A biopsychosocial perspective on endometriosis: the importance of psychological inflexibility
Sophia Åkerblom, Ingrid Peppler Jönsson, Åsa Ringqvist, Johanna Nordengren, Xiang Zhao

TL;DR
This study explores how psychological factors, especially psychological inflexibility, play a key role in endometriosis symptoms and suggests new treatment approaches.
Contribution
The study highlights psychological inflexibility as a novel key factor in endometriosis symptom networks.
Findings
Psychosocial variables like perceived control and depression are central to endometriosis symptoms.
Biological factors had low relevance in the symptom network.
Psychological inflexibility emerged as the most important psychological process in the study.
Abstract
Treatment strategies for endometriosis have traditionally been biomedical. There is a need for a more multidimensional understanding of endometriosis and more targeted and individualized treatment interventions, including psychological approaches. The aims of this study were twofold: (1) to identify key biopsychosocial characteristics in individuals attending a tertiary clinic for endometriosis and (2) to inform the development of future, targeted, and efficacious interventions by examining the importance of psychological processes central to two scientific models, pain catastrophizing and fear of movement from the fear-avoidance model, and psychological inflexibility from the psychological flexibility model. Psychosocial variables, more specifically perceived control and powerlessness, social support, and depression, were of particular importance to the symptom structure in this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
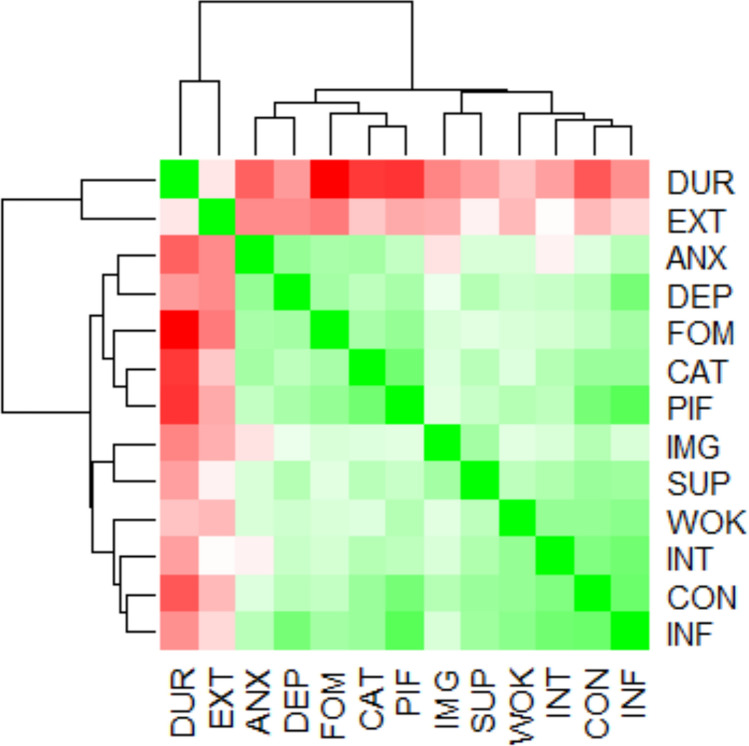 Figure 1
Figure 1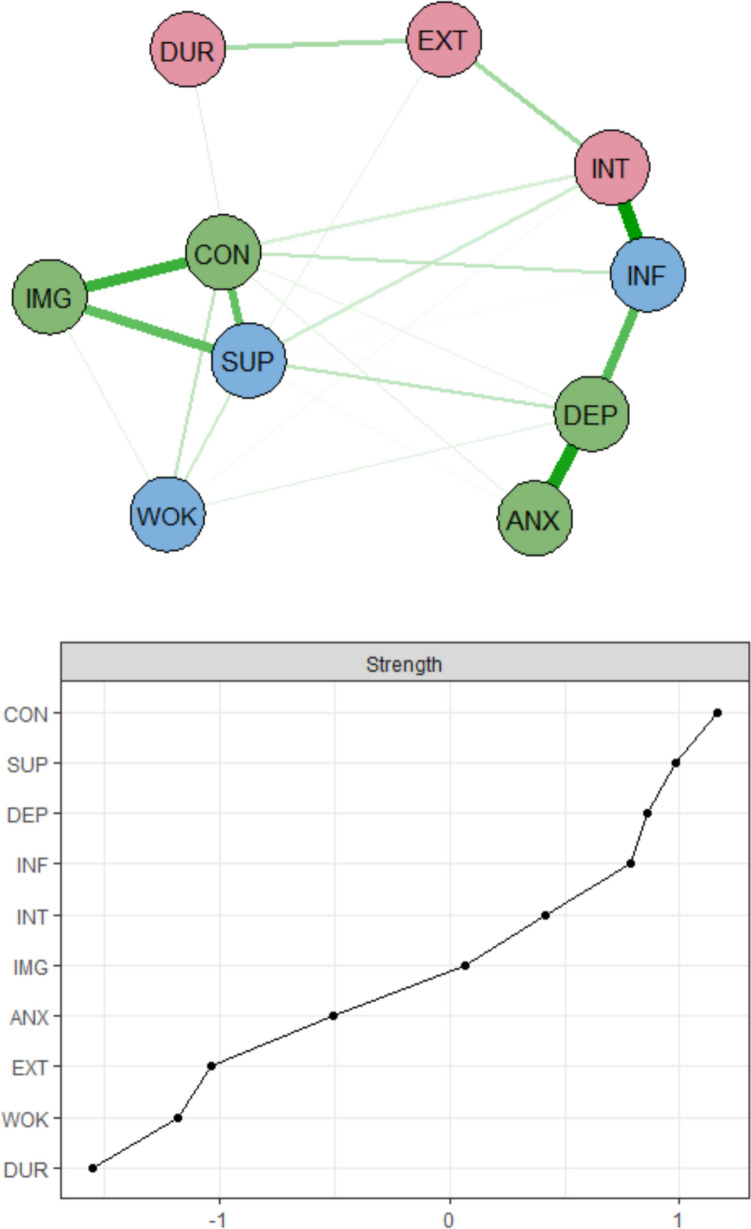 Figure 2
Figure 2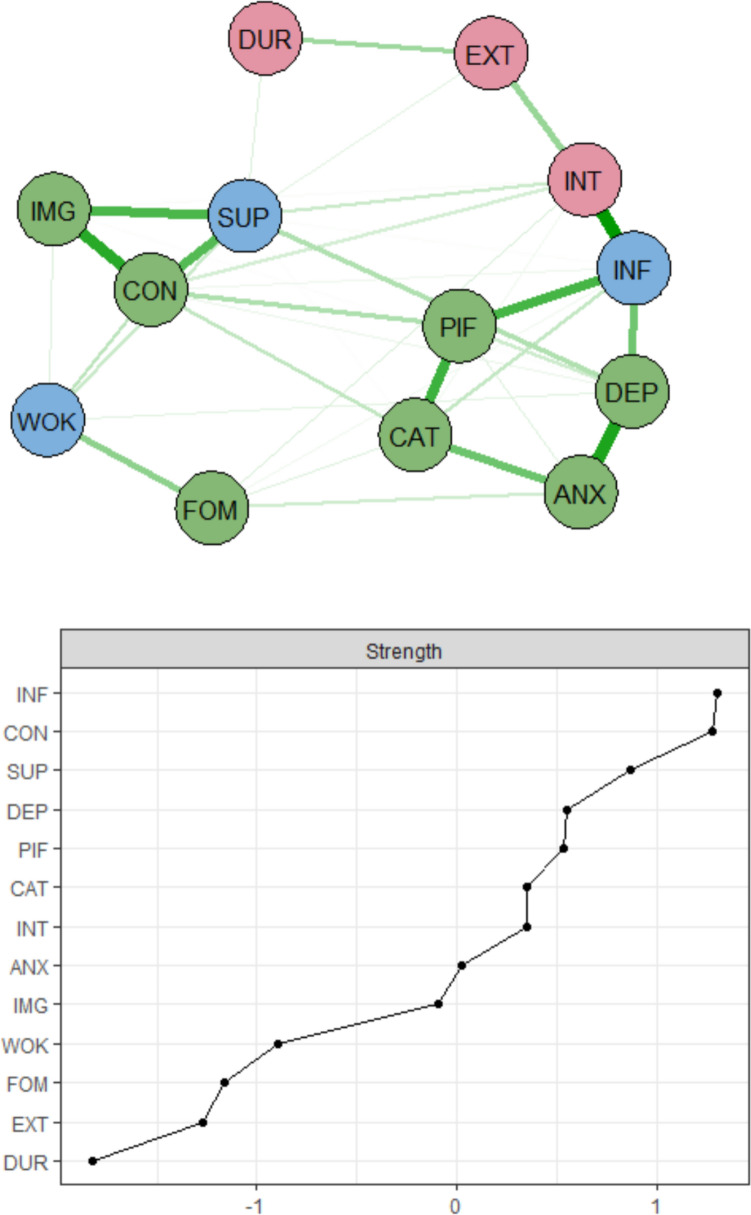 Figure 3
Figure 3- —Skåne University Hospital Psychology Research and Development Grant
- —Lund University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometriosis Research and Treatment · Neuroendocrine regulation and behavior · Attachment and Relationship Dynamics
What does this study add to the clinical work?
A multidimensional approach based on the biopsychosocial model seems to be useful in understanding, assessing, and treating endometriosis. Psychological treatments and in particular interventions based on the psychological flexibility model, such as Acceptance and Commitment Therapy, may be effective for individuals living with endometriosis
Introduction
Endometriosis is an inflammatory disease in which endometrial-like tissue grows outside the uterus, affecting an estimated 10% of women worldwide [1, 2]. Characteristic symptoms include painful menstruation, ovulation, intercourse, and defecation; urinary tract and gastrointestinal symptoms; and fertility problems [1]. A significant proportion of individuals with endometriosis experience chronic pelvic pain, and pain is widely recognized as a cardinal symptom of the condition [1, 3, 4]. Endometriosis can also lead to far-reaching social and psychological consequences, including psychiatric comorbidities, such as depression and anxiety, reduced quality of life, and negative effects on key life areas, such as relationships, sexuality, fertility, work, and leisure [5–9]. The symptoms of endometriosis are complex, heterogeneous, and multidimensional, pointing to the fact that the symptom profiles might be better understood from a biopsychosocial viewpoint, where the dynamic interplay of biological, psychological, and social factors is considered together [10, 11].
Still, treatment strategies for endometriosis are typically biomedical, and a baseline treatment is often hormone therapy to reduce endometriosis-associated dyspareunia, dysmenorrhea, and non-menstrual pain, which cannot be tolerated by some due to side effects [12, 13]. Different analgesics for pain management are frequently prescribed, and in certain instances surgical methods are implemented. Surgical interventions can be of benefit to selected individuals and offer pain relief for some individuals [14, 15]. However, medical interventions are connected to a heightened risk of iatrogenic consequences and physical, psychological, and social adverse events, such as serious side effects, repeated surgery due to recurrence of pain, and worsened symptoms and quality of life [15–21]. Individuals with insignificant effects from these treatments are frequently prescribed long-term opioids for pain control, which has an associated risk of amplified pain from opioid-induced hyperalgesia, disability, tolerance, and heightened risk of addiction and overdose [22, 23].
Taken together, there is a need for more targeted and individualized treatment interventions for individuals with endometriosis, incorporating psychological, biological, and social factors [10, 24]. Calls have also been made for effective psychological treatment of endometriosis [24, 25], but thus far psychological research and treatment methods within the field have been relatively sparse, and further exploration is needed [12, 13, 26, 27].
Evidence-based treatment programs for chronic pain are grounded in the biopsychosocial model and commonly use psychological principles, most often cognitive behavioral therapy (CBT) [25]. CBT has proven to be effective for chronic pain and might be a promising candidate for improved quality of life in endometriosis [24, 25]. The fear-avoidance model is a focused CBT model centered on chronic pain [28]. Kinesiophobia or fear of movement, and catastrophizing are core concepts within this long-established and active scientific model [29–32]. The psychological flexibility model, which also stems from the CBT tradition, has gained increasing empirical support in the chronic pain field over the past decade. This growing support is largely due to accumulating evidence that greater psychological flexibility, characterized by openness to experience, present-moment awareness, and value-based action, is associated with improved adjustment and reduced disability among individuals with chronic pain [28, 33]. Kinesiophobia, pain catastrophizing, and psychological (in) flexibility have been established as key treatment mechanisms in interventions for chronic pain and have gained some attention in endometriosis [26, 28, 31, 34–37]. However, the psychological processes most relevant to endometriosis and the interventions likely to benefit affected individuals remain largely unknown [26, 27].
Complex relations among psychological, social, and biological factors can be captured using network analysis [38]. This statistical tool has been widely used within psychiatry and clinical psychology to outline symptom structures, identify important features of different conditions, and gain insight into important psychological mechanisms underlying specific conditions [39–42]. The aims of this study are twofold: (1) to identify key biopsychosocial characteristics in individuals attending a tertiary clinic for endometriosis and (2) to inform the development of future, targeted, and efficacious interventions by examining the importance of psychological processes central to two scientific models, pain catastrophizing and fear of movement from the fear-avoidance model, and psychological inflexibility from the psychological flexibility model.
Methods
Participants
Participants were 113 individuals with painful, either laparoscopically or ultrasound-verified endometriosis, referred for assessment at the endometriosis clinic at Skåne University Hospital between April 2019 and May 2024. The endometriosis clinic is part of the Swedish National Health Service, serving as a regional, specialist center providing healthcare services to individuals with endometriosis. The study was approved by the Swedish Ethical Review Authority (2019-00023) and participants provided informed consent.
Measures
For analytical clarity, factors were grouped into biological, psychological, and social categories. This categorization provides a clear framework for interpreting the structure and patterns of associations in the network analysis, thereby facilitating a more meaningful understanding of how different domains of the biopsychosocial model interact in the context of endometriosis. However, some constructs (such as pain interference) encompass elements of more than one domain, consistent with the integrative nature of the model. In this context, psychological process factors, such as psychological inflexibility, represent underlying mechanisms that shape psychological adaptation and act as key targets for intervention within the scientific models examined.
Biological factors
Pain duration was registered in years.
Pain intensity was measured with the Numerical Rating Scale (NRS). The NRS is well-established and is used in pain research to measure pain intensity over the past week on an 11-point scale (0 = no pain; 10 = worst possible pain). The NRS detects variations in pain level in different contexts [43, 44].
Pain extent, or the number of pain locations, was assessed using 36 predefined anatomical areas (18 on the right side of the body and 18 on the left) and patients indicated the areas where they experienced pain: (1) head/face, (2) neck, (3) shoulder, (4) upper arm, (5) elbow, (6) forearm, (7) hand, (8) anterior aspect of chest, (9) lateral aspect of chest, (10) abdomen, (11) sexual organs, (12) upper back, (13) lower back, (14) hip/gluteal area, (15) thigh, (16) knee, (17) shank, and (18) foot. The number of pain locations (range: 0–36) was summed.
Social factors
Pain interference was measured using this specific subscale from the Multidimensional Pain Inventory Version 2 (MPI) [45]. Pain interference is rated on a seven-point scale (0 = never; 6 = very often) in the areas of family and marital functioning, work and work-related activities, and social and leisure activities. A mean interference score is computed, with higher scores denoting greater functional impairment from pain. The MPI has adequate psychometric properties [46] and the Swedish version used in this study has shown good sensitivity in pain outcome studies [47].
Social support and work life were measured with these specific subscales from the Endometriosis Health Profile-30 (EHP-30). The EHP-30 assesses health-related quality of life in individuals with endometriosis. Social support was measured using a main subscale of the EHP-30, whereas work life was assessed with a supplementary module subscale, which also covers additional areas, including relationships with children, sexual relationships, feelings about the medical profession, feelings about treatment, and feelings about infertility. The items are rated on a five-point scale (0 = never; 4 = always). For each domain, the scores are converted to a 0–100 scale, with 0 representing the best health-related quality of life and 100 the worst [48]. The psychometric properties of both the original and Swedish versions of the EHP-30 have been deemed to be valid and reliable [48, 49].
Psychological factors
Control and powerlessness and self-image were also measured with these specific subscales from the Endometriosis Health Profile-30 (EHP-30) as described above. Again, for each domain, the scores are converted to a 0–100 scale, with 0 representing the best health-related quality of life and 100 the worst [48].
Rates of anxiety and depression were assessed with the 14-item Hospital Anxiety and Depression Scale (HADS) [50], with seven anxiety and seven depression items, respectively. The items are rated from 0 to 3, with higher scores indicating greater levels of depression and anxiety over the past week. Scores of 0–7, 8–10, and 11–21 represent cutoff points for non-cases, doubtful cases, and clinical cases [50]. The psychometric properties of the English original and of the Swedish version used in this study are well-established and widely accepted [50, 51].
Psychological process factors
Catastrophic thinking was assessed using the 13-item Pain Catastrophizing Scale (PCS), which evaluates three dimensions: helplessness, magnification, and rumination [52]. The items are scored on a five-point scale (0 = not at all; 4 = all the time) and are added to produce a total score, where higher scores represent greater catastrophizing. The psychometric properties of the measure are well-established [52].
Psychological inflexibility was assessed using the Psychological Inflexibility in Pain Scale (PIPS) [53]. The 12 items are scored on a seven-point scale (1 = never true; 7 = always true), where higher scores indicate a greater degree of psychological inflexibility. The psychometric properties of the Swedish PIPS are acceptable [53].
Fear of movement or reinjury (kinesiophobia) was measured using the Tampa Scale of Kinesiophobia (TSK) [54]. The 17 items are rated on a four-point scale (1 = strongly disagree; 4 = strongly agree). Higher scores indicate greater levels of kinesiophobia. Both the original and Swedish versions of the TSK have displayed satisfactory psychometric properties [54–56].
Analysis
The study constructs were organized broadly following the biopsychosocial framework [10]. Biological factors included pain duration, pain intensity, and pain extent. Psychological factors were anxiety, depression, control and powerlessness, and self-image. Psychological process factors, pain catastrophizing and fear of movement (the fear-avoidance model) and psychological inflexibility (the psychological flexibility model) were also included here. Social factors included pain interference, social support, and work life. Given the cross-sectional nature of the data, undirected (rather than directed) networks were used to encapsulate the complex and reciprocal interplays among the biopsychosocial symptoms. Each symptom was regarded as a node in the system [57]. To estimate the connections (i.e., edges) between nodes, the EBICglasso algorithm was applied, which is based on an LASSO method [58]. In the visualization, thicker edges reflect stronger partial correlations; green and red links mean positive and negative associations, respectively. To relax the normality assumption in estimation, a nonparanormal transformation (“npn”) was also applied to normalize the data [59]. While the packages produce several centrality metrics for networks, we only used strength centrality, as it is considered the most interpretable metric in psychosomatic data [60]. The strength metric refers to a measure of centrality that considers the weights of the edges connected to a node: \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$${s}_{i}=\sum_{j\ne i}\left|{\omega }_{ij}\right|$$\end{document} , where \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$${\omega }_{ij}$$\end{document} is the weight of the edge between nodes i and j. Because the absolute values of the weights are used, the metric reflects the overall magnitude of connections, regardless of their positive or negative direction. Thus, the nodes with relatively larger strength values possess more direct connections and stronger partial correlations with other nodes. In our context, nodes with larger strength values represent the most influential symptoms in the biopsychosocial networks. To examine the stability of networks and centrality values, we used 1000 bootstraps for each edge as well as for the strength metrics. Based on visual inspection, most visible and strong edges did not include zero in the bootstrapped networks. Even when the subset sample comprised 40% of the original sample, the strength estimate remained above 0.70. The packages “qgraph” [61] and “bootnet” [62] were used to estimate and visualize the networks using R. Pairwise deletion was used to handle missing data.
Results
Descriptive information of sample
The study included 113 women. On average, participants were 36.9 years (SD = 8.0), with ages ranging from 21 to 61 years. The majority of participants (70.8%) were born in Sweden or other Nordic countries. Regarding education, 62.5% of participants had completed tertiary education, while 27.7% had completed secondary education. The average reported duration of pain was 12.1 years. Participants reported an average pain extent of 9.7 locations. For more details, see Table 1. Using the supplementary parts of the EHP-30 participants rated the following areas if relevant to them: work life, relationship with children, sexual relationship, feelings about the medical profession, feelings about treatment, and feelings about infertility (Table 2). Taken together, work life, sexual relationship, and feelings about treatment appeared to be the subscales most relevant to the individuals in this study. A minority felt that the children and infertility subscales were relevant to them. The subscales reflecting the worst health status were sexual relationship, feelings about treatment, and feelings about infertility. Table 1. Means, standard deviations and minimum and maximum values for the sample on the network variablesVariableMeanSDMinMaxINT5.632.74010EXT9.716.71036DUR12.1010.17034INF3.621.4906DEP7.874.42019ANX10.294.67021WOK45.0028.400100SUP50.3527.300100CON63.0125.970100IMG56.0027.780100PIF57.8314.541984CAT31.8612.28152FOM39.659.991962INT pain intensity (NRS), EXT number of pain locations, DUR pain duration, INF pain interference (MPI), DEP depression (HADS), ANX anxiety (HADS), WOK work life (EHP-30), SUP social support (EHP-30), CON control and powerlessness (EHP-30), IMG self-image (EHP-30), PIF psychological inflexibility (PIPS), CAT pain catastrophizing (PCS), FOM fear of movement (TAMPA)Table 2. Descriptive information from the EHP-30 supplementary modulesSubscoreValid cases (%)MeanSDWork life76 (67.3%)45.0028.40Relationship with children49 (43.4%)34.6925.29Sexual relationship73 (64.6%)59.4531.42Feelings about the medical profession66 (58.4%)40.1527.10Feelings about treatment70 (61.9%)57.0225.13Feelings about infertility41 (36.3%)55.7930.89
Networks and centrality metrics
Bivariate Spearman’s correlations were first examined and visualized using a heatmap (Fig. 1). Apart from the intercorrelations among the EHP-30 subscales, the remaining variables only showed sporadic associations with other variables. Notably, the dendrogram on the sides of the heatmap briefly delineates the clustering of nodes. Three main clusters emerged: (1) a biological cluster, encompassing pain duration and pain extent; (2) an emotions and psychological processes cluster, which includes depression, anxiety, catastrophizing, psychological inflexibility, and fear of movement; and (3) a pain-related cluster, consisting of pain interference and intensity, along with four EHP-30 subscales: work life, social support, control and powerlessness, and self-image.Fig. 1. Heatmap with a dendrogram. INT pain intensity (NRS), EXT number of pain locations, DUR pain duration, INF pain interference (MPI), DEP depression (HADS), ANX anxiety (HADS), WOK work life (EHP-30), SUP social support (EHP-30), CON control and powerlessness (EHP-30), IMG self-image (EHP-30), PIF psychological inflexibility (PIPS), CAT pain catastrophizing (PCS), FOM fear of movement (TAMPA)
As illustrated in the first biopsychosocial network (without the psychological process factors), pain interference, pain intensity, anxiety, and depression were closely connected, forming a cluster comprising pain aspects and negative emotions. Three subscales (control and powerlessness, social support, and self-image) of the EHP-30 formed another close cluster (Fig. 2), the EHP-30-based cluster. In terms of centrality, biological factors showed limited relevance within the network, with pain extent and pain duration displaying low strength values. In contrast, control and powerlessness and social support demonstrated multiple, strong connections with other nodes. As shown in the centrality plot, control and powerlessness had the largest strength values in the network, followed by social support and depression. All of these variables were classified as psychological or social nodes.Fig. 2. Network with strength centrality plot. There are three domains in nodes: red = biological nodes, green = psychological nodes, blue = social nodes. In the strength centrality plot, z-scores are shown on the x-axis rather than raw centrality indices. INT pain intensity (NRS), EXT number of pain locations, DUR pain duration, INF pain interference (MPI), DEP depression (HADS), ANX anxiety (HADS), WOK work life (EHP-30), SUP social support (EHP-30), CON control and powerlessness (EHP-30), IMG self-image (EHP-30)
When the psychological process nodes were added (Fig. 3), the EHP-30-based cluster remained, but pain catastrophizing and psychological inflexibility were incorporated into the first cluster, together with pain aspects and negative emotions.Fig. 3. Network with strength centrality plot. There are three domains in nodes: red = biological nodes, green = psychological nodes, blue = social nodes. In the strength centrality plot, z-scores are shown on the x-axis rather than raw centrality indices. INT pain intensity (NRS), EXT number of pain locations, DUR pain duration, INF pain interference (MPI), DEP depression (HADS), ANX anxiety (HADS), WOK work life (EHP-30), SUP social support (EHP-30), CON control and powerlessness (EHP-30), IMG self-image (EHP-30), PIF psychological inflexibility (PIPS), CAT pain catastrophizing (PCS), FOM fear of movement (TAMPA)
Control and powerlessness and social support remained the leading nodes, but pain interference ranked higher than both. Interestingly, psychological inflexibility, pain catastrophizing, and fear of movement showed different connectivities with other nodes. Fear of movement was positioned closer to the work life subscale of the EHP-30, whereas psychological inflexibility and pain catastrophizing clustered more closely with depression, anxiety, and pain interference. Among the psychological process variables, psychological inflexibility exhibited comparatively higher strength centrality than the others. Fear of movement emerged as the least important psychological process node in the network. Visually, psychological inflexibility showed a strong and direct connection with pain interference, while pain catastrophizing was strongly connected with anxiety.
Discussion
There is a need for a multidimensional understanding of endometriosis and for more targeted, personalized treatment interventions, including psychological approaches. The first aim of this study was to identify key biopsychosocial characteristics in individuals attending a tertiary clinic for endometriosis. One major finding was that psychosocial variables emerged as the most central elements in this biopsychosocial symptom network, when the psychological process variables were not included. The strongest variable was control and powerlessness, closely followed by social support and depression. These factors appear to be central targets for intervention in endometriosis, suggesting that enhancing perceived control, strengthening social support, and alleviating depressive symptoms may promote better overall adjustment.
These findings are consistent with previous research showing that depression is a common comorbidity in endometriosis [8, 63, 64] and that social support serves as an important resilience factor [65]. Both social support and perceived control have been associated with quality of life in individuals with endometriosis, and improvements in these factors have been observed following psychological treatment [66]. Because such processes are often targeted in psychological therapies, such as CBT [28], these results suggest that psychological interventions may be of particular value in endometriosis. This is consistent with recent meta-analytic evidence emphasizing the potential of psychological treatments to reduce pain and improve mental and physical well-being in this population [27]. However, current international guidelines (e.g., [15]) conclude that, at present, no firm recommendations can be made regarding the effectiveness of psychological interventions for improving pain or quality of life in individuals with endometriosis, highlighting the need for further rigorous research in this area [15].
In contrast, biological factors such as pain extent and pain duration showed lower centrality in the biopsychosocial network, suggesting they may play a less integrative role in the symptom structure compared to psychosocial factors. This pattern could indicate that once pain becomes chronic, its established features are less intertwined with pain-related functioning as compared to psychological processes, such as perceived control, catastrophizing, or depression, which exert broader influences across the network. These findings contrast with current treatment approaches for endometriosis, which are typically biomedical [12, 13], but are in line with previous studies in other chronic pain populations, where pain extent has shown limited relevance when outlining symptom structures and understanding functioning [42, 67].
The second aim of this study was to inform the development of future, targeted, and efficacious psychological interventions by examining the importance of psychological processes central to two scientific models, pain catastrophizing and fear of movement (the fear-avoidance model), and psychological inflexibility (the psychological flexibility model). Psychological inflexibility emerged as the most central psychological process in the network, ranking among the stronger nodes. These findings are in accordance with the scarce existing research on endometriosis, where a single study has demonstrated that psychological flexibility, and its counterpart psychological inflexibility, are relevant to functioning in individuals with endometriosis [26]. These findings align with previous studies, where therapeutic processes from the psychological flexibility model have been identified as essential for functioning in chronic pain populations [47, 68–70] and have been shown to be more influential than fear of movement for treatment outcomes in chronic pain interventions [71]. The psychological flexibility model emphasizes healthy activity and well-being achieved through increases in psychological flexibility and Acceptance and Commitment Therapy (ACT) is based on this model [72]. Psychological flexibility involves the ability to act in alignment with one’s values despite psychological or physical discomfort, whereas psychological inflexibility represents difficulty engaging in meaningful activities due to avoidance or fusion with distressing internal experiences. Psychological flexibility entails six core therapeutic processes: acceptance, cognitive defusion, present-focused awareness, self-as-context, committed action, and value-based action, which can be summarized as behavioral patterns that are open, aware, and engaged [73]. Research on the psychological flexibility model and ACT has grown substantially in recent years, and empirical support for this model and treatment approach in chronic pain is robust [68]. Moreover, a recent study suggests that such treatment strategies may also be beneficial for individuals with endometriosis [66]. Overall, the study enhances our knowledge of the psychological factors involved in endometriosis and provides a foundation for developing and testing targeted psychological interventions. Based on the findings of this study, interventions focused on psychological inflexibility appear particularly promising for individuals with endometriosis, as they may improve functioning, reduce avoidance behaviors, and enhance engagement in valued activities. Building on these findings, future studies could empirically test this approach through well-designed pilot studies or randomized controlled trials, assessing changes in pain, physical functioning, quality of life, and psychological flexibility. Furthermore, investigating which subgroups, such as patients with varying symptom severity, care settings, or diagnostic status, benefit most could help guide tailored intervention strategies.
Even if the relevance of pain catastrophizing was not as strong as psychological inflexibility, it still appears to be a meaningful treatment target in endometriosis. Catastrophizing is a core component from the fear-avoidance model, reflecting a tendency to amplify negative thoughts and emotions related to pain [52, 74]. In chronic pain populations, such as those with fibromyalgia, pain catastrophizing has been associated with greater pain intensity, emotional distress, disability, and poorer treatment outcomes [75–77]. The significance of pain catastrophizing in endometriosis has also been highlighted in earlier studies [34, 35], underscoring its role as a key factor in pain-related functioning [28, 78]. Fear of movement showed low relevance in this symptom network, which contrasts with previous research emphasizing its importance in chronic pain populations [29, 79]. One possible explanation for this discrepancy is that endometriosis-related pain may be less directly linked to movement or physical activity compared to musculoskeletal pain conditions, where movement often triggers pain and reinforces avoidance behaviors.
Strengths of the study included the selection of the population, as only patients with laparoscopically or ultrasound-verified endometriosis were included, and the inclusion of a wide array of aspects from the biopsychosocial model in the analyses. Nonetheless, the present findings must be interpreted in light of certain limitations. All measures were self-reported, which may introduce response biases or common method variance that could affect the observed associations between variables and the interpretation of centrality findings. Moreover, all measures included were organized according to the biopsychosocial model, with most factors being psychological, which may have influenced the results. The cross-sectional design of the study precluded the identification of causal directions. The study sample was relatively small and drawn from a tertiary care clinical service, with some participants scheduled for surgical interventions. Consequently, the results may not fully reflect symptom patterns in patients treated at primary or secondary care settings, or in individuals without a formal diagnosis of endometriosis, who may differ in symptom severity, treatment history, or other clinical characteristics. The self-report measure PIPS was used to measure psychological inflexibility. While the PIPS has satisfactory psychometric properties [53], cross-validation studies suggest that the total score may not fully capture all aspects of psychological flexibility/inflexibility, such as present-focused awareness, self-as-context, committed action, and value-based action [80, 81]. Future research could address these limitations by employing alternative or complementary measures of psychological flexibility and recruiting larger, more diverse samples from different levels of care to enhance the representativeness and generalizability of the findings.
In conclusion, a biopsychosocial approach appears to be particularly useful in understanding endometriosis. Despite the current treatment regimen being predominately biomedical, psychosocial variables, such as perceived control and powerlessness, social support, and depression were especially important for the symptom structure in this patient population with laparoscopically or ultrasound-verified endometriosis. When aiming to inform future, promising psychological interventions for endometriosis, psychological inflexibility emerged as the most central psychological process in the network. Interventions based on this model, such as ACT, may hold promise for improving outcomes in this population, but this requires testing in future studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Institute for Health and Care Excellence (2017) Endometriosis: diagnosis and management (NG 73). NICE, London; 2022. https://www.nice.org.uk/guidance/ng 7329787038 · pubmed ↗