Peroral cholangioscopic diagnosis of refractory hemobilia caused by pancreatic arteriovenous malformation: a case report
Min Xu, Yingying Li, Yanru Li, Yuwei Wang, Shuyi Zhang, Wen Li, Hao Zhang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
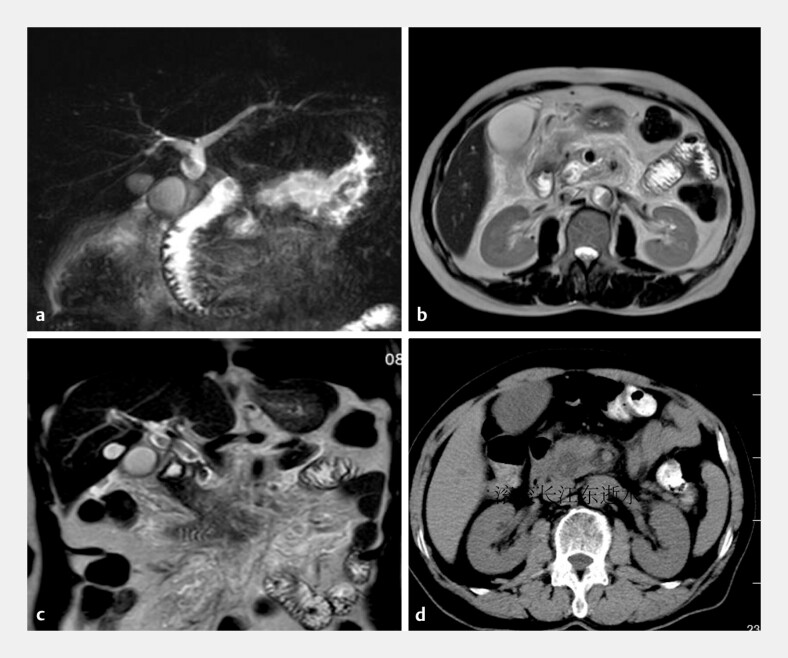 Fig. 1
Fig. 1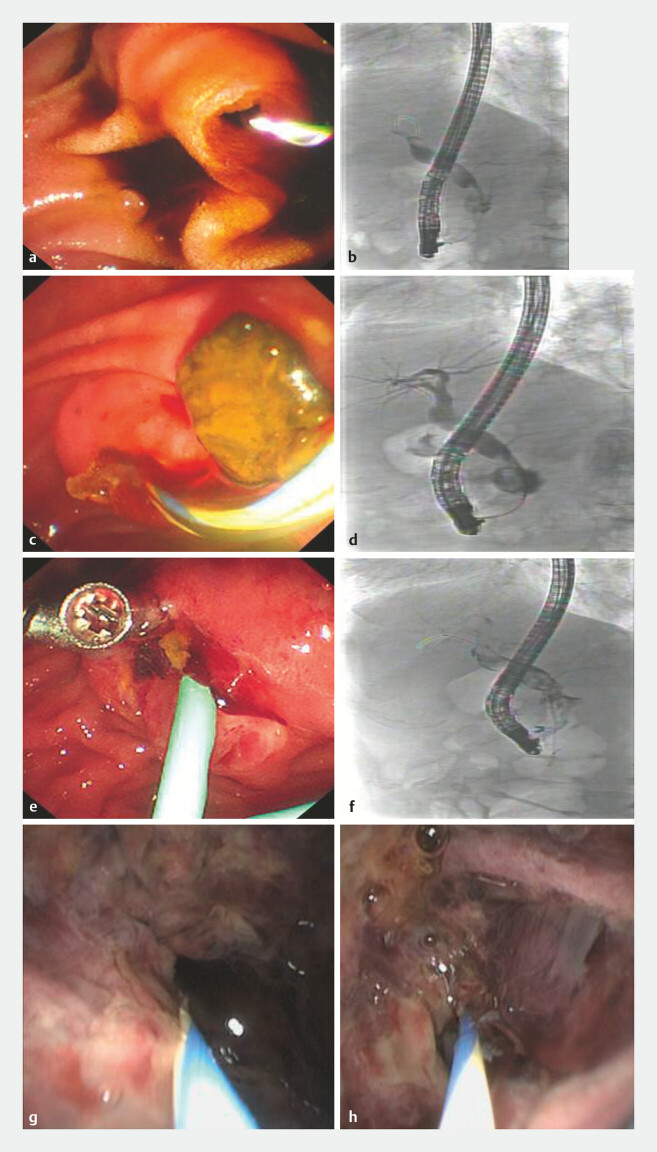 Fig. 2
Fig. 2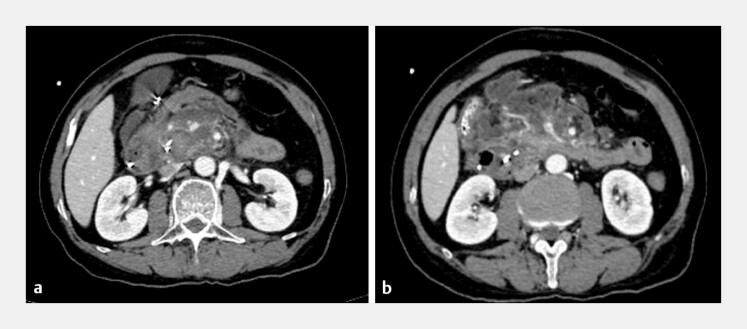 Fig. 3
Fig. 3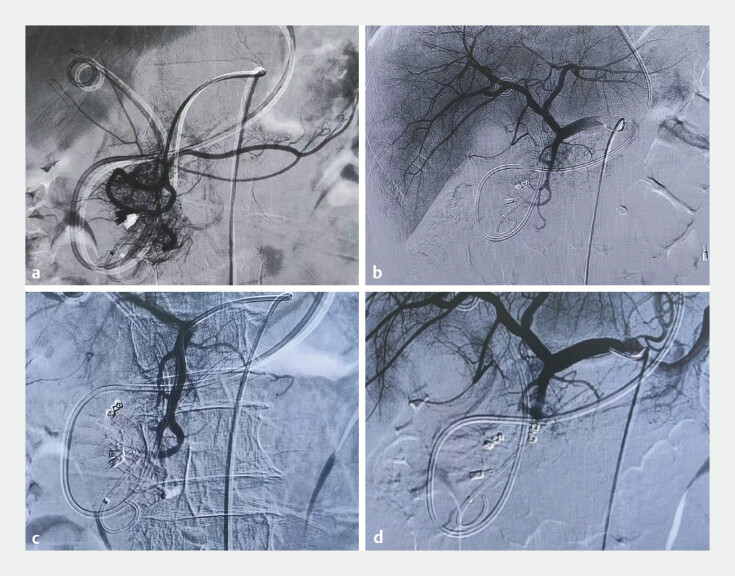 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Pancreatitis Pathology and Treatment · Gallbladder and Bile Duct Disorders
Pancreatic arteriovenous malformation is a rare vascular anomaly. The first reported case was described in 1968 by Halpern et al. 1 . Yang Zhuo et al. reported a case of failed treatment of biliary hemorrhage caused by a gastroduodenal artery malformation with fully covered biliary metal stents 2 . In this case, the patient was admitted due to “common bile duct stones” and experienced hemobilia after endoscopic retrograde cholangiopancreatography (ERCP). Peroral cholangioscopy revealed bleeding from a cystic lesion in the pancreatic portion of the common bile duct.
A 67-year-old man was admitted to our hospital with upper abdominal pain. Magnetic resonance cholangiopancreatography showed an abnormal signal intensity in the pancreatic head, common bile duct stones and pancreatitis ( Fig. 1 ). The patient underwent ERCP to remove the stone ( Fig. 2 a–d ). The patient developed abdominal pain, blood in the nasobiliary drainage, and melena after ERCP. No active bleeding was observed at the endoscopic sphincterotomy incision margin ( Fig. 2 e–f ). Peroral cholangioscopy revealed a cystic dilation of the distal common bile duct. Within the cyst, the normal bile duct wall architecture was absent, and tortuous, dilated vessels along with a hematoma were observed ( Fig. 2 g–h ). The cholangioscopic findings suggested bleeding from a vascular malformation ( Video 1 ).
a, b MRCP revealing cystic dilation of the pancreatic segment of the common bile duct. c MRCP reveals a hypointense focus within the common bile duct. d Abdominal CT revealing dilation of the pancreatic segment containing hyperdensity. CT, computed tomography; MRCP, magnetic resonance cholangiopancreatography
The first ERCP: a hemobilia from the orifice of Vater’s ampulla before cannulation. b ERCP reveals dilation of the extrahepatic bile duct within stones and cystic dilation of the pancreatic segment of the common bile duct. c Bloody bile drainage is observed after stone removal. d Fluoroscopy reveals a blood clot within the cystic dilation. e No active bleeding was observed at the EST incision margin. The second ERCP: f fluoroscopy reveals a blood clot within the cystic dilation. g, h Peroral cholangioscopy revealed a cystic dilation of the distal common bile duct. Within the cyst, the normal bile duct wall architecture was absent, and tortuous, dilated vessels along with a hematoma were observed. ERCP, endoscopic retrograde cholangiopancreatography; EST, endoscopic sphincterotomy.
Peroral cholangioscopy shows a cystic dilation in the distal common bile duct with a hematoma. During DSA, the pancreatic head region exhibits dense vascularity, accompanied by rapid visualization of the portal vein. DSA, digital subtraction angiography.Video 1
During digital subtraction angiography (DSA), angiographic findings were considered typical of an arteriovenous malformation in the pancreaticobiliary region ( Fig. 3 a ). After the superior pancreatoduodenal artery was embolized, post-embolization angiography confirmed the disappearance of the vascular cluster and the fistula ( Fig. 3 b , Video 1 ). Subsequently, the hemobilia occurred again. An abdominal contrast-enhanced computed tomographic scan showed that the surgical intervention was not feasible ( Fig. 4 a, b ). A repeat DSA was performed, and the superior pancreaticoduodenal artery was embolized using coils ( Fig. 4 c, d ). No further bleeding occurred following this procedure. The nasobiliary tube was removed 7 days later. Unfortunately, the patient died due to a cardiocerebrovascular accident.
Enhanced computed tomography reveals multiple hypervascular spots in the pancreatic head and early visualization of the portal vein and superior mesenteric vein.
The first DSA: a GDA angiography: the pancreatic head region exhibits dense vascularity, accompanied by rapid visualization of the portal vein. b The arterioportal fistula vanished subsequent to the gelatin sponge embolization of the superior pancreaticoduodenal artery. The second DSA: c Angiography of the common hepatic artery still demonstrates blood supply to the pancreatic head region via the superior pancreaticoduodenal artery and d followed by coil embolization of the superior pancreaticoduodenal artery. DSA, digital subtraction angiography; GDA, gastroduodenal artery.
Endoscopy_UCTN_Code_CCL_1AZ_2AN
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Halpern M Turner AF Citron BP Hereditary hemorrhagic telangiectasia. An angiographic study of abdominal visceral angiodysplasias associated with gastrointestinal hemorrhage Radiology 1968901143114910.1148/90.6.11435656734 · doi ↗ · pubmed ↗
- 2Han K Zhao Q Sun Y Direct peroral cholangioscopic diagnosis and metal stent failure in a case of refractory arterial hemobilia Endoscopy 20255701 E 1096 E 109710.1055/a-2686-341440983102 PMC 12453878 · doi ↗ · pubmed ↗