from the medical record after the SCID diagnostic interview. Inter-rater reliability was high for panic disorder (κ=0.82) and panic attacks (κ=1.00). Weekly consensus meetings were held throughout the study period. Diagnostic uncertainties were adjudicated by the study psychiatrist (LL).
Participants also completed a the Clinical Report Form (CRF) which captured patient-reported demographics, lifetime medical history, frequency of ED visits and hospital admissions in the past year, recent life events in the past year, physician diagnosis for the current ED visit, and discharge disposition.
Sample size determination
2.5
A priori sample size calculations indicated that a total sample size of 310 participants would be sufficient to estimate the area under the curve at 0.85 with a 95% confidence interval within a reasonable width of 0.125, assuming that approximately 20% of participants met criteria for panic-related anxiety.
Model derivation
2.6
The procedures and results to develop the original model are detailed in Sung et al. (8). To derive our updated predictive model, we used the SCID symptom checklist as the primary predictor set, with presence/absence of panic-related anxiety diagnosis (as diagnosed by the SCID) as the outcome variable. We entered all 13 panic attack symptoms into a stepwise multivariable logistic regression with an entry probability of 0.01 and an exit probability of 0.05 to identify symptoms that independently predicted a panic-related anxiety diagnosis.
Performance of updated model
2.7
Model performance was assessed by calculating the area under the receiver operating characteristic (ROC) curve, sensitivity, specificity, positive and negative likelihood ratios, and the Youden index. We used Youden Index for the best balance of sensitivity and specificity. We evaluated various cutoff points for panic symptom counts to identify the optimal threshold for the updated model’s clinical application. All analyses were conducted using Stata, and confidence intervals were calculated for all diagnostic performance metrics.
Results
3
Participants
3.1
We recruited 324 eligible participants for the study (See Figure 1). The most common reason for exclusion was lack of proficiency in the two study languages. Three participants withdrew before completing all study procedures, resulting in a final sample of 321 participants. Full details of sample demographics are shown in Table 1. The mean age was 52.3 years (SD = 12.4), with a higher proportion of males (68.9%) than females. The sample was ethnically diverse, with 61.4% Chinese, 13.7% Malay, 19.3% Indian, and 5.6% representing other ethnic groups. The majority of participants presented with a chief complaint of chest pain (92.2%), followed by dizziness (5.0%) and palpitations (2.8%).
Participant flow diagram.
Using the SCID, 39% (n=125) of participants met diagnostic criteria for panic-related anxiety, either as isolated panic attacks or as part of a panic disorder diagnosis. Among those diagnosed, the most common symptoms reported included shortness of breath, dizziness, and palpitations, which were frequently co-occurring with chest pain. Fewer than 1% of participants received an anxiety-related diagnosis upon ED discharge, and only 0.6% were referred to outpatient psychiatry for follow-up, highlighting the discrepancy between clinical presentation and discharge diagnosis (see Table 1).
Derivation of updated model and performance
3.2
As presented in Table 2, the original model did not perform as well in the external validation sample. When applying the same cutoff score of ≥ 3 in the external validation sample, the original model’s performance declined, with a classification accuracy of 77.9%, reduced sensitivity of 60%, and a Youden index slightly below 50%.
In deriving the updated model, the stepwise logistic regression model identified seven symptoms as significant predictors of panic-related anxiety: shortness of breath, dizziness, palpitations, trembling or shaking, fear of dying, choking, and sweating. When tested at an optimal cutoff score of ≥3 symptoms, the updated model achieved an area under the curve (AUC) of 0.88, with a sensitivity of 78.4% and specificity of 85.7%. The Youden index was 64.1%, indicating good discriminatory ability (Table 2). Positive and negative likelihood ratios were 5.49 and 0.25, respectively, further supporting the model’s utility in distinguishing patients with panic-related anxiety from those without. Shortness of breath, dizziness, and palpitations were significant predictors for panic-related anxiety in both the original and updated models, but the remaining items did not overlap (See Table 2).
Discussion
4
In our initial model development study, the original prediction model showed excellent separation between those with and without panic-related anxiety at a cutoff score of ≥ 3. In this derivation of an updated model, the performance of the original model decreased, possibly due to differences in the patient population of the validation sample. The new model’s AUC and diagnostic performance were superior, validating the updated symptom combination as a more accurate tool for detecting panic-related anxiety in the ED setting. These improved metrics indicate that the updated model has good discrimination and a clinically useful balance between sensitivity and specificity for ED screening, with an optimal cutoff score of ≥ 3. It is well-known that prediction models tend to perform better on data on which the model was constructed than on new data (14). Therefore, our findings underline the importance of ongoing evaluation and refinement of predictive models to maintain their accuracy and generalizability across different settings.
Clinical implications
4.1
Consistent with previous studies (6, 8, 9), nearly 40% of participants in the present study met diagnostic critiera for panic-related anxiety and physician detection was low in the ED setting. Due to the physical nature of panic attack symptoms, it is not uncommon for patients to initially seek care in medical settings (4, 15, 16), which may lead to considerable delays in receiving appropriate diagnosis and treatment. For example, data from a worldwide meta-analysis found a peak age of onset of 15.5 years for first panic attack symptoms, in contrast to a peak age at first diagnosis of panic disorder of 39.5 years (17). More than 60% of patients who visited medical settings following their first panic attack reported that these visits did little to address their concerns and may have served to increase their anxiety about future attacks (16).
When patients with panic-related anxiety do not receive timely information regarding the cause of their physical symptoms, they are more likely to return to the ED when symptoms re-occur (18, 19). This pattern has been observed worldwide and remains a considerable public health problem leading to poor long-term patient outcomes, repeat ED admissions, and unnecessary medical costs (4, 20–22). Systematic screening for panic-related anxiety by ED clinicians is likely to help considerably with early detection and right-siting of these patients earlier in the course of illness. In practice, this brief symptom-based model may support ED screening by providing clinicians with a rapid, structured way to identify patients at higher likelihood of panic-related anxiety, facilitating timely reassurance and appropriate referral after medical causes are excluded. Given its brevity and symptom-based format, the SCID could feasibly be administered by triage nurses, emergency physicians, or other trained ED staff as part of routine assessment.
Strengths and limitations
4.2
Strengths of the present study include a relatively large sample size, the use of gold-standard diagnostic interview assessments of panic-related anxiety, and the availability of complete data for all participants. Limitations include recruitment from a single ED, over-representation of Indian participants compared to the Singapore general population, and exclusion of a number of potential participants due to language barriers. Furthermore, screening of participants was restricted to weekday daytime hours, which may have affected the representativeness of the sample. Although the SCID has been widely used in multilingual clinical settings, the Mandarin administration used in this study has not undergone independent psychometric validation within this sample, which may have introduced measurement variability. Furthermore, some panic-like symptoms may have been substance-induced (e.g., related to caffeine, stimulants, or medications) rather than attributable to panic disorder, which could have contributed to misclassification and influenced model performance.
Conclusions
5
Panic-related anxiety should be strongly considered in ED patients with cardiopulmonary complaints, who frequently present to emergency medicine and are often challenging to diagnose. We have externally validated and updated a brief clinical multivariable diagnostic prediction model for timely screening of panic-related anxiety in ED patients, particularly those with chest pain who also endorse shortness of breath, dizziness, and palpitations which are the most prevalent physical symptoms in panic attacks (4). Implementing such an interview may improve early detection and proper management of patients with panic-related anxiety at presentation to the ED. Future research is needed to more fully evaluate the model’s clinical utility and impact on physician decision-making.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Davidoff J Christensen S Khalili DN Nguyen J Ishak WW . Quality of life in panic disorder: looking beyond symptom remission. Qual Life Res. (2012) 21:945–59. doi: 10.1007/s 11136-011-0020-7, PMID: 21935739 · doi ↗ · pubmed ↗
- 2Roy-Byrne PP Wagner AW Schraufnagel TJ . Understanding and treating panic disorder in the primary care setting. J Clin Psychiatry. (2005) 66 Suppl 4:16–22., PMID: 15842183 · pubmed ↗
- 3Deacon B Lickel J Abramowitz JS . Medical utilization across the anxiety disorders. J Anxiety Disord. (2008) 22:344–50. doi: 10.1016/j.janxdis.2007.03.004, PMID: 17420113 · doi ↗ · pubmed ↗
- 4Tunnell NC Corner SE Roque AD Kroll JL Ritz T Meuret AE . Biobehavioral approach to distinguishing panic symptoms from medical illness. Front Psychiatry. (2024) 15:1296569. doi: 10.3389/fpsyt.2024.1296569, PMID: 38779550 PMC 11109415 · doi ↗ · pubmed ↗
- 5Buccelletti F Ojetti V Merra G Carroccia A Marsiliani D Mangiola F . Recurrent use of the Emergency Department in patients with anxiety disorder. Eur Rev Med Pharmacol Sci. (2013) 17 Suppl 1:100–6., PMID: 23436671 · pubmed ↗
- 6Foldes-Busque G Denis I Poitras J Fleet RP Archambault P Dionne CE . A closer look at the relationships between panic attacks, emergency department visits and non-cardiac chest pain. J Health Psychol. (2019) 24:717–25. doi: 10.1177/1359105316683785, PMID: 28810369 · doi ↗ · pubmed ↗
- 7Zane RD Mc Afee AT Sherburne S Billeter G Barsky A . Panic disorder and emergency services utilization. Acad Emerg Med. (2003) 10:1065–9. doi: 10.1197/S 1069-6563(03)00349-X, PMID: 14525739 · doi ↗ · pubmed ↗
- 8Sung SC Rush AJ Earnest A Lim LEC Pek MPP Choi JMF . A brief interview to detect panic attacks and panic disorder in emergency department patients with cardiopulmonary complaints. J Psychiatr Pract. (2018) 24:32–44. doi: 10.1097/PRA.0000000000000283, PMID: 29320381 · doi ↗ · pubmed ↗