Impact of age on the management and prognosis of esophageal fistula after atrial fibrillation ablation—a subanalysis of the worldwide POTTER-AF study
Sorin S. Popescu, Zeynep G. Demirtakan, Vanessa Schmidt, Helmut Pürerfellner, Philipp Sommer, Christian Sohns, Christian Veltmann, Daniel Steven, K. R. Julian Chun, Philippe Maury, Estelle Gandjbakhch, Mikael Laredo, Stephan Willems, Thomas Beiert, Leon Iden, Anna Füting

TL;DR
This study examines how age affects the management and outcomes of esophageal fistula after heart ablation procedures for atrial fibrillation.
Contribution
The study provides new insights into age-related differences in the diagnosis and treatment of esophageal fistula following AF ablation.
Findings
Older patients had a shorter time to symptom onset after esophageal fistula.
Older patients were more likely to receive endoscopic treatment without surgery.
Older patients showed a trend toward higher fatality rates.
Abstract
Esophageal fistula (EF) is a rare but devastating complication following atrial fibrillation (AF) ablation. Data regarding the impact of age on EF are scarce. To study the impact of age on the management and prognosis of EF following catheter ablation for AF. The POTTER-AF study is a worldwide registry on EF following catheter ablation for AF. A total of 553,729 patients underwent AF ablation in 214 centers between 1996 and 2022. Of them, 138 patients experienced EF, and data regarding age, management, and prognosis were available in 113 patients. The population was divided based on the median age. The median age was 63 years; 54 patients were <63 years old (Group 1), and 59 patients were ≥63 years old (Group 2). The groups were similar regarding procedural characteristics. The older population had a shorter time to symptom onset [15.0 (6.0, 21.0) vs. 21.0 (10.0, 25.3) days; p =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
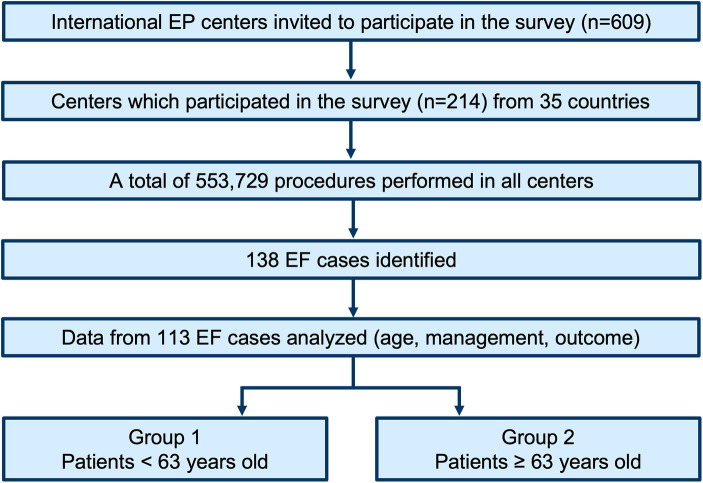 Figure 1
Figure 1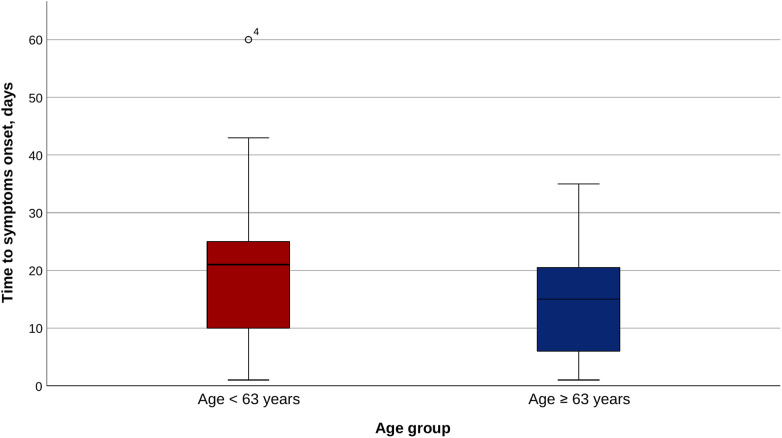 Figure 2
Figure 2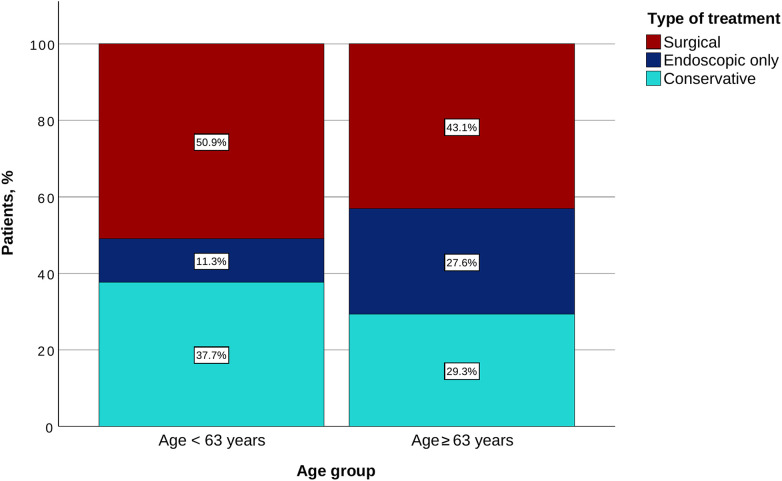 Figure 3
Figure 3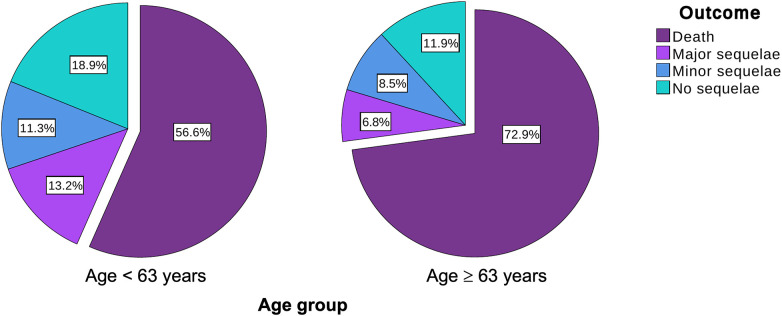 Figure 4
Figure 4| Characteristics | Age < 63 | Age ≥ 63 | |
|---|---|---|---|
| Female sex, | 24/54 (44.4%) | 28/58 (48.3%) | 0.708 |
| Body mass index, kg/m2 | 26.5 (24.4, 28.3) | 26.3 (22.7, 29.4) | 0.813 |
| Structural heart disease, | 12/53 (22.6%) | 22/59 (37.3%) | 0.104 |
| Left ventricular ejection fraction, % | 60.0 (50.0, 65.0) | 60.0 (52.5, 64.0) | 0.837 |
| Coronary artery disease, | 5/51 (9.8%) | 14/56 (25.0%) |
|
| Congestive heart failure, | 7/52 (13.5%) | 11/58 (19.0%) | 0.607 |
| Hypertension, | 23/54 (42.6%) | 43/59 (72.9%) |
|
| Diabetes, | 8/54 (14.8%) | 7/59 (11.9%) | 0.783 |
| Vascular disease, | 6/41 (14.6%) | 8/45 (17.8%) | 0.775 |
| Chronic kidney disease, | 3/42 (7.1%) | 7/46 (15.2%) | 0.320 |
| History of esogastric pathology, | 5/50 (10%) | 3/56 (5.4%) | 0.471 |
| CHA2DS2-VASc score < 3 | 43/52 (82.7%) | 23/59 (39.0%) |
|
| PPI before ablation, | 14/51 (27.5%) | 9/55 (16.4%) | 0.238 |
| Paroxysmal AF, | 23/54 (42.6%) | 25/59 (42.4%) | 1 |
| Previous AF/atrial tachycardia ablation, | 5/54 (9.3%) | 5/59 (8.5%) | 1 |
| Characteristics | Age < 63 | Age ≥ 63 | |
|---|---|---|---|
| Initial symptoms | |||
| Duration until initial symptoms, days | 21.0 (10.0, 25.3) | 15.0 (6.0, 21.0) |
|
| Duration until EF diagnosis, days | 23.0 (14.5, 32.0) | 19.0 (14.3, 29.0) | 0.240 |
| Duration from initial symptoms until EF diagnosis, days | 2.0 (1.0, 6.0) | 4.0 (0.5, 10.5) | 0.411 |
| Duration from procedure until hospital admission, days | 21.0 (12.0, 26.8) | 18.5 (12.3, 27.0) | 0.763 |
| Fever, | 33/54 (61.1%) | 34/59 (57.6%) | 0.848 |
| Chest pain/odynophagia, | 29/54 (53.7%) | 31/59 (52.5%) | 1 |
| Neurological signs, | 26/54 (48.1%) | 25/59 (42.4%) | 0.574 |
| Other symptoms, | 30/54 (55.6%) | 44/59 (74.6%) | 0.047 |
| Further complications | |||
| Stroke, | 10/48 (20.8%) | 14/54 (25.9%) | 0.642 |
| Septic shock, | 26/48 (54.2%) | 32/54 (59.3%) | 0.690 |
| Coma, | 22/48 (45.8%) | 25/54 (46.3%) | 1 |
| Cardiac arrest, | 9/48 (18.8%) | 11/54 (20.4%) | 1 |
| Tamponade, | 6/48 (12.5%) | 4/54 (7.4%) | 0.510 |
| Gastrointestinal bleeding, | 10/48 (20.8%) | 8/54 (14.8%) | 0.448 |
| Other complications, | 14/48 (29.2%) | 16/54 (29.6%) | 1 |
| Characteristics | Age < 63 | Age ≥ 63 | |
|---|---|---|---|
| Diagnostic method | |||
| Chest CT, | 43/53 (81.1%) | 46/58 (79.3%) | 1 |
| Endoscopy, | 11/53 (20.8%) | 13/58 (22.4%) | 1 |
| Echocardiography, | 12/53 (22.6%) | 16/58 (27.6%) | 0.663 |
| Brain CT or brain MRI, | 24/53 (45.3%) | 15/58 (25.9%) | |
| Others, | 12/53 (22.6%) | 7/58 (12.1%) | 0.207 |
| Type of esophageal fistula | |||
| Atrioesophageal fistula | 52/54 (96.3%) | 56/59 (94.9%) | 1 |
| Esophageal perforation | 0/54 (0.0%) | 1/59 (1.7%) | 1 |
| Esophageal–pericardial fistula | 2/54 (3.7%) | 2/59 (3.4%) | 1 |
| Characteristics | Age < 63 | Age ≥ 63 | |
|---|---|---|---|
| Conscious sedation, | 11/54 (20.4%) | 6/59 (10.2%) | 0.188 |
| Deep analgosedation, | 15/54 (27.8%) | 19/59 (32.2%) | 0.683 |
| General anesthesia, | 24/54 (44.4%) | 29/59 (49.2%) | 0.707 |
| Use of thermal probe, | 13/54 (24.1%) | 15/59 (25.4%) | 1 |
| Procedure duration, minutes | 141.5 (105.0, 183.0) | 148.5 (112.5, 180.0) | 0.895 |
| Radiofrequency, | 51/54 (94.4%) | 58/59 (98.3%) | 0.347 |
| Cryoballoon, | 2/54 (3.7%) | 1/59 (1.7%) | 0.605 |
| Laser balloon, | 1/54 (1.9%) | 0/59 (0.0%) | 0.478 |
| RF duration, minutes | 38.5 (25.3, 59.1) | 38.0 (21.0, 48.0) | 0.346 |
| PVI circumferential, | 48/49 (98.0%) | 50/55 (90.9%) | 0.210 |
| PVI segmental ostial, | 1/49 (2.0%) | 0/55 (0.0%) | 0.471 |
| PVI anatomical, | 1/49 (2.0%) | 5/55 (9.1%) | 0.210 |
| PPI postprocedural, | 39/50 (78.0%) | 42/59 (71.2%) | 0.511 |
| Characteristics | Age < 63 | Age ≥ 63 | |
|---|---|---|---|
| Esophageal surgery, | 27/53 (50.9%) | 25/58 (43.1%) | 0.450 |
|
Esophageal surgery without endoscopic treatment, | 22/53 (41.5%) | 23/58 (39.7%) | 0.849 |
| Endoscopic treatment, | 11/53 (20.8%) | 18/58 (31.0%) | 0.281 |
|
Endoscopic treatment without surgery, | 6/53 (11.3%) | 16/58 (27.6%) | 0.035 |
| Conservative treatment, | 20/53 (37.7%) | 17/58 (29.3%) | 0.421 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac Arrhythmias and Treatments · Esophageal and GI Pathology
Introduction
Atrial fibrillation (AF) is the most common arrhythmia in adults, and its prevalence is expected to double in the next few decades, posing a high burden on the healthcare systems worldwide (1, 2). Catheter ablation is the cornerstone of the rhythm control strategy and is recommended as first-line therapy in patients with paroxysmal AF and second-line therapy in those with persistent AF (2, 3).
Due to solid validation and increased operator experience, thermal ablation remains the most used technology today, with cryoballoon- and radiofrequency-based catheter ablation performed on a wide scale worldwide (4–8). Although the safety profile of these technologies improved over time due to significant technological improvements, thermal-related complications such as pulmonary vein stenosis, phrenic nerve palsy, and esophageal fistulas (EFs) cannot be completely avoided (9–14).
EF is rare but has a high fatality rate (11, 12, 14, 15). The recently published POTTER-AF study was the largest to date to investigate the incidence, management, and prognosis of EF following AF and atrial tachycardia ablation. The study reported an overall EF incidence of 0.025% and an overall fatality of 65.8%, rising up to 89.5% among patients treated conservatively (11). The anatomical proximity between the left atrium and the esophagus is a determining factor in the development of EF, and the lack of fatty tissue between the two structures increases the risk (16). In obese patients, the risk of EF formation is therefore decreased (17). There are several hypotheses on the development of atrioesophageal fistula after catheter ablation including direct thermal effects, ischemia of the esophageal mucosa via occlusion of an esophageal artery, or nerve lesions resulting in motility disorders (16, 17). As an empirical measure, mucosal protection via proton pump inhibitors (PPI) postprocedurally might be efficient in preventing the complication and is widely implemented (3, 18, 19). Esophageal temperature measurement was also suggested to prevent the development of EF; however, the current data are contradictory (14, 20).
One of the most important patient characteristics with a significant impact on ablation success and safety is age. It has been shown that advanced age is associated with a higher risk of atrial arrhythmia recurrence and a higher incidence of major cardiac adverse events (21, 22). However, the impact of age on the management and outcome of EF is unknown.
This subanalysis of the POTTER-AF study aimed to investigate the impact of patients’ age on the management and outcome of EF following catheter ablation for AF.
Methods
Study design
The POTTER-AF study is an international, multicenter, anonymized, invitation-based registry, which was conducted at the Department of Rhythmology, University Heart Centre Lübeck under the auspices of the Working Group of Cardiac Electrophysiology of the German Cardiac Society (AGEP, DGK). It was approved by the Ethics Committee of the University of Lübeck, Germany (AZ 21–291), and by the local ethics committees of all participating institutions and was registered at clinicaltrials.gov with the identification number NCT05273645. As this study represents a retrospective analysis of anonymized data, patient consent was not obtained. The study has been conducted in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Experienced electrophysiological centers were invited worldwide (11).
Data were recorded retrospectively and electronically via a standardized online questionnaire using SurveyMonkey. Patients who had an atrioesophageal fistula, esophageal–pericardial fistula, or esophageal perforation after catheter ablation were included in the POTTER-AF study. There were no exclusion criteria.
The present work is an age-based subanalysis of the POTTER-AF study, designed to evaluate the influence of age on the management and outcomes of EF following catheter ablation for AF. In addition, the analysis characterizes age-specific differences in baseline and procedural variables. The study population was divided into two cohorts according to the median age: Group 1 comprised patients younger than the median, and Group 2 included those with a median age or older.
Statistical analysis
All categorical variables were reported as absolute and relative frequencies and were compared using Fisher's exact test or the χ^2^ test, as appropriate. Continuous variables were tested for normal distribution using the Shapiro–Wilk test. They were reported as mean ± standard deviation (SD) in the case of normal distribution, otherwise as median and interquartile range (first quartile, third quartile). Continuous variables were compared using the non-paired Student's t-test when normally distributed and the Mann–Whitney U test otherwise. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 28.0 (IBM SPSS Statistics)
Results
Patient population
A total of 553,729 patients underwent ablation procedures for AF or atrial tachycardia in 214 electrophysiological centers from 35 countries between 1996 and 2022. Of them, 138 (0.025%) patients experienced postprocedural EF, and data regarding the age, management, and prognosis were available in 113 patients. The median age of the population was 63 years. A total of 54 (47.8%) patients experiencing EF were younger than 63 years old (Group 1), and 59 (52.2%) patients were at least 63 years old (Group 2) (Figure 1).
Study flowchart. EF, esophageal fistula; EP, electrophysiological.
The baseline characteristics of the two groups are depicted in Table 1. Almost half of the patients in each group were females (44.4% vs. 48.3%; p = 0.708). No difference was noted between the groups regarding the median body mass index (26.5 vs. 26.3, p = 0.813). Regarding the comorbidities, Group 2 was more likely to suffer from coronary artery disease (25.0% vs. 9.8%; p = 0.046) and hypertension (72.9% vs. 42.6%; p = 0.001). As expected, a CHA_2_DS_2_-VASc score lower than 3 was less frequent in the older population (39.0% vs. 82.7%; p < 0.001). There was no statistically significant difference between the two groups regarding the incidence of structural heart disease, congestive heart failure, diabetes, vascular disease, chronic kidney disease, and history of esophageal/gastric disease.
Symptom onset and diagnosis
The median time to symptom onset was 21.0 (10.0, 25.3) days in Group 1 and 15.0 (6.0, 21.0) days in Group 2 (p = 0.031), while the median time to EF diagnosis was 23.0 (14.5, 32.0) days and 19.0 (14.3, 29.0), respectively (p = 0.240; Figure 2). There was no significant difference between the groups regarding the initial symptoms, as well as regarding the further complications developed (Table 2).
Time to symptom onset in the two age groups.
When analyzing the diagnostic methods, Group 2 was less likely to undergo a brain computed tomography (CT) or brain magnetic resonance imaging (MRI) (25.9% vs. 45.3%; p = 0.046). There was no statistically significant difference between the use of chest CT, endoscopy, or echocardiography (Table 3).
No difference was noted between the groups regarding the proportions of atrioesophageal fistula, esophageal perforation, and esophageal–pericardial fistula (Table 3).
Procedural characteristics
The two populations were similar in terms of sedation type, energy source, and ablation techniques used, as well as in terms of esophageal temperature probe utilization (Table 4). General anesthesia was used in 44.4% of patients in Group 1 vs. 49.2% of patients in Group 2 (p = 0.707). Most of the patients underwent a radiofrequency-based catheter ablation (94.4% in Group 1 vs. 98.3% in Group 2; p = 0.347). An esophageal temperature probe was used in 24.1% of patients in Group 1 and in 25.4% of patients in Group 2 (p = 1).
Management and outcome
The older population was more likely to undergo a direct endoscopic treatment without surgery (27.6% vs. 11.3%; p = 0.035), while there was no difference regarding the rate of surgical treatment. The conservative treatment was used in similar proportions (37.7% in Group 1 vs. 29.3% in Group 2; p = 0.421) (Table 5 and Figure 3). A clear trend toward a higher fatality was noted in the older population (72.9% vs. 56.6%; p = 0.078). The incidence of major and minor sequelae was similar for both groups (Table 5 and Figure 4).
Type of treatment for each age group.
Outcome for each age group.
The fatality of EF was significantly higher in patients managed conservatively compared with that of patients treated invasively (endoscopically and/or surgically) in both Group 1 (80.0% vs. 40.6%, p = 0.009) and Group 2 (100.0% vs. 61.0%, p = 0.003).
Discussion
To the best of our knowledge, this is the first study to date to evaluate the impact of age on EF management and prognosis following catheter ablation for AF or AT. The main findings of the study are as follows:
- The time to symptom onset was significantly shorter in the older population.
- Brain CT or MRI was less commonly used among older patients.
- Direct endoscopic treatment was used more often in the older population.
- Conservative therapy was used in similar proportions of patients.
- The older patients showed a trend toward a higher fatality. Age is the main risk factor for developing AF and for its progression from paroxysmal to persistent type (1). In some studies, age is shown to predict the postprocedural complication rates after AF ablation; however, the current data are contradictory (21–28).
Regarding EF following catheter ablation for AF, it has been shown that the treatment, either endoscopic or surgical, can improve the outcome in these patients (11, 14, 29, 30). For this reason, the early diagnosis and initiation of therapy are crucial to reduce mortality. An important limitation in this case is the relatively late onset of symptoms following AF ablation, which can lead to a delayed diagnosis (11, 14, 29, 30). As demonstrated in the POTTER-AF study, the patients with an early EF detection received an early treatment via endoscopy or esophageal surgery and showed a lower fatality as compared with those with late detection, who more often received a conservative treatment (11). The present study demonstrated a shorter time to symptom onset in the elderly population, which might be at least partially explained by the frailer status of these patients. However, this difference did not translate into a lower fatality in this group, probably due to the impact of age itself on the prognosis.
When a clinical suspicion for EF occurs, the most frequently used modality for diagnosis is chest CT (11, 22, 29, 30). Transthoracic echocardiography is not sensitive enough, and transesophageal echocardiography should be avoided, as it may worsen the situation (30, 31). Esophagogastroscopy or nasogastric tube insertion might also be detrimental, as it can open the tissue flap and increase the blood flow through the fistula and aggravate systemic air embolism (32). In the present study, the most common diagnostic method was the chest CT, with similar rates in both groups. However, in the elderly population, the rate of brain CT and brain MRI was lower compared with the younger population, although the incidence of neurological symptoms was similar between the groups.
In the present study, direct endoscopic treatment without surgery was significantly more often used in the elderly group, while the surgical treatment was slightly more common in the younger population, without reaching the statistical significance level. This observation might however be biased by the clinical status of the patients, which is expected to be more deteriorated in the older group, leading to a lower rate of surgical interventions. As previously discussed, the use of a conservative approach was associated with a higher fatality as compared with endoscopic or surgical approaches (11, 12, 29, 30). In this study, the use of a conservative approach was slightly more common in the younger population, without reaching statistical significance. Given the retrospective nature of this study, the criteria guiding treatment decisions cannot be derived from our dataset. Nevertheless, several hypotheses may help explain this counterintuitive observation. One possibility is that younger patients appeared clinically more stable at presentation, prompting clinicians to opt for a conservative strategy. However, considering the high lethality of this condition, such an approach may be misleading, as conservatively managed patients generally exhibit poorer outcomes. Another contributing factor could be a longer time from symptom onset to diagnosis observed in younger individuals, potentially influencing clinical decision-making. A further explanation may relate to the perceived greater physiological reserve in younger patients, leading to the expectation that they might recover without aggressive intervention.
A trend toward higher fatality (i.e., the proportion of patients who died from EF among those who developed it) was observed in the older population. This finding should be taken into account when discussing the risks and benefits of catheter ablation for AF in this age group.
Regardless of age, it is important to emphasize that conservative management is associated with a worse prognosis, and an interventional or surgical approach should be pursued whenever feasible (11, 14).
Limitations
This is a subanalysis of a retrospective, invitation-based, international registry and comes with several specific limitations. First, the incidence of EF in the two age-based groups could not be determined due to the study design. Of note, the prevalence of mediastinal changes diagnosed by endosonography was not age dependent, so we cannot exclude that the observed age differences represent an accidental observation (33). Second, only data from patients exhibiting EF were collected, so the assessment of predictors of EF occurrence was not possible. Third, the decision regarding the management, as well as the outcome, could have been biased due to comorbidities, critical illness, and operability of the patients. Data on preoperative physical health status, such as the American Society of Anesthesiologists (ASA) score, which could have provided valuable insights into the decision-making process, were not available for this analysis. Fourth, due to the retrospective character of the registry, not all data were available for the whole population. Fifth, given the method of data acquisition via an invited survey, underreporting of these complications and the loss of detailed individual patient information cannot be excluded.
Conclusions
This is the first study to date to report on the impact of age on the management and outcome of EF following catheter ablation for AF. Older patients had initial symptoms earlier, and brain CT or brain MRI was used less commonly as a diagnostic modality in this population. Older patients who developed EF after catheter ablation were more frequently treated with direct endoscopic interventions and showed a trend toward higher fatality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kornej J Börschel CS Benjamin EJ Schnabel RB. Epidemiology of atrial fibrillation in the 21st century. Circ Res. (2020) 127(1):4–20. 10.1161/CIRCRESAHA.120.31634032716709 PMC 7577553 · doi ↗ · pubmed ↗
- 2Van Gelder IC Rienstra M Bunting KV Casado-Arroyo R Caso V Crijns HJGM 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2024) 45(36):3314–414. 10.1093/eurheartj/ehae 17639210723 · doi ↗ · pubmed ↗
- 3Tzeis S Gerstenfeld EP Kalman J Saad EB Sepehri Shamloo A Andrade JG 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace. (2024) 26(4):euae 043. 10.1093/europace/euae 04338587017 PMC 11000153 · doi ↗ · pubmed ↗
- 4Heeger CH Sano M Popescu SS Subin B Feher M Phan H-L Very high-power short-duration ablation for pulmonary vein isolation utilizing a very-close protocol—the FAST AND FURIOUS PVI study. EP Europace. (2023) 25(3):880–8. 10.1093/europace/euac 243PMC 1006236936546582 · doi ↗ · pubmed ↗
- 5Heeger CH Popescu SS Inderhees T Nussbickel N Eitel C Kirstein B Novel or established cryoballoon ablation system for pulmonary vein isolation: the prospective ICE-AGE-1 study. Europace. (2023) 25(9):euad 248. 10.1093/europace/euad 24837589146 PMC 10468200 · doi ↗ · pubmed ↗
- 6Heeger C Bohnen J Popescu S Meyer-Saraei R Fink T Sciacca V Experience and procedural efficacy of pulmonary vein isolation using the fourth and second generation cryoballoon: the shorter, the better? J Cardiovasc Electrophysiol. (2021) 32(6):1553–60. 10.1111/jce.1500933760304 · doi ↗ · pubmed ↗
- 7Heeger CH Popescu SS Saraei R Kirstein B Hatahet S Samara O Individualized or fixed approach to pulmonary vein isolation utilizing the fourth-generation cryoballoon in patients with paroxysmal atrial fibrillation: the randomized INDI-FREEZE trial. EP Europace. (2021) 24(6):921–7. 10.1093/europace/euab 305.PMC 928291234907431 · doi ↗ · pubmed ↗
- 8Kuck KH Brugada J Fürnkranz A Metzner A Ouyang F Chun KRJ Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med. (2016) 374(23):2235–45. 10.1056/NEJ Moa 160201427042964 · doi ↗ · pubmed ↗