Ischemic Colitis Secondary to Mesenteric Arteriovenous Malformation: A Rare Cause of Bowel Ischemia—Case Report and Literature Review
Arparat Kanacharoen, Nantaporn Srivanitchapoom, Pornrujee Hirunpat, Nuttapat Tungtrongchitr

TL;DR
A rare case of ischemic colitis caused by a mesenteric arteriovenous malformation is reported, highlighting the importance of early diagnosis and surgical treatment.
Contribution
Presents a rare case of ischemic colitis due to a mesenteric arteriovenous malformation and emphasizes the role of CT angiography in diagnosis.
Findings
Ischemic colitis was caused by an arteriovenous malformation in the inferior mesenteric artery.
Surgical resection and ligation of the AVM resolved the patient's symptoms.
Early CT angiography is crucial for diagnosing mesenteric AVMs in cases of ischemic colitis.
Abstract
Ischemic colitis is the most common form of intestinal ischemia, typically caused by a temporary reduction in blood flow to the colon. It is often linked to atherosclerosis, low blood pressure, or embolism. We present a case of ischemic colitis with atypical location due to an inferior mesenteric arteriovenous malformation (inferior mesenteric artery–vein) in a 77‐year‐old woman with Child‐Turcotte‐Pugh Class A hepatitis C cirrhosis. She had a 2‐day history of rectal bleeding, mild abdominal pain, and nausea. Colonoscopy findings show segmental erythematous and edematous mucosa with multiple discrete shallow ulcers in the sigmoid and descending colons (23–30 cm from the anal verge). Computed tomography (CT) and CT angiography showed an arteriovenous malformation (AVM) supplied by the inferior mesenteric artery, draining into the inferior mesenteric vein, consistent with ischemic colitis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
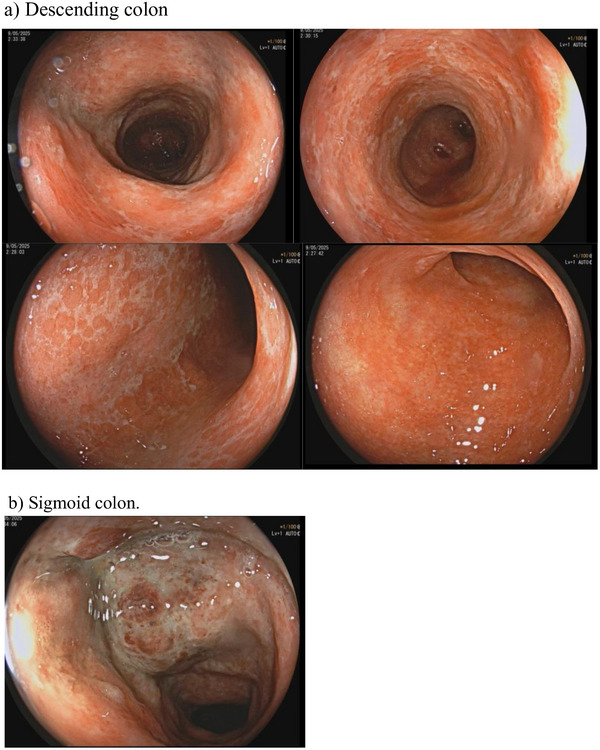 FIGURE 1
FIGURE 1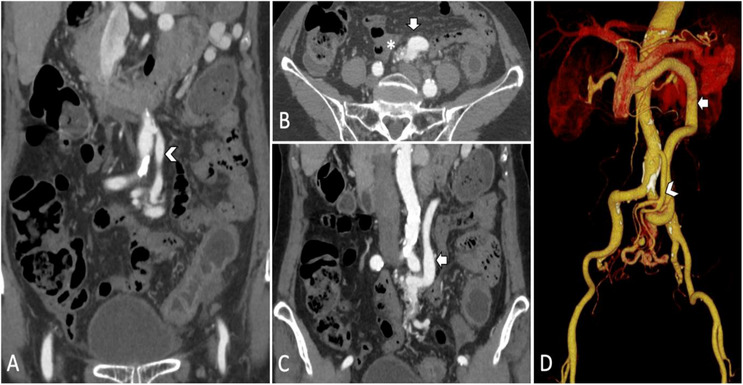 FIGURE 2
FIGURE 2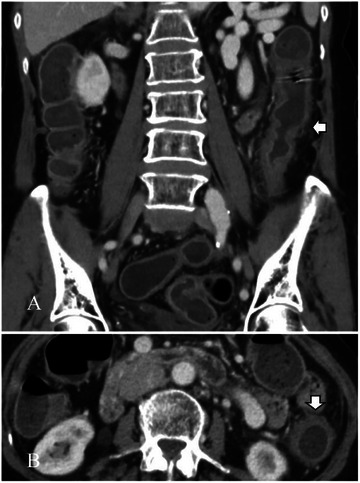 FIGURE 3
FIGURE 3| Lab test | Reference range | Unit | Result |
|---|---|---|---|
| Blood urea nitrogen | 10–20 | mg/dL | 18 |
| Creatinine | 0.55–1.02 | mL/min/1.73 m2 | 0.95 |
| Electrolytes | |||
| Sodium | 136–145 | mmol/L | 140 |
| Potassium | 3.5–5.1 | mmol/L | 3.5 |
| Chloride | 98–107 | mmol/L | 108 |
| Carbon dioxide | 22.0–29.0 | mmol/L | 22 |
| Fasting blood glucose | 74–100 | mg/dL | 110 |
| HBA1C | <6.5 | % | 5.54 |
| Lipid profile | |||
| HDL | >=60 | mg/dL | 46 |
| LDL | <130 | mg/dL | 123 |
| Triglyceride | <150 | mg/dL | 68 |
| Cholesterol | <200 | mg/dL | 178 |
| Liver function test | |||
| AST | 5–34 | U/L | 34 |
| ALT | 0–55 | U/L | 24 |
| ALP | 40–150 | U/L | 36 |
| GGT | 9–36 | U/L | 19 |
| Albumin | 34–48 | g/L | 36.5 |
| Total protein | 64–83 | g/L | 75 |
| Total bilirubin | 0.2–1.2 | mg/dL | 1.1 |
| Direct bilirubin | 0.0–0.5 | mg/dL | 0.4 |
| Coagulogram | |||
| APTT | 23.4–30.6 | sec | 25.1 |
| PT | 9.9–11.9 | sec | 12.5 |
| INR | 0.9–1.1 | 1.15 | |
| TT | 16–18.8 | sec | 16.6 |
| C‐reactive protein | < 5 | mg/L | 63.94 |
| Lactate | 0.7‐2.5 | mmol/L | 0.9 |
| Complete blood count | |||
| WBC | 4.00–10.00 | ×103/µL | 11.57 ↑ |
| RBC | 4.00–5.50 | ×106/µL | 4.00 |
| HGB | 12.00–16.00 | g/dL | 11.30 ↓ |
| HCT | 36.00–48.00 | % | 35.50 ↓ |
| MCV | 80.00–99.00 | fL | 88.6 |
| MCH | 27.0–31.0 | pg | 28.1 |
| MCHC | 33.0–37.0 | g/dL | 31.8 ↓ |
| RDW | 11.5–14.5 | % | 13.2 |
| PLT | 140.0–450.0 | ×103/µL | 130.0 ↓ |
| MPV | 7.20–11.10 | fL | 9.70 |
| Neutrophils | 40–74 | % | 73 |
| Lymphocytes | 19–48 | % | 19 |
| Monocytes | 3–9 | % | 7 |
| Eosinophils | 0–7 | % | 1 |
| Basophils | 0–2 | % | 0 |
| RBC Morphology | Normal RBC | Normal | |
|
| MRR | All Negative | |
| CMV viral load | Negative | IU/mL | <34.5 (Negative) |
| ANTI‐HIV | Negative | Negative | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Vascular Anomalies and Treatments · Gastrointestinal Bleeding Diagnosis and Treatment
Introduction
1
Ischemic colitis is the most commonly found form of gastrointestinal ischemia, accounting for 50%–60% of gastrointestinal ischemic events and comprising up to 24% of hospitalized cases of acute lower gastrointestinal bleeding [1, 2]. Its incidence ranges from 4.5 to 44 per 100,000 person‐years. It increases with age, particularly among women over 65 [2, 3]. Ischemic colitis results from transient hypoperfusion, most often in the setting of systemic hypotension, atherosclerosis, or thromboembolic disease [4]. Endoscopically, the disease appears as segmental erythema, oedema, friability, and shallow colon ulcerations, typically confined to the “watershed” areas—the splenic flexure and rectosigmoid junction [1, 5].
Most cases of ischemic colitis are non‐occlusive and resolve with supportive care, but rarely, vascular anomalies like mesenteric arteriovenous malformations (AVMs) can cause mucosal hypoxia through a steal phenomenon. AVMs of the inferior mesenteric artery–vein (IMA–IMV) axis are especially rare. Diagnosis requires a high index of suspicion and is best confirmed with computed tomography (CT) angiography. Here we present a case of ischemic colitis secondary to a mesenteric AVM.
Case Report
2
A 77‐year‐old woman with hepatitis C‐related cirrhosis (Child–Turcotte–Pugh A) presented with a two‐day history of hematochezia and mild left‐sided abdominal pain. She did not have a fever or vomiting, and she had no history of gastrointestinal bleeding before this episode. Her surgical history included a total abdominal hysterectomy for a uterine myoma 40 years earlier. She was taking carvedilol (6.25 mg twice daily) and had no family history of malignancy.
On admission, the patient's vital signs were stable and afebrile. Physical examination showed conjunctival pallor and mild left‐sided abdominal tenderness without peritonitis. No stigmata of portal hypertension or ascites were noted. Laboratory testing (Table 1) revealed leukocytosis, mild normocytic anemia, and a slightly prolonged prothrombin time, with normal liver and renal functions. Stool cultures and Clostridioides difficile toxin assays were negative.
A colonoscopy (Figure 1) performed one day post‐admission demonstrated circumferential erythema, oedema, friability, and shallow ulcerations in the descending and sigmoid colon (23–30 cm from the anal verge)—notably, the colitis extended beyond the classical watershed regions. Biopsies during colonoscopy revealed epithelial erosion and chronic active inflammation with reactive atypia. A contrast‐enhanced abdominal CT (Figures 2 and 3) done three days post‐admission revealed thickening and hypoenhancement of the descending and sigmoid colon. CT angiography identified an AVM originating from the IMA and draining into the IMV via a dilated outflow vein with a prominent vascular nidus, which was consistent with mesenteric steal physiology. This led to the diagnosis of ischemic colitis caused by a mesenteric AVM.
Findings from the colonoscopy in this case.
Findings of arteriovenous malformation from the computerized tomography of the abdomen and the computerized tomography angiogram in this case.
Findings of segmental colitis from the computerized tomography of the abdomen in this case.
The patient was initially managed with absolute bowel rest, intravenous (IV) fluids, and empiric ceftriaxone 2 g IV once daily plus metronidazole 500 mg IV every 8 h. After a multidisciplinary discussion (involving gastroenterology, vascular surgery, and interventional radiology specialists), surgical resection was selected as the treatment modality over AVM embolization due to the high risk of worsening the colonic ischemia.
An open anterior resection with AVM ligation was performed nine days post‐admission. Intraoperative colonoscopy confirmed grade 1 ischemic colitis without transmural necrosis. The operative findings included a 4.0 cm mesenteric AVM with a 0.6 cm IMA feeding vessel and a 0.8 cm IMV draining vessel. Histopathology confirmed the presence of a mesenteric AVM and associated colonic mucosal epithelial erosion and chronic active inflammation. The patient's diet was initiated at two days post‐operatively, and recovery was uneventful. There was complete resolution of abdominal pain, and no further events of gastrointestinal bleeding, and the patient was discharged one week after the successful surgery. At a 3‐month follow‐up, the patient was well and had resumed a regular oral diet without any recurrent episodes of gastrointestinal bleeding or abdominal pain.
Discussion
3
The most common causes of ischemic colitis are atherosclerosis, thromboembolism, and hypotension [1, 2]; however, the present case differed from classic cases of ischemic colitis in several ways. The patient had no significant cardiovascular comorbidities or systemic hypotension at presentation, and colonoscopy showed diffuse involvement of the descending and sigmoid colon extending beyond the typical watershed zones. In usual cases of ischemic colitis due to atherosclerotic causes, colonoscopy findings often demonstrate segmental erythema, oedema, friability, and shallow ulcerations, most often confined to watershed zones such as the splenic flexure (Griffith's point, junction of the SMA and IMA) and rectosigmoid junction (Sudeck's point, junction of the IMA and hypogastric circulation) as these are the regions with marginal perfusion [6]. However, the colonoscopy findings in this case showed circumferential erythema, oedema, friability, and shallow ulcerations in the descending and sigmoid colon (23–30 cm from the anal verge), which did not follow typical watershed zones of poor perfusion, and thus, further CT angiography was prompted to assess for abnormal lesions in the arterial supply of the left‐sided colon.
In atypical cases of ischemic colitis, it's essential to differentiate the cause from other colonic inflammations, such as infectious colitis or inflammatory bowel disease. In this case, negative stool cultures and signs of ischemic injury ruled out these causes. A CT angiography revealed an AVM involving the inferior mesenteric artery and vein, which corresponded to the ischemic colitis observed in colonoscopy and imaging. This diagnosis of AVM‐induced ischemic colitis allowed for early surgical intervention before transmural necrosis could occur.
Mesenteric AVMs are rare vascular anomalies that can cause ischemia by diverting arterial blood from mucosal capillaries. They may present with bloody diarrhea and abdominal pain, resembling ischemic colitis, but colonoscopy findings alone may not identify the underlying cause.
CT angiography is crucial for diagnosing AVM‐related ischemic colitis, as it helps visualize the AVM nidus and feeding vessels. Without early CT angiography, AVM‐related ischemic colitis might be misclassified as idiopathic or atherosclerotic, delaying treatment and increasing the risk of complications like bowel perforation and sepsis.
Managing AVM‐related ischemic colitis is case‐specific and depends on the disease severity and anatomy. Despite a high recurrence rate, conservative medical treatment can be applied in mild or pauci‐symptomatic cases as demonstrated in Lakin's case report [7]. Endovascular embolization is becoming increasingly popular as a first‐line treatment, as it is less invasive than surgery [8]. Embolization may worsen ischemia if collateral circulation is lacking. In large fistulas over 8 mm, embolization material can migrate into the portal venous system [9]. In contrast, surgical resection is the preferred treatment for large AVMs or severe ischemia, yielding better long‐term outcomes and lower recurrence rates. A review of the literature on IMA‐IMV AVF case reports [10] found that out of 45% of patients who received initial surgical management, 35% received successful embolization, 7.5% were managed conservatively, while 12.5% required combined embolization and surgery following failure of single‐modality therapy.
Surgical treatment was chosen in this case for several reasons. The AVM measured 4.0 cm, which indicated a high blood flow. This made embolization riskier due to the potential for non‐target embolization and the migration of embolic materials, particularly in fistulas larger than 8 mm in diameter. Furthermore, conservative management carried a significant risk of recurrent bleeding and ischemic episodes. These complications could lead to necrosis, perforation, and sepsis if treatment is delayed. Therefore, surgical resection combined with AVM ligation was selected to eliminate the shunt, remove non‐viable bowel tissue, and reduce the risk of recurrence and disease progression.
This case illustrates a rare presentation of ischemic colitis secondary to an inferior mesenteric AVM in a patient without conventional risk factors. Unlike typical ischemic colitis, which is often located within watershed zones, this case involved diffuse left‐sided disease caused by mesenteric steal physiology. Performing a colonoscopy and CT angiography at an early stage enabled prompt diagnosis and treatment before complications of ischemia occurred. Clinicians should maintain a high index of suspicion for AVMs in cases of atypical ischemic colitis to ensure timely, definitive treatment.
Author Contributions
Arparat Kanacharoen: conceptualization, data curation, formal analysis, and writing – original draft; Nantaporn Srivanitchapoom: visualization and writing – review & editing; Pornrujee Hirunpat: investigation, resources, and writing – review & editing; Nuttapat Tungtrongchitr: conceptualization, methodology, software, data curation, investigation, validation, formal analysis, supervision, project administration, and writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
None
Ethics Statement
The patient consented. The Human Research Ethics Committee, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, reviewed and approved this study (COA. MURA 2025/550).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. J. Brandt , P. Feuerstadt , G. F. Longstreth , et al., “ACG Clinical Guideline: Epidemiology, Risk Factors, Presentation Patterns, Diagnosis, and Management of Colon Ischemia (CI),” American Journal of Gastroenterology 110, no. 1 (2015): 18–44, 10.1038/ajg.2014.395.25559486 · doi ↗ · pubmed ↗
- 2P. D. R. Higgins , K. J. Davis , and L. Laine , “Systematic Review: The Epidemiology of Ischaemic Colitis,” Alimentary Pharmacology & Therapeutics 19, no. 7 (2004): 729–738, 10.1111/j.1365-2036.2004.01907.x.15043513 · doi ↗ · pubmed ↗
- 3S. O'Neill and S. Yalamarthi , “Systematic Review of the Management of Ischaemic Colitis,” Colorectal Disease 14, no. 11 (2012): e 751–e 763, 10.1111/j.1463-1318.2012.03171.x.22776101 · doi ↗ · pubmed ↗
- 4W. Wiesner , B. Khurana , H. Ji , et al., “CT of Acute Bowel Ischemia,” Radiology 226, no. 3 (2003): 635–650, 10.1148/radiol.2263011747.12601205 · doi ↗ · pubmed ↗
- 5D. Moszkowicz , A. Mariani , C. Trésallet , et al., “Ischemic Colitis: The AB Cs of Diagnosis and Surgical Management,” Journal of Visceral Surgery 150, no. 1 (2013): 19–28, 10.1016/j.jviscsurg.2012.12.002.23433833 · doi ↗ · pubmed ↗
- 6A. Theodoropoulou and I. E. Koutroubakis , “Ischemic Colitis: Clinical Practice in Diagnosis and Treatment,” World Journal of Gastroenterology 14, no. 48 (2008): 7302–7308, 10.3748/wjg.14.7302.19109863 PMC 2778113 · doi ↗ · pubmed ↗
- 7G. E. Lakin , T. Van Herpe , K. Van den Heede , M. van Tornout , and I. S. Gill , “Transmesenteric Arteriovenous Malformation: Case Report and Review of the Literature,” Journal of Medical Case Reports 8 (2014): 191.24928221
- 8A. Athanasiou , A. Michalinos , A. Alexandrou , S. Georgopoulos , and E. Felekouras , “Inferior Mesenteric Arteriovenous Fistula: Case Report and World‐literature Review,” World Journal of Gastroenterology 20, no. 25 (2014): 8298–8303, 10.3748/wjg.v 20.i 25.8298.25009407 PMC 4081707 · doi ↗ · pubmed ↗