Direct cholangioscopic visualization during placement of overlapping stents in malignant duodenal horizontal segment obstruction
Junzhen Li, Chumei Huang, Mufeng Ye, Yutao Zhao, Weiwen Shi, Jian Qi, Man Yang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
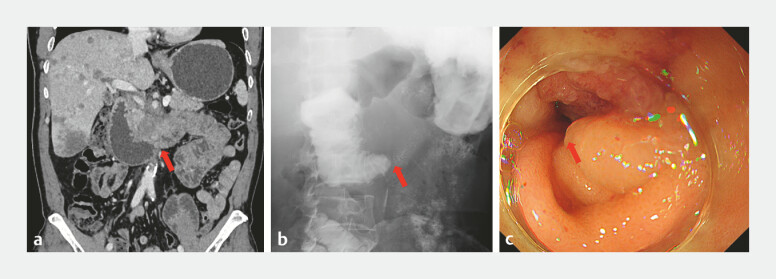 Fig. 1
Fig. 1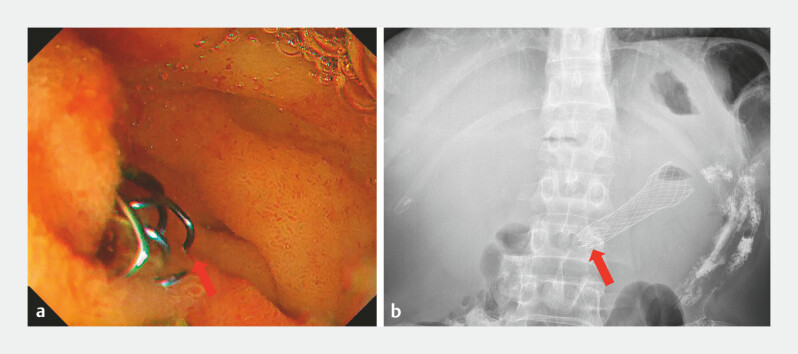 Fig. 2
Fig. 2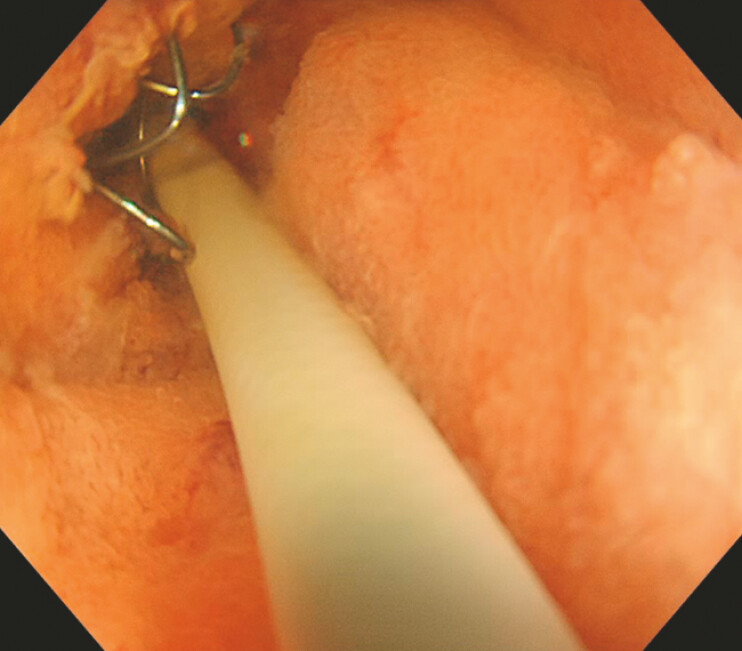 Fig. 3
Fig. 3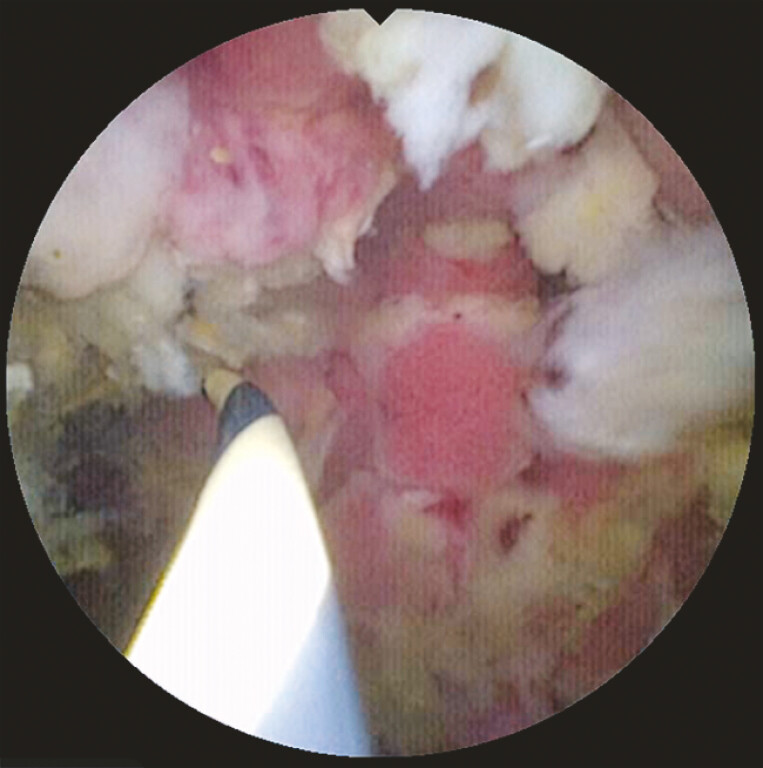 Fig. 4
Fig. 4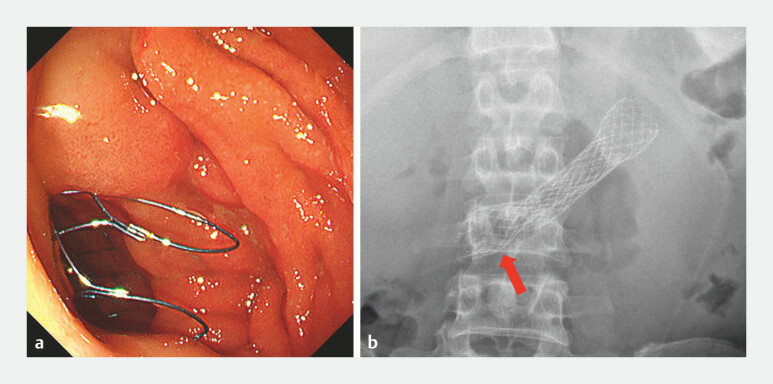 Fig. 5
Fig. 5- —The Shenzhen Clinical Research Center for Gastroenterology (Gastrointestinal Surgery)
- —The Sanming Project of Medicine in Shenzhen
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Gastrointestinal Bleeding Diagnosis and Treatment
A 51-year-old man was admitted for nausea and vomiting for 2 months. He was diagnosed with pancreatic cancer with liver, lung, and bone metastasis 3 months ago and had completed four cycles of chemotherapy. An abdominal computed tomography scan revealed pancreatic head carcinoma with duodenal involvement, indicating malignant obstruction ( Fig. 1 a ). Upper gastrointestinal series demonstrated luminal stenosis at the horizontal portion of duodenum, with dilation of the descending duodenum ( Fig. 1 b ).
Luminal stenosis at the horizontal portion of duodenum (red arrow), due to the invasion of pancreatic carcinoma. a An abdominal computed tomography scan view. b An upper gastrointestinal series view. c An endoscopy view.
Endoscopy identified a stricture at the duodenal horizontal segment ( Fig. 1 c ). A 25 × 60 mm uncovered duodenal stent was deployed across the stenotic segment ( Fig. 2 a ). An abdominal X-ray showed that the proximal end of the stent failed to achieve well expansion due to its deep deployment and the angulation at the duodenal horizontal segment ( Fig. 2 b ), with retained food contents in the dilated stomach and descending duodenum. An ultrathin endoscope could not be advanced through the stent due to the angulation at the duodenal horizontal segment.
The proximal end of the stent (red arrow) failed to achieve complete expansion. a An endoscopy view and b an abdominal X-ray view.
A cholangioscope was inserted through the stent ( Fig. 3 ). Under direct visualization, a guidewire was passed through the lumen of the stent, not through the stent mesh, and successfully advanced into the distal duodenum ( Fig. 4 , Video 1 ). A second 25 × 60 mm uncovered stent was successfully placed overlapping the first stent under the guidance of the guidewire ( Fig. 5 a ). An abdominal X-ray confirmed the complete expansion of the proximal end of the second stent ( Fig. 5 b ). The patient was able to eat semi-liquid foods without vomiting.
A cholangioscope was inserted through the stent.
Under direct visualization, a guidewire was passed through the lumen of the stent and advanced into the distal duodenum.
A novel cholangioscopic approach to overlapping stent placement in malignant duodenal horizontal segment obstruction.Video 1
Well expansion of the proximal end of the second stent (red arrow), successfully overlapping the first stent. a An endoscopy view and b an abdominal X-ray view.
To the best of our knowledge, this case represents the first successful attempt for direct cholangioscopic visualization without X-ray assisted during the placement of overlapping stents in malignant duodenal obstruction. The use of a cholangioscope for intraluminal visualization in technically challenging stent placement plays a crucial role by allowing for precise, radiation-free and safe deployment of overlapping stents.
Endoscopy_UCTN_Code_TTT_1AO_2AZ