Evaluating the real-world safety of cholestyramine for the treatment of hyperlipidemia: disproportionality analysis of FAERS data
Qiang Li, Mengmeng Fan, Anbang Gao, Limin Qin

TL;DR
This study assesses the real-world safety of cholestyramine, a drug used for high cholesterol and bile acid disorders, by analyzing adverse event reports.
Contribution
The study identifies both known and previously undocumented adverse reactions of cholestyramine using FAERS data.
Findings
Confirmed known adverse reactions like constipation, bloating, and vitamin deficiencies.
Identified new adverse reactions not listed in the drug's package insert, including GERD and tooth fracture.
Highlighted the importance of monitoring adverse events in real-world clinical use.
Abstract
Hypercholesterolemia is a significant risk factor for severe cardiovascular diseases. Cholestyramine lowers serum low-density lipoprotein cholesterol (LDL-C) levels and is clinically indicated for the treatment of primary hypercholesterolemia, relieve itching symptoms caused by bile acid accumulation in cholestatic diseases (such as primary biliary cirrhosis), as well as to manage bile acid diarrhea resulting from bile acid metabolic disorders. With its widespread clinical application, it is essential to understand its safety in real-world settings. This study evaluated the clinical safety of cholestyramine by analyzing all adverse event reports since 2004 in the FDA Adverse Event Reporting System (FAERS), where cholestyramine was identified as the primary suspected drug. Bayesian Confidence Propagation Neural Network (BCPNN), the Medicines and Healthcare Products Regulatory Agency…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
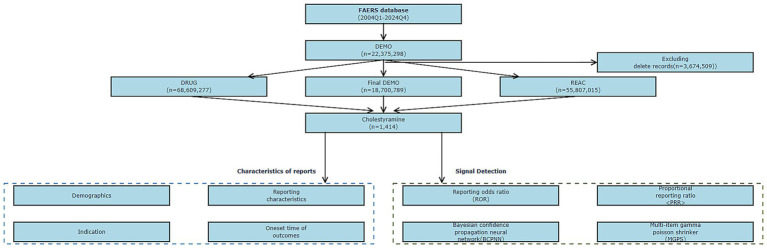 Figure 1
Figure 1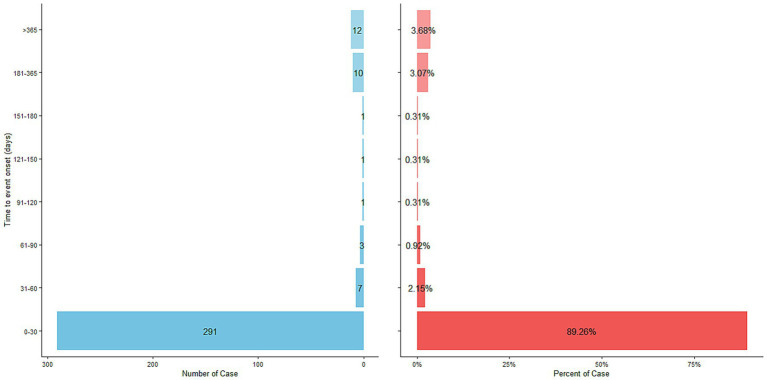 Figure 2
Figure 2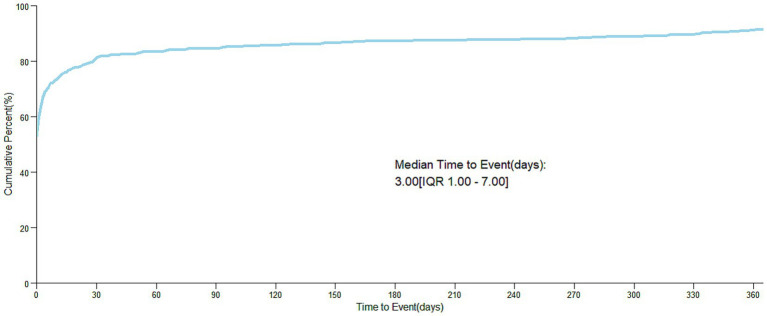 Figure 3
Figure 3| Characteristics | Number of cases | Proportion of cases (%) |
|---|---|---|
| Number of AE reports | 1,414 | |
| Sex | ||
| Male | 341 | 24.11 |
| Female | 878 | 62.09 |
| Not specified | 195 | 13.79 |
| Age | ||
| <18 | 7 | 0.5 |
| 18–65 | 258 | 18.25 |
| >65 | 340 | 24.05 |
| Not specified | 809 | 57.21 |
| Reporter | ||
| Consumer | 988 | 69.87 |
| health-professor | 36 | 2.55 |
| Other health professional | 42 | 2.97 |
| Pharmacist | 123 | 8.7 |
| Physician | 183 | 12.94 |
| Not specified | 42 | 2.97 |
| Reporting year | ||
| 2004 | 16 | 1.13 |
| 2005 | 10 | 0.71 |
| 2006 | 3 | 0.21 |
| 2007 | 7 | 0.50 |
| 2008 | 15 | 1.06 |
| 2009 | 12 | 0.85 |
| 2010 | 7 | 0.50 |
| 2011 | 6 | 0.42 |
| 2012 | 9 | 0.64 |
| 2013 | 11 | 0.78 |
| 2014 | 9 | 0.64 |
| 2015 | 100 | 7.07 |
| 2016 | 113 | 7.99 |
| 2017 | 139 | 9.83 |
| 2018 | 128 | 9.05 |
| 2019 | 211 | 14.92 |
| 2020 | 107 | 7.57 |
| 2021 | 130 | 9.19 |
| 2022 | 144 | 10.18 |
| 2023 | 100 | 7.07 |
| 2024 | 137 | 9.69 |
| Top 5 reporting countries | ||
| United States of America | 1,271 | 89.89 |
| France | 7 | 0.5 |
| Germany | 7 | 0.5 |
| Great Britain | 5 | 0.35 |
| Denmark | 3 | 0.21 |
| Outcome | ||
| Life-threatening | 10 | 3.95 |
| Hospitalization—initial or prolonged | 57 | 22.53 |
| Disability | 12 | 4.74 |
| Death | 5 | 1.98 |
| Required intervention to prevent permanent impairment/damage | 8 | 3.16 |
| Congenital anomaly | 10 | 3.95 |
| Other | 151 | 59.68 |
| System organ class (SOC) | Case reports | ROR (95% CI) | PRR (95% CI) | IC (IC025) | EBGM (EBGM05) |
|---|---|---|---|---|---|
| Gastrointestinal disorders | 1,026 | 3.869 | 3.191 | 1.561 | 3.190 |
| Product issues | 795 | 34.534 | 28.390 | 4.655 | 28.330 |
| Injury, poisoning and procedural complications | 713 | 3.026 | 2.693 | 1.301 | 2.692 |
| General disorders and administration site conditions | 534 | 0.926 | 0.935 | −0.236 | 0.935 |
| Respiratory, thoracic and mediastinal disorders | 336 | 2.770 | 2.632 | 1.220 | 2.632 |
| Investigations | 211 | 1.429 | 1.409 | 0.283 | 1.409 |
| Nervous system disorders | 174 | 0.727 | 0.738 | −0.664 | 0.738 |
| Musculoskeletal and connective tissue disorders | 101 | 0.668 | 0.676 | −0.854 | 0.676 |
| Skin and subcutaneous tissue disorders | 99 | 0.634 | 0.643 | −0.928 | 0.643 |
| Metabolism and nutrition disorders | 45 | 1.194 | 1.192 | −0.183 | 1.192 |
| Psychiatric disorders | 39 | 0.374 | 0.380 | −1.835 | 0.380 |
| Immune system disorders | 39 | 1.262 | 1.260 | −0.137 | 1.260 |
| Infections and infestations | 31 | 0.260 | 0.265 | −2.395 | 0.265 |
| Renal and urinary disorders | 28 | 0.661 | 0.663 | −1.116 | 0.663 |
| Hepatobiliary disorders | 20 | 1.416 | 1.415 | −0.161 | 1.414 |
| Neoplasms benign, malignant and unspecified (incl cysts and polyps) | 14 | 0.722 | 0.723 | −1.190 | 0.723 |
| Vascular disorders | 13 | 0.250 | 0.252 | −2.682 | 0.252 |
| Congenital, familial and genetic disorders | 13 | 11.480 | 11.449 | 1.938 | 11.440 |
| Blood and lymphatic system disorders | 12 | 0.449 | 0.451 | −1.890 | 0.451 |
| Eye disorders | 12 | 0.434 | 0.435 | −1.939 | 0.435 |
| Cardiac disorders | 11 | 0.273 | 0.275 | −2.607 | 0.275 |
| Ear and labyrinth disorders | 10 | 0.802 | 0.803 | −1.164 | 0.803 |
| Reproductive system and breast disorders | 8 | 1.102 | 1.102 | −0.840 | 1.102 |
| Surgical and medical procedures | 8 | 0.910 | 0.910 | −1.085 | 0.910 |
| Pregnancy, puerperium and perinatal conditions | 6 | 0.872 | 0.873 | −1.263 | 0.873 |
| Social circumstances | 2 | 2.428 | 2.427 | −1.244 | 1.618 |
| Endocrine disorders | 2 | 0.914 | 0.915 | −2.180 | 0.610 |
| Preferred term (PT) | Case reports | ROR (95% CI) | PRR (95% CI) | IC (IC025) | EBGM (EBGM05) |
|---|---|---|---|---|---|
| Diarrhoea | 183 | 4.275 | 4.137 | 1.802 | 4.136 |
| Product solubility abnormal | 176 | 562.874 | 540.083 | 6.820 | 518.357 |
| Product taste abnormal | 170 | 194.677 | 187.089 | 6.246 | 184.421 |
| Product use in unapproved indication | 159 | 10.465 | 10.118 | 3.021 | 10.111 |
| Product substitution issue | 150 | 38.401 | 37.108 | 4.658 | 37.004 |
| Product physical consistency issue | 126 | 373.663 | 362.842 | 6.284 | 352.913 |
| Drug ineffective for unapproved indication | 94 | 25.610 | 25.077 | 4.017 | 25.030 |
| Product use complaint | 92 | 101.602 | 99.469 | 5.283 | 98.713 |
| Constipation | 85 | 5.895 | 5.800 | 2.139 | 5.797 |
| Throat irritation | 69 | 22.806 | 22.459 | 3.751 | 22.421 |
| Abdominal pain upper | 65 | 4.622 | 4.568 | 1.754 | 4.566 |
| Abdominal discomfort | 62 | 5.405 | 5.342 | 1.951 | 5.340 |
| Retching | 59 | 40.530 | 39.993 | 4.219 | 39.872 |
| Product use issue | 49 | 3.913 | 3.880 | 1.462 | 3.879 |
| Foreign body in throat | 47 | 270.495 | 267.576 | 4.926 | 262.143 |
| Cough | 44 | 2.290 | 2.277 | 0.712 | 2.277 |
| Choking | 42 | 31.411 | 31.116 | 3.747 | 31.044 |
| Product odour abnormal | 42 | 61.697 | 61.110 | 4.224 | 60.826 |
| Product residue present | 41 | 122.560 | 121.411 | 4.519 | 120.285 |
| Product quality issue | 38 | 3.874 | 3.849 | 1.376 | 3.848 |
| Dysgeusia | 36 | 6.677 | 6.630 | 2.045 | 6.627 |
| Flatulence | 33 | 8.498 | 8.441 | 2.292 | 8.436 |
| Oropharyngeal pain | 32 | 4.967 | 4.938 | 1.634 | 4.937 |
| Blood glucose increased | 28 | 2.070 | 2.063 | 0.453 | 2.063 |
| Choking sensation | 28 | 74.082 | 73.610 | 3.851 | 73.197 |
| Dyspepsia | 27 | 4.004 | 3.985 | 1.299 | 3.985 |
| Abdominal distension | 26 | 3.641 | 3.625 | 1.164 | 3.624 |
| Oropharyngeal discomfort | 23 | 40.256 | 40.048 | 3.336 | 39.927 |
| Product physical issue | 22 | 16.636 | 16.557 | 2.698 | 16.537 |
| Dysphagia | 21 | 3.196 | 3.185 | 0.916 | 3.185 |
| Gastrointestinal disorder | 14 | 2.433 | 2.429 | 0.401 | 2.429 |
| Tooth discolouration | 14 | 65.849 | 65.640 | 2.879 | 65.312 |
| Intentional product use issue | 13 | 2.186 | 2.182 | 0.235 | 2.182 |
| Gastrooesophageal reflux disease | 13 | 2.344 | 2.340 | 0.320 | 2.340 |
| Illness | 12 | 2.082 | 2.079 | 0.138 | 2.079 |
| Drug effective for unapproved indication | 12 | 6.508 | 6.493 | 1.387 | 6.490 |
| Foreign body in mouth | 11 | 2287.538 | 2281.741 | 2.741 | 1938.068 |
| Dysphonia | 11 | 2.696 | 2.692 | 0.402 | 2.692 |
| Product packaging difficult to open | 10 | 70.630 | 70.470 | 2.395 | 70.091 |
| Product availability issue | 10 | 7.280 | 7.266 | 1.338 | 7.262 |
| Rectal haemorrhage | 10 | 3.264 | 3.258 | 0.562 | 3.258 |
| Intestinal obstruction | 10 | 3.965 | 3.958 | 0.768 | 3.957 |
| Throat tightness | 10 | 5.297 | 5.287 | 1.055 | 5.286 |
| Therapeutic response unexpected | 10 | 3.096 | 3.092 | 0.504 | 3.091 |
| Poor quality product administered | 10 | 16.749 | 16.713 | 1.910 | 16.693 |
| Poor quality product administered | 10 | 16.749 | 16.713 | 1.910 | 16.693 |
| Reaction to excipient | 9 | 57.991 | 57.873 | 2.198 | 57.618 |
| Foreign body in respiratory tract | 9 | 90.471 | 90.286 | 2.269 | 89.663 |
| Abnormal faeces | 9 | 15.860 | 15.830 | 1.757 | 15.811 |
| Oral discomfort | 9 | 9.118 | 9.101 | 1.415 | 9.095 |
| Abnormal faeces | 9 | 15.860 | 15.830 | 1.757 | 15.811 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions · Advanced Causal Inference Techniques · Meta-analysis and systematic reviews
Introduction
1
Coronary heart disease (CHD) is one of the most common and severe cardiovascular disease. Its high incidence and case-fatality rate threaten patients’ lives, markedly degrade quality of life, and impose a heavy burden on the health-care systems (1). Hypercholesterolemia, particularly elevated levels of low-density lipoprotein cholesterol (LDL-C), is an important risk factor for CHD and myocardial infarction (MI) (2). Excess LDL-C deposits in the coronary intima, forming atherosclerotic plaques that narrow or occlude vessels, precipitating myocardial ischaemia, angina, and potentially MI. Consequently, is essential to prevent cardiovascular events, Excess LDL-C deposits in the coronary intima, forming atherosclerotic plaques that narrow or occlude vessels, precipitating myocardial ischemia, angina, and potentially MI (3). Consequently, aggressive lipid management, and in particular maintaining LDL-C within target ranges, is crucial for preventing cardiovascular events, retard atherogenesis, and reduce CHD morbidity and mortality.
Cholestyramine, an anion-exchange resin that sequesters bile acid in the gut, interrupts their enterohepatic circulation.
The drug is indicated for primary hypercholesterolaemia—particularly in statin-intolerant patients—and for cholestatic pruritus (e.g., in primary biliary cholangitis) and bile-acid diarrhoea caused by malabsorption. Although its efficacy is well established, safety concerns persist. By binding intestinal bile acids, cholestyramine can impair fat digestion and cause bloating, constipation, or diarrhoea. It also reduces absorption of fat-soluble vitamins (A, D, E, and K), potentially leading to osteoporosis (vitamin D deficiency) or bleeding disorders (vitamin K deficiency).
The resulting bile-acid depletion drives hepatic conversion of cholesterol to new bile acids, thereby reducing serum LDL-C levels (4). It is clinically used primarily for the treatment of primary hypercholesterolemia, especially in patients who are intolerant to statins (4, 5). It is also used to relieve itching symptoms caused by bile acid accumulation in cholestatic diseases (such as primary biliary cirrhosis) and to manage bile acid diarrhea resulting from bile acid malabsorption (6–8). Although the efficacy of cholestyramine is well-established, safety concerns persist. By binding intestinal bile acids, cholestyramine can impair fat digestion and cause constipation, bloating or diarrhea (9). It also reduces the absorption of fat-soluble vitamins (A, D, E, and K), increasing the risk of deficiencies in these vitamins (10). This can, in turn, potentially leading to osteoporosis (vitamin D deficiency) or coagulation disorders (vitamin K deficiency).
The FDA adverse event reporting system (FAERS) is a global pharmacovigilance database that collects spontaneously reported adverse events (AEs) from healthcare professionals, patients, and pharmaceutical companies to detect post-marketing safety signals. Compared with clinical trials, FAERS offers larger sample sizes, longer observation, and greater population diversity, making it particularly effective in detecting rare or delayed adverse events. Data-mining of FAERS, for example, researchers have successfully identified mental status changes, conversion disorder, and eye movement disorder caused by Regadenoson, highlighting its value in pharmacovigilance (11). As clinical experience accumulates, FAERS mining suggests that the full safety profile of cholestyramine may have gradually been identified.
Materials and methods
2
Data source
2.1
This study relied on the open data resources of the US FAERS to conduct a retrospective analysis of adverse events related to cholestyramine. The data covered the period from the first quarter of 2004 to the fourth quarter of 2024, and the inclusion criteria were all ASCII format original report data that labeled cholestyramine as the “primary suspect drug.” This database integrates drug safety information submitted by global medical staff, patients, and pharmaceutical companies through a spontaneous reporting mechanism.
This study utilized publicly available data from the U.S. Food and drug administration adverse event reporting system (FAERS). The data were accessed and used in accordance with the terms and conditions specified by the FAERS database, ensuring compliance with all relevant regulations and guidelines. As the data are de-identified and publicly accessible, no individual patient information was disclosed, and no additional ethical approval was required for this study. The study design and analysis were conducted in a manner that respects patient privacy and confidentiality. The authors declare no conflicts of interest related to the use of FAERS data in this research.
Data processing procedure
2.2
The data cleaning and standardization process included three stages as follows. The first stage implemented the FDA-recommended hierarchical deduplication strategy, which involved sorting by case unique identifier (CASEID) and prioritizing the report with the most recent receipt date (FDA_DT), selecting the record with a larger PRIMARYID value when CASEID and FDA_DT were completely the same, and synchronizing the verification of the deletion list for quarterly data update packages after 2019 to exclude invalid entries. The second stage completed medical coding transformation, based on MedDRA terminology library version 27.1, to uniformly map the original adverse event descriptions to standardized preferred terms (PT) and system organ classification (SOC). The final stage constructed a structured dataset, and the specific processing procedure is shown in Figure 1, the technical roadmap.
Flowchart demonstrating the AE analysis process for cholestyramine using the FAERS database. AE, adverse event; DEMO, demographic data; DRUG, drug; FAERS, FDA adverse event reporting system; REAC, reaction data; ROR, reporting odds ratio; PRR, proportional reporting ratio; BCPNN, Bayesian confidence propagation neural network; MGPS, multi-item gamma Poisson shrinker; SOC, system organ class; PS, primary suspect; PT, preferred term.
Statistical analysis strategy
2.3
An incremental analysis framework was adopted: (1) descriptive statistics: to parse the composition characteristics of the dataset from dimensions such as demographic characteristics, report sources, and geographical distribution; (2)signal detection: integrating four internationally accepted disproportionality analysis methods—reporting odds ratio (ROR), proportional reporting ratio (PRR, with thresholds set according to the MHRA standard), Bayesian confidence propagation neural network (BCPNN), and multi-item gamma Poisson shrinkage (MGPS); (3)time series modeling: constructing a Weibull distribution model to explore the temporal dynamic characteristics of adverse events. The analysis process was implemented on the SAS 9.4 platform, and the algorithm parameters and calculation formulas are detailed in Supplementary Tables S1, S2.
An incremental analysis framework was adopted, including descriptive statistics to parse the composition characteristics of the dataset from dimensions such as demographic characteristics, report sources, and geographical distribution; signal detection integrating four internationally accepted disproportionality analysis methods—reporting odds ratio (ROR), proportional reporting ratio (PRR) with thresholds set according to the MHRA standard, Bayesian confidence propagation neural network (BCPNN), and multi-item gamma Poisson shrinkage (MGPS), and time series modeling constructing a Weibull distribution model to explore the temporal dynamic characteristics of adverse events. The analysis process was implemented on the SAS 9.4 platform, and the algorithm parameters and calculation formulas are detailed in Supplementary Tables S1, S2.
Results
3
Clinical characteristics
3.1
A total of 1,414 adverse event reports with cholestyramine as the primary suspect drug were included in this study (Figure 1). Among them, 62.09% were female patients, 24.11% were male patients, and 13.79% had unknown gender. The age group with the highest proportion was >65 years old (24.05%), followed by the 18–65 years group (18.25%), with the <18 years group being the least (0.5%), and 57.21% had unknown age. Most reports were submitted by consumers (69.87%), doctors (12.94%), pharmacists (8.7%), and other health professionals (5.52%). Adverse events were mainly concentrated in the years 2015–2024 after the drug was marketed, with very few adverse events occurring in 2004–2015, which is considered to be related to the initial lack of widespread application of the drug. 89.89% of the reports came from the United States. Adverse reactions often led to patient hospitalization (22.53%), disability (4.74%), or life-threatening conditions (3.95%). See Table 1 for details.
Adverse event distribution at the system organ class (SOC) level
3.2
Adverse events related to cholestyramine involved all 27 SOC classifications. As shown in Table 2, significant categories included, but were not limited to gastrointestinal disorders, product issues, injury, poisoning and procedural complications, general disorders and administration site conditions, respiratory, thoracic and mediastinal disorders, investigations, nervous system disorders, musculoskeletal and connective tissue disorders, skin and subcutaneous tissue disorders, metabolism and nutrition disorders, psychiatric disorders, immune system disorders, infections and infestations, and renal and urinary disorders. Table 2 shows the signal strength at the SOC level.
Adverse event distribution at the preferred term (PT) level
3.3
Adverse events related to cholestyramine were sorted by frequency of occurrence and assessed for signals. Among the adverse events in the FAERS, the side effects mentioned in the package insert are as follows. The most common adverse reaction is constipation, especially in patients with high doses of cholestyramine and those over 60 years old. Less common adverse reactions include abdominal discomfort, bloating, nausea, vomiting, diarrhea, belching, anorexia, steatorrhea, bleeding tendency, night blindness, hyperchloremic acidosis, osteoporosis, rash, and local irritation caused by vitamin K, A, and D deficiency. In children, there have been rare reports of intestinal obstruction (including two deaths), and some patients may experience biliary calcification or biliary colic, but these may be related to liver disease rather than directly caused by the drug. Other reported events (not necessarily related to the drug) include gastrointestinal symptoms (such as rectal bleeding, dysphagia, pancreatitis, etc.), laboratory test abnormalities (liver function abnormalities, prolonged prothrombin time, etc.), allergic reactions (urticaria, asthma, dyspnea, etc.), musculoskeletal pain, nervous system symptoms (headache, anxiety, vertigo, dizziness, fatigue, tinnitus, syncope, somnolence, femoral neuralgia, paresthesia, etc.), and eye and kidney problems (uveitis, hematuria, etc.).
Adverse reactions not mentioned in the package insert found by FAERS analysis include as following. Off-label use, unapproved indications, intentional product misuse, and use of prescription drugs without a prescription. Product-related issues, including issues with product solubility, taste, physical consistency, formulation, packaging, supply, container, and product quality issues, physical contamination of the product, product sedimentation, etc. Newly discovered adverse reactions include discomfort or abnormalities in the respiratory tract, mouth, and throat (foreign body sensation in the mouth, foreign body sensation in the throat, foreign body sensation in the respiratory tract, dysphonia, cough, choking, choking sensation, oropharyngeal pain, tooth discoloration, gastroesophageal reflux disease, irritable bowel syndrome, etc.), fecal abnormalities (color change, softening, hardening), and abnormal urine odor. Others are as follows: blood glucose fluctuations, tooth fracture, exacerbation of concomitant diseases, etc. Table 3 shows the details of the top 50 adverse events at the PT level. All adverse events that meet the positive signal criteria are listed in the Supplementary Table.
Time of adverse event occurrence
3.4
After excluding reports with false or missing adverse event occurrence times, 326 cholestyramine-related adverse events provided occurrence time data. Most adverse events occurred immediately after administration (n = 234, 71.78%) and within 3 days after administration (1 day after administration n = 14, 4.29%; 2 days after administration n = 6, 1.84%; 3 days after administration n = 7, 2.15%), with the highest proportion of adverse reactions occurring within 1 month after administration (n = 291, 89.26%). Rare cases occurred 2 months (n = 7, 2.15%), 3 months (n = 3, 0.92%), 4 months (n = 1, 0.31%), 5 months (n = 1, 0.31%), 6 months (n = 1, 0.31%), 7 to 12 months (n = 10, 3.07%), and more than 1 year (n = 12, 3.68%) after administration. The median occurrence time was 3 days (interquartile range [IQR] 1.00–7.00 days). The time distribution is shown in Figure 2, and the cumulative incidence curve is shown in Figure 3.
Time to event report distribution of AE reports. AE, adverse event.
Cumulative incidence of AEs. AE, adverse event.
Discussion
4
Hypercholesterolemia is a metabolic disorder characterized by elevated blood cholesterol, particularly LDL-C (12). Aetiologically, it is subdivided into primary forms (familial monogenic or polygenic hypercholesterolemia), and secondary forms attributable to diseases (such as hypothyroidism, diabetes, and liver disorders) or drugs (such as glucocorticoids and β-blockers) (13). Irrespective of cause, hypercholesterolemia is an independent driver of atherosclerosis, stroke, and CHD, and therefore constitutes a serious human-health threat (14). The therapeutic cornerstoen is to reduce LDL-C levels to attenuate atherosclerosis and cardiovascular diseases. Cholestyramine is a bile acid-binding resin that lowers plasma LDL-C levels by binding bile acids in the intestine and promoting the metabolism of cholesterol to bile acids in cells, and it can be used for patients intolerant to statins (15). Despite its well-documented efficacy safety concerns regarding cholestyramine persist. Through data mining of the FAERS database, this study uncovers potential serious adverse events associated with cholestyramine use, highlighting findings of substantial clinical significance.
This investigation conducted a comprehensive assessment of adverse events related to cholestyramine since its market release in 2004. By analyzing the FAERS database, the study confirmed the common adverse events listed in the drug’s package insert, including constipation, abdominal discomfort, bloating, nausea, vomiting, diarrhea, belching, anorexia, steatorrhea, and bleeding tendencies, night blindness, hyperchloremic acidosis, osteoporosis, rashes, and local irritation caused by deficiencies in vitamins K, A, and D. Additionally, potential adverse events not listed in the package insert were identified, such as off-label use, unapproved indications, discomfort or abnormalities in the respiratory tract, mouth, and throat, gastroesophageal reflux disease (GERD), irritable bowel syndrome (IBS), fecal abnormalities (color changes, softening, hardening), blood glucose fluctuations, tooth fracture, and exacerbation of concomitant diseases. These findings highlight the importance of strengthening drug monitoring, especially during the initial administration of cholestyramine, to effectively manage potential side effects.
It is noteworthy that the formulation of cholestyramine—a powder requires reconstitution before administration—may increase the risk of medication errors. Data from the FAERS indicate that the incidence of esophageal obstruction or mucosal injury is significantly higher in patients who swallow the drug directly without dissolving it compared to other formulations. Off-label use, identified as a potential risk factor for adverse reactions associated with cholestyramine, refer to clinical prescribing practices that extend beyond the approved indications, target populations, dosages, or target populations approved by drug regulatory authorities in the drug’s package insert (16). Currently, off-label use is prevalent in clinical practice for several reasons. Firstly, the absence of targeted therapies for certain diseases, such as rare diseases, prompts doctors to explore new therapeutic applications for existing drugs. Secondly, although emerging evidence may support the efficacy of a drug for a new indication, pharmaceutical companies may not have pursued regulatory approval for that use. Thirdly, the need for individualized treatment arises when patients are intolerant to conventional treatments and require dosage adjustments. Lastly, cost considerations lead patients to choose cheaper old drugs over expensive new ones due to economic issues (17). Thus, it appears that appropriate explanations are: when using cholestyramine, doctors or pharmacists may not clearly instruct patients, and patients may not use cholestyramine according to the required indications, dosages, etc., in the package insert, leading to off-label use. To mitigate these risks, clinicians should adhere to standardized prescribing protocols and reinforce patient education regarding proper medication handling and potential adverse effects.
GERD is another potential adverse reaction. GERD refers to a condition where the contents of the duodenum or stomach reflux into the esophagus, mouth, or airway, causing reflux esophagitis or damage to extra-esophageal tissues (18). Common manifestations of GERD include persistent cough, heartburn, acid regurgitation, and chest pain. The pathogenesis of GERD is highly complex and may involve the direct corrosive effects of stomach acid and pepsin on the esophageal mucosa, vagal nerve dysfunction, inflammatory responses, increased esophageal sensitivity, and Helicobacter pylori infection (19). Known adverse reactions of cholestyramine include nausea and vomiting (20). Thus, a possible explanation is that cholestyramine use, which causes nausea and vomiting, leads to the reflux of stomach contents, including stomach acid and pepsin, into the esophagus, directly corroding the esophageal mucosa and causing esophageal inflammation, erosion, and even ulcers. The relationship between cholestyramine and GERD needs further research to be proven, but this adverse reaction provides a basis for doctors to prevent GERD when using cholestyramine in patients with hypercholesterolemia.
IBS has been identified as a potential adverse reaction associated with cholestyramine use. IBS is a functional gastrointestinal disorder characterized by symptoms such as abdominal pain, bloating, and changes in bowel habits (21). Its current incidence ranges from 2 to 12%, though actual rates are likely higher, with a slightly predominance in females. IBS is typically classified into four subtypes: constipation-predominant, diarrhea-predominant, mixed, and unsubtyped IBS (22). The condition is often recurrent and chronic, significantly affecting patients’ quality of life. Studies indicate that IBS arises from a multifactorial interplay of elements, including psychological disorders, gastrointestinal motility abnormalities, gastrointestinal infections and inflammation, visceral hypersensitivity, and gastrointestinal hormones (23). These underlying mechanisms align with several documented adverse reactions of cholestyramine, such as constipation, abdominal discomfort, and diarrhea. Thus, a plausible explanatory mechanism is that cholestyramine induced constipation, abdominal discomfort, or diarrhea may disrupt gastrointestinal motility, visceral hypersensitivity, exacerbate intestinal infections or inflammation, and alter gastrointestinal hormone secretion, collectively contributing to the occurrence of IBS. During treatment with cholestyramine, close monitoring of intra-abdominal pressure, bowel movements, and other gastrointestinal parameters is recommended. If symptoms such as increased intra-abdominal pressure, abdominal pain, diarrhea, or constipation occur, IBS should be considered in the differential diagnosis. Physicians should advise patients to remain vigilant regarding these potential adverse reactions when prescribing cholestyramine.
Our study also suggests that fecal abnormalities (color changes, softening, hardening) are potential risks associated with cholestyramine. Fecal abnormalities indicate issues with the digestive system or other problems and are commonly manifested as: abnormal color, such as tarry stools indicating upper gastrointestinal bleeding or iron use, bright red stools indicating lower gastrointestinal bleeding such as anal fissures or colorectal cancer, and grayish-white stools possibly caused by biliary obstruction; changes in consistency, such as watery stools indicating infection, food poisoning, or allergies, and hard stools indicating constipation or intestinal obstruction, steatorrhea suggesting pancreatitis (24, 25). Fecal abnormalities are often accompanied by symptoms such as abdominal pain, diarrhea, fever, and weight loss. This corresponds with the known adverse reactions of cholestyramine, such as diarrhea and steatorrhea (26). A plausible explanation is that cholestyramine use, which binds bile acids in the intestines, leads to fatty acid metabolic disturbances and poor fat absorption, causing watery stools and steatorrhea. The relationship between cholestyramine and fecal abnormalities needs further research to be confirmed, but this adverse reaction provides a basis for doctors to monitor fecal tests in patients treated with cholestyramine.
Blood glucose fluctuations are potential adverse reactions identified in our study. Blood glucose fluctuations, also known as glycemic variability, refer to the unstable state of blood glucose levels fluctuating between high and low values at different time intervals (27). Physiological blood glucose fluctuations occur under the regulation of the neuroendocrine system to adapt to environmental changes, with a general fluctuation range of 2–3 mmol/L within 24 h (28). Patients, due to infections, stress, and other factors, may experience pancreatic cell damage, increased insulin resistance, and increased secretion of glucagon and other hormones, resulting in more significant blood glucose levels and fluctuation amplitudes compared to normal individuals (29). The cause of blood glucose fluctuations induced by cholestyramine may be that cholestyramine binds to bile acids in the intestines, indirectly affecting fat metabolism and intestinal hormones, impacting insulin sensitivity. Cholestyramine may affect the absorption of other hypoglycemic drugs such as metformin, influencing blood glucose fluctuations. Further research is needed to explore the relationship between cholestyramine and blood glucose fluctuations. In summary, blood glucose fluctuations are potential adverse reactions identified in our study. When using cholestyramine, closely monitor blood glucose changes and provide timely symptomatic treatment.
Tooth fracture has been identified as a potential adverse reaction associated with cholestyramine. Tooth fracture refers to the transverse or longitudinal splitting of teeth caused by trauma, biting hard objects, or weakened tooth structure (30). The organic content in teeth decreases with age, while the inorganic content gradually increases, causing teeth to become more brittle; after biting hard objects, enamel damage can lead to tooth fractures (31). This corresponds with the known adverse reactions of cholestyramine, such as vitamin D deficiency and osteoporosis. A plausible explanation is that cholestyramine use, which causes vitamin D deficiency and osteoporosis, leads to thinner and more fragile bone tissue, making teeth more susceptible to damage or fractures; severe osteoporosis can cause thinning of the alveolar bone, leading to loose teeth, receding gums, and tooth loss. This adverse reaction provides a basis for doctors to advise patients to be cautious about such adverse reactions when treating them with cholestyramine for hypercholesterolemia.
Exacerbation of concomitant diseases is a potential adverse reaction identified in our study. Exacerbation of concomitant diseases refers to the increased risk of worsening conditions and symptom intensification when multiple diseases coexist in a patient, commonly seen in elderly patients, those with chronic illnesses, and individuals with weakened immune systems. The causes of exacerbation of concomitant diseases may include: interactions between different diseases leading to complex conditions, decreased immunity making patients more susceptible to infections, and interactions between different medications affecting drug efficacy (32). The cause of exacerbation of concomitant diseases induced by cholestyramine may be: cholestyramine binding to bile acids in the intestines indirectly affects fat metabolism and the secretion of intestinal hormones, reducing immunity; cholestyramine use, which causes deficiencies in vitamins K, A, and D, leading to bleeding tendencies, may exacerbate damage to other organs. In summary, exacerbation of concomitant diseases is a potential adverse reaction identified in our study. When treating patients with cholestyramine, doctors should advise patients to be cautious about such adverse reactions.
This study conducted a disproportionality analysis of the FAERS data and predicted the cumulative incidence and timing of adverse reactions associated with cholestyramine as the primary suspect drug. This indicates the need for early detection and treatment of related adverse reactions following cholestyramine treatment for hypercholesterolemia and other diseases. This provides strong evidence for the prevention and treatment of adverse reactions, which is beneficial for reducing adverse reactions and improving disease prognosis.
The study has certain limitations. Firstly, the FAERS database is a reporting system provided by patients, pharmacists, and doctors, and there may be inaccuracies and missing data. We have implemented a rigorous data processing procedure, including correcting obvious data entry errors and deleting duplicate reports, to increase the sample size and offset the impact of individual inaccurate data, making our conclusions more accurate. Secondly, our data are all from the United States, so the conclusions are more biased towards North America and may have deviations for regions in Asia, Africa, and Latin America. Lastly, while the FAERS database can provide potential risks of adverse reactions, it offers limited assistance with patient epidemiological data.
Conclusion
5
This study utilized FAERS data to conduct a disproportionality analysis of adverse events associated with cholestyramine, focusing on all reports from the first quarter of 2004 to the fourth quarter of 2024. The analysis results confirmed known adverse reactions of cholestyramine, such as constipation, abdominal discomfort, bloating, nausea, vomiting, diarrhea, belching, anorexia, steatorrhea, and bleeding tendencies, night blindness, hyperchloremic acidosis, osteoporosis, rashes, and local irritation caused by deficiencies in vitamins K, A, and D. It also identified potential adverse reactions such as off-label use, unapproved indications, discomfort or abnormalities in the respiratory tract, mouth, and throat, GERD, IBS, fecal abnormalities (color changes, softening, hardening), blood glucose fluctuations, tooth fracture, and exacerbation of concomitant diseases. These findings underscore the necessity of early monitoring of adverse reactions in patients to ensure the safe application of cholestyramine in the treatment of hypercholesterolemia and other diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Groenendyk JW Greenland P Khan SS. Incremental value of polygenic risk scores in primary prevention of coronary heart disease: a review. JAMA Intern Med. (2022) 182:1082–8. doi: 10.1001/jamainternmed.2022.3171, 35994254 · doi ↗ · pubmed ↗
- 2Shaya GE Leucker TM Jones SR Martin SS Toth PP. Coronary heart disease risk: low-density lipoprotein and beyond. Trends Cardiovasc Med. (2022) 32:181–94. doi: 10.1016/j.tcm.2021.04.002, 33872757 · doi ↗ · pubmed ↗
- 3Bjornson E Adiels M Taskinen MR Burgess S Chapman MJ Packard CJ . Lipoprotein(a) is markedly more atherogenic than LDL: an apolipoprotein B-based genetic analysis. J Am Coll Cardiol. (2024) 83:385–95. doi: 10.1016/j.jacc.2023.10.039, 38233012 PMC 7616706 · doi ↗ · pubmed ↗
- 4Macchiaiolo M Gagliardi MG Toscano A Guccione P Bartuli A. Homozygous familial hypercholesterolaemia. Lancet. (2012) 379:1330. doi: 10.1016/S 0140-6736(11)61476-122285056 · doi ↗ · pubmed ↗
- 5Sjoberg BG Straniero S Angelin B Rudling M. Cholestyramine treatment of healthy humans rapidly induces transient hypertriglyceridemia when treatment is initiated. Am J Physiol Endocrinol Metab. (2017) 313:E 167–74. doi: 10.1152/ajpendo.00416.2016, 28487440 · doi ↗ · pubmed ↗
- 6Beuers U Wolters F Oude Elferink RPJ. Mechanisms of pruritus in cholestasis: understanding and treating the itch. Nat Rev Gastroenterol Hepatol. (2023) 20:26–36. doi: 10.1038/s 41575-022-00687-7, 36307649 · doi ↗ · pubmed ↗
- 7Scaldaferri F Pizzoferrato M Ponziani FR Gasbarrini G Gasbarrini A. Use and indications of cholestyramine and bile acid sequestrants. Intern Emerg Med. (2013) 8:205–10. doi: 10.1007/s 11739-011-0653-0, 21739227 · doi ↗ · pubmed ↗
- 8Selim R Ahn J. Pruritus in chronic liver disease. Clin Liver Dis. (2023) 27:47–55. doi: 10.1016/j.cld.2022.08.01136400466 · doi ↗ · pubmed ↗