Hybrid endoscopic rescue following endoscopic ultrasound-guided choledochoduodenostomy
Miguel Martins, Joana Mota, Filipe Vilas-Boas, Joel Ferreira-Silva, Eduardo Rodrigues-Pinto, Guilherme Macedo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
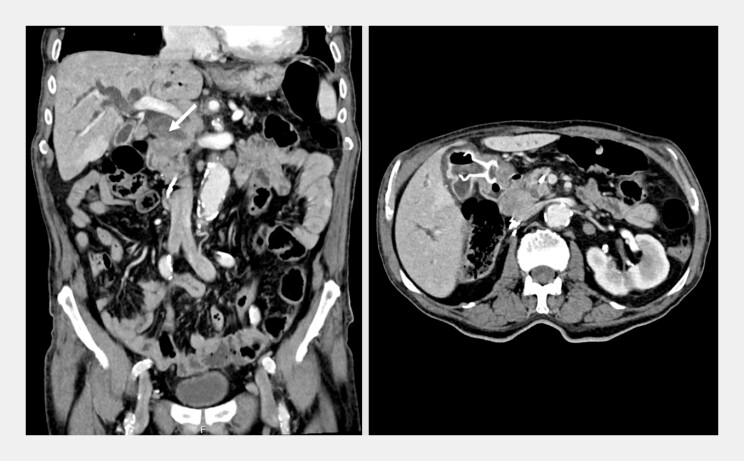 Fig. 1
Fig. 1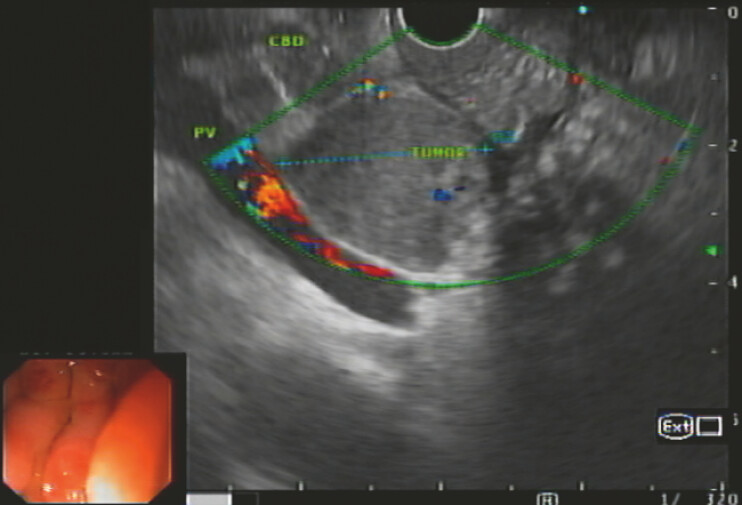 Fig. 2
Fig. 2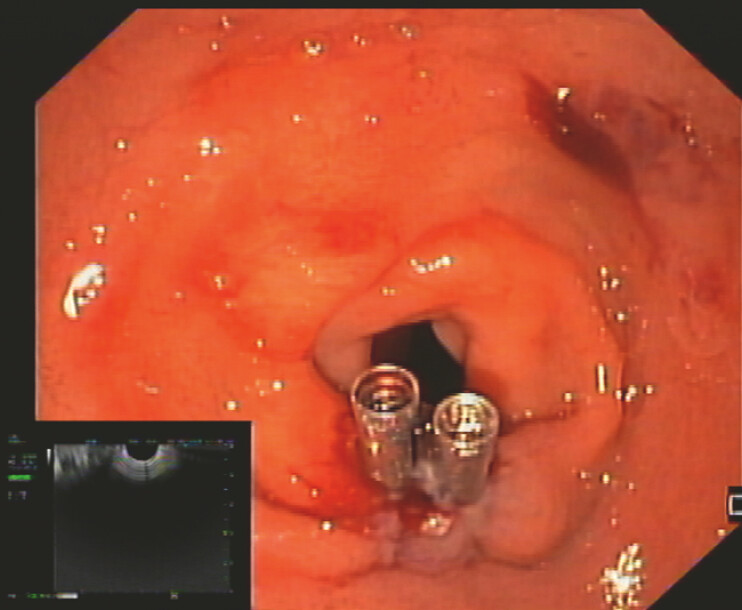 Fig. 3
Fig. 3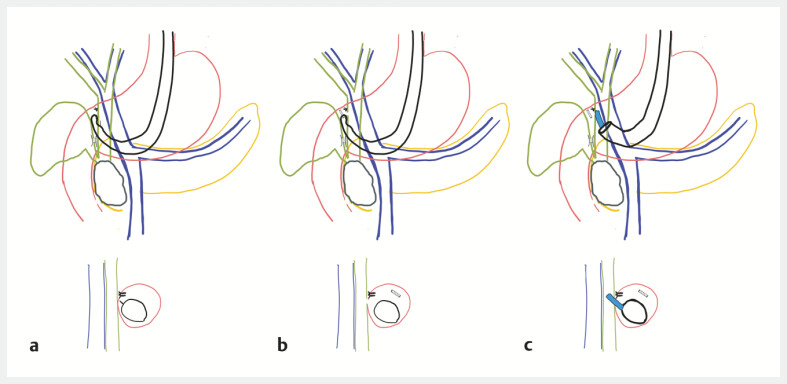 Fig. 4
Fig. 4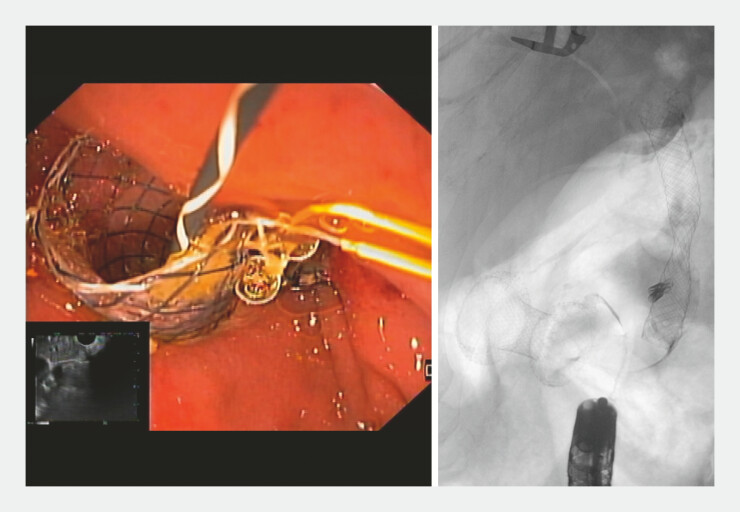 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Minimally Invasive Surgical Techniques · Esophageal and GI Pathology
An 88-year-old man with biliary obstruction caused by a complex cystic lesion in the pancreatic head, considered inoperable due to significant comorbidities, was referred for endoscopic biliary drainage. Following failed endoscopic retrograde cholangiopancreatography, endoscopic ultrasound (EUS)-guided cholecystogastrostomy was performed, as the cystic duct was patent. Two years later, he presented with cholangitis from recurrent biliary obstruction due to disease progression ( Fig. 1 ). EUS revealed common bile duct (CBD) dilation (~14 mm), caused by the pancreatic head lesion ( Fig. 2 ). Left intrahepatic bile duct dilation was minimal, precluding hepaticogastrostomy. Decision was to perform EUS-guided choledochoduodenostomy.
A CT scan showing biliary obstruction caused by a mass in the pancreatic head, with a previously placed cholecystogastrostomy lumen-apposing metal stent (LAMS) in situ. CT, computed tomography.
An endoscopic ultrasound image showing common bile duct (CBD) dilation caused by the pancreatic head lesion.
The first attempt with a 6 × 8 mm electrocautery-tip lumen-apposing metal stent (Axios, Boston Scientific) using the free-hand technique resulted in a type I misdeployment 1 . The stent was removed, and the duodenal wall defect was closed with two through-the-scope clips ( Fig. 3 ). The second attempt involved CBD puncture using a 19G needle (Expect Slimline, Boston Scientific) for cholangiography and duct distension, fistula creation using an 8.5 Fr cystotome (Cysto-Gastro-Set, Endo-Flex), and the placement of the 10 × 60 mm fully covered metal biliary stent (Evolution, Cook Medical); however, the stent migrated distally during deployment ( Fig. 4 ). Despite multiple attempts, CBD re-canulation using guidewire manipulation was not achieved. Using a therapeutic endoscope (Olympus GIF-2TH180), a cholangioscope (SpyGlass DS II, Boston Scientific) was advanced through the fistula into retroperitoneal space, enabling access to the bile duct and stent placement over a guidewire ( Video 1 ). Final endoscopic and fluoroscopic imaging confirmed pneumobilia and adequate bile/contrast drainage ( Fig. 5 ). Patient recovered rapidly, being discharged on post-procedure day 3.
An endoscopic view of the duodenal bulb showing the closure of the wall defect resulting from the initial drainage attempt complicated by type 1 lumen-apposing metal stent (LAMS) misdeployment.
Schematic representation of procedural adverse events and their management: a Duodenal wall defect closure after lumen-apposing metal stent (LAMS) misdeployment. b Stent migration during the second attempt, resulting in biliary and duodenal defects. c The hybrid endoscopic rescue procedure using cholangioscopy for recannulation of the biliary fistula and stent repositioning.
Final endoscopic and fluoroscopic images demonstrating successful biliary drainage.
Cholangioscopy-assisted recannulation of the biliary fistula after stent migration, enabling guidewire reposition and deployment of a fully covered metal stent to restore effective biliary drainage.Video 1
EUS-guided biliary drainage is an effective alternative when transpapillary drainage is not feasible, although adverse events can be significant 2 . To our knowledge, the use of cholangioscopy for biliary fistula salvage after EUS-choledochoduodenostomy has not been previously reported 3 . This hybrid NOTES-based approach may represent a valuable rescue option in such cases.
Endoscopy_UCTN_Code_CPL_1AL_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen YI Long C Sahai AV Stent misdeployment and factors associated with failure in endoscopic ultrasound-guided choledochoduodenostomy: analysis of the combined datasets from two randomized trials Endoscopy 20255733033839505002 10.1055/a-2463-1601 · doi ↗ · pubmed ↗
- 2Gopakumar H Singh RR Revanur V Endoscopic Ultrasound-Guided vs Endoscopic Retrograde Cholangiopancreatography-Guided Biliary Drainage as Primary Approach to Malignant Distal Biliary Obstruction: A Systematic Review and Meta-Analysis of Randomized Controlled Trials Am J Gastroenterol 20241191607161510.14309/ajg.000000000000273638421018 · doi ↗ · pubmed ↗
- 3Vanella G Bronswijk M Dell’Anna G Classification, risk factors, and management of lumen apposing metal stent dysfunction during follow-up of endoscopic ultrasound-guided choledochoduodenostomy: Multicenter evaluation from the Leuven-Amsterdam-Milan Study Group Dig Endosc 20233537738836177532 10.1111/den.14445 PMC 12136247 · doi ↗ · pubmed ↗