Successful complete closure of anastomotic leak in ileal pouch anal anastomosis with endoscopic helix tacking device
Eleni Nakou, Panagiotis Dikeakos, Marianna Spinou, Dimitrios Dimitriadis, Petros Zormpas, Margarita-Eleni Manola, George Tribonias

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
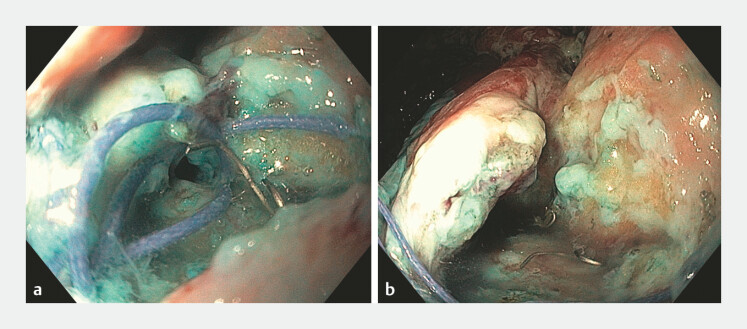 Fig. 1
Fig. 1 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Stoma care and complications · Colorectal Cancer Surgical Treatments
Anastomotic leaks remain a serious complication after ileal pouch–anal anastomosis (IPAA), ranging from acute events to chronic leaks leading to pouch dysfunction or failure 1 . Although traditionally managed surgically, minimally invasive endoscopic approaches are increasingly used, with variable success rates 1 2 .
We report the first successful endoscopic closure of an anastomotic leak using a suturing device after ileoanal pouch construction.
A 53-year-old man with ulcerative colitis and prior laparoscopic subtotal colectomy was admitted for ileoanal pouch construction. The procedure included end ileostomy takedown, extensive adhesiolysis, transabdominal and transanal rectal stump excision, construction of a 16-cm ileoanal pouch and creation of a protective loop ileostomy.
On the 5th postoperative day, the patient developed fever and purulent output from the surgical drain. Computed tomography demonstrated an anastomotic leak and exploratory laparotomy was performed identifying the site of rupture in the IPAA. Thorough lavage of the peritoneal cavity was performed and surgical drains were placed in all abdominal compartments.
The patient demonstrated no signs of peritonitis and conservative management was chosen. On the 12th postoperative day, the patient was referred to the gastroenterology department for the endoscopic management of the leak. During endoscopy, a leak of approximately 20 mm in diameter was identified near the dentate line at the anal–pouch anastomosis ( Fig. 1 a, b ). Endoscopic complete closure with a helix tacking device (X-Tack, Boston Scientific) was performed successfully ( Video 1 ).
a A close-up endoscopic view of a 20-mm anastomotic leak at the pouch–anal anastomosis. b A wide-field endoscopic view of a 20-mm anastomotic leak at the pouch–anal anastomosis.
Endoscopic management of an IPAA anastomotic leak. The video demonstrates the identification of the defect and complete closure using the helix tacking device (X-Tack), followed by surveillance endoscopy at 4 and 12 months. IPAA, ileal pouch–anal anastomosis.Video 1
The drain output decreased and the patient was discharged in good condition. Follow-up endoscopy at 4, 12 and 18 months demonstrated complete mucosal healing ( Fig. 2 a, b ) with the X-Tack device in situ ( Fig. 2 c ). The patient remained asymptomatic through the 18-month follow-up and it was decided to proceed with takedown of the loop ileostomy.
a A wide-field endoscopic view demonstrating complete mucosal healing at an 18-month follow-up. b A close-up endoscopic view of the healed mucosa at an 18-month follow-up. c An X-Tack device in situ at an 18-month follow-up.
Endoscopic suturing devices offer a promising minimally invasive option for managing postoperative complications after IPAA, potentially reducing morbidity and reoperation challenges.
Endoscopy_UCTN_Code_CPL_1AJ_2AJ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Huang AL Plietz M Greenstein AJ Management of Anastomotic Leaks in Ileal Pouch Anal Anastomosis for Ulcerative Colitis Clin Colon Rectal Surg 20223546947410.1055/s-0042-175813836591405 PMC 9797281 · doi ↗ · pubmed ↗
- 2ForcignanòE Verra M Lo Secco G Endoscopic Management of Anastomotic Insufficiencies in the Lower GI Tract Visc Med 2025 Online ahead of print 10.1159/000547021 PMC 1227407040688737 · doi ↗ · pubmed ↗