Intralesional Corticosteroid Therapy for Isolated Immunoglobulin G4-Related Esophageal Involvement: A Novel Approach to a Rare Condition
Balkeess Alhanaktah, Emad Chishti, Nathan R. Shelman, Bahaaeldeen Ismail

TL;DR
A novel treatment combining intralesional steroids and balloon dilation successfully managed a rare case of immunoglobulin G4-related esophageal disease.
Contribution
This paper introduces a new treatment approach for immunoglobulin G4-related esophageal disease using intralesional steroids.
Findings
The patient showed prolonged clinical stability with the novel treatment approach.
Systemic and topical steroids were poorly tolerated by the patient.
Combining intralesional steroids with serial balloon dilation proved effective for managing the condition.
Abstract
Immunoglobulin G4-related disease is a chronic, systemic immune-mediated condition. Esophageal involvement is considered rare and often poses major diagnostic and therapeutic challenges. We present an 81-year-old male patient with isolated esophageal immunoglobulin G4-related disease with extended clinical and endoscopic follow-up for 6 years, who had poor tolerance to systemic and topical steroids. The patient was successfully treated using a combination of intralesional steroids and serial balloon dilations spaced at long intervals. This approach, which has not been previously reported in this condition, resulted in prolonged clinical stability over an extended period.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1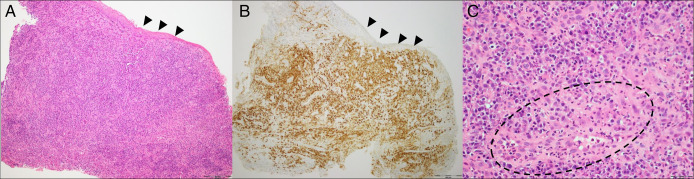 Figure 2
Figure 2| Study | Age | Sex | Presenting symptoms and duration before diagnosis | Pattern of esophageal involvement | Location of the esophageal lesion | Serum IgG4 levels | Involvement of other organs | Medical treatments used (in order) | Endoscopic treatments used (in order) | Surgical interventions | Outcome | Estimated follow-up duration |
| Dumas-Campagna et al, | 63 | Female | Progressive odynophagia, dysphagia and weight loss (10 yr) | Circumferential ulcerative esophagitis with stenosis and dissecans superficialis appearance | Three distinct stenoses throughout the esophagus | NA. | None | Prednisone; oral mercaptopurine; oral mycophenolate mofetil; oral cyclosporine; infliximab; adalimumab; rituximab | None | None | Minimal response to prednisolone and rituximab but no significant improvement with other modalities | 3 yr |
| Oh et al, | 33 | Male | Progressive dysphagia and weight loss (1 yr) | Stricture and neck mass surrounding the lower cervical esophagus | Cervical esophagus just below the UES | Elevated | Isolated | Prednisolone (40 mg/d tapering by 10 mg/2 wk, then maintenance 5 mg/d) | None | None | Improved (able to tolerate solids) | 11 mo |
| Yang et al, | 60 | Male | Occasional acid reflux (workup was initiated because of esophageal masses on imaging) | Hard, fixed mass, normal overlying mucosa | Lower esophagus | Elevated | Stomach (ulcer) and liver (masses) | Steroids (no further details) | None | None | Stationary 3 mo after steroids (neither regression nor progression of the esophageal mass) | 3 mo |
| Obiorah et al, | 63 | Male | Dysphagia (20 yr) | Achalasia-like (distal esophagus dilation), along with esophagitis | Distal esophagus | NA. | None | Steroids (no further details) | None | Botox (for suspected achalasia) | Stationary | NA. |
| 47 | Male | Dysphagia (6 yr) | Stricture with friable mucosa | NA. | Normal | None | Prednisolone initiated (0.6–1 mg/kg daily) then tapered and use maintenance mycophenolate mefotil | Multiple endoscopic dilations (before diagnosis) | None | Improved after prednisolone and mycophenolate mefotil | NA. | |
| 79 | Female | Dysphagia (14 yr) | Stricture with friable mucosa | NA. | Normal | None | Steroids (no further details), then mycophenolate mefotil | Multiple endoscopic dilations | None | Improved after prednisolone and mycophenolate mefotil | NA. | |
| Sharma et al, | 18 | Male | Dysphagia and weight loss (2 yr) | Stricture | Distal 7–8 cm | Elevated | None | Steroids (no further details) | Endoscopic dilation once | Esophagectomy | Uneventful postoperative period | NA. |
| Jang et al, | 56 | Male | Dysphagia to solids and weight loss (for 3 yr) | Stricture and mucosal abrasion | At 32 cm (from incisors) | Normal | None | Prednisolone (30 mg slow taper | None | Ivor-Lewis esophagectomy (patient preferred more definitive therapy) | Uneventful postoperative course and improved after prednisolone | 11 mo |
| Kaneshiro et al, | 87 | Female | Dysphagia to solids (1 yr) | Stricture | At 27 cm (from incisors) | NA. | None | Swallowed fluticasone inhaler | Twelve endoscopic dilations | None | Minimal symptomatic relief, but inflammation worsened on following biopsy (3 mo after fluticasone) | 24 mo |
| 65 | Male | Dysphagia to solids and liquids and odynophagia | Diffuse narrowing with dissecans superficialis appearance. Then new focal stricture on follow up | Focal stricture at 20 cm (from incisors) | NA. | None | Oral | None | Esophago-gastrectomy (for eventual diagnosis of squamous cell carcinoma, proximal esophagus) | No response, after 6 mo of steroids | 6 mo | |
| Poole et al, | 47 | Male | Impacted food bolus obstruction, progressive dysphagia and weight loss (6 mo) | Firm impassable stricture with mild inflammation | Stricture at 30 cm (from incisors) and circumferential narrowing from 30 cm to GEJ. | Elevated | None | Intravenous | Endoscopic dilation to 14 mm | VATS core biopsy (because of hypoechoic esophageal wall thickening) | Symptomatic improvement; recurrence upon weaning prednisolone; sustained improvement on azathioprine monotherapy | 2.5 yr |
| Correia et al, | 30 | Female | Dysphagia and odynophagia (yr) | Fibrous ring/membrane | Proximal esophagus | Normal | None | Topical fluticasone | Endoscopic dilation twice (complicated by perforation) | None | No significant improvement after 8 wk of fluticasone | 10 mo |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Autoimmune Bullous Skin Diseases · Vasculitis and related conditions
INTRODUCTION
Immunoglobulin G4-related disease (IgG4-RD) is a chronic fibroinflammatory condition mediated by a dysregulated immune response involving lymphocytes and plasma cells eventually leading to fibrosis.^1^ Characteristic histology includes IgG4-rich lymphoplasmacytic infiltrate, storiform fibrosis, and obliterative phlebitis.^2^
The pancreato-hepatobiliary tract is the most commonly involved region in gastrointestinal IgG4-RD, whereas luminal gastrointestinal involvement is rare. More than 20 esophageal IgG4-RD cases are reported, and while presentation and diagnosis are described, treatment approaches and disease course remain unclear, largely because of the limited follow-up time in the available cases. We report a case of esophageal IgG4-RD with six-year follow-up, successfully managed with multiple therapies, including the novel use of intralesional steroids.
CASE REPORT
An 81-year-old man presented with progressive dysphagia to solids and regurgitation over 2–3 years, worsening rapidly in the 6 months before his referral. Medical history included hypertension and type 2 diabetes. He denied smoking or alcohol use. A modified barium swallow showed cervical osteophytes without functional impact. Laboratory results showed normal blood counts and metabolic panel.
He then underwent his first esophagogastroduodenoscopy (EGD) that revealed a 6 mm × 1 cm inflamed stricture at the gastroesophageal junction, with no other abnormalities (Figure 1). Dilation was deferred because of inflammation, and omeprazole 40 mg was increased to twice daily for suspected gastroesophageal reflux disease. The stricture biopsies revealed >100 IgG4-positive plasma cells per high-power field and a 40% IgG4-to-total plasma cell ratio, suggesting IgG4-RD (Figure 2), despite normal serum IgG4 and negative antinuclear antibody. Chest computed tomography and magnetic resonance cholangiopancreatography showed no evidence of IgG4-RD in other organs.
Endoscopic appearance of the stricture at initial presentation a 6 mm × 1 cm inflamed stricture at the gastroesophageal junction, with no other mucosal or intraluminal findings noted throughout the esophagus (A). (B) After serial endoscopic dilation alone at 9 months, (C) after serial endoscopic dilation with intralesional steroid injection at 19 months, and (D) most recent esophagogastroduodenoscopy five years from initial presentation.
Histopathological findings from stricture biopsy at time of diagnosis. (A) Squamous mucosa [black arrowheads] undermined by dense infiltrate of plasma cells, with stromal sclerotic change (H&E, 100×). (B) Squamous mucosa [black arrowheads] undermined by dense infiltrate of plasma cells [IgG4 positive, brown chromagen], with stromal sclerotic change (IgG4 IHC, 100×). (C) High power field [1 HPF] demonstrating infiltration of plasma cells and area of early sclerotic change (interrupted line) with associated small vessel (asterisk) (H&E, 400×). H&E, hematoxylin and eosin; IgG4, immunoglobulin G4; IHC, immunohistochemistry.
Four weeks later, EGD was repeated showing persistent inflammatory stricturing and underwent through-the-scope balloon dilation to 8 mm. Serial dilation every 1–2 weeks was advised to reach 15–18 mm, but the patient opted for less frequent sessions. Two months later, EGD showed persistent 8 mm stricture that was dilated to 12 mm. Oral prednisone 40 mg daily was initiated then and tapered over 3 months, which was associated with worsening hypertension and hyperglycemia. Six months later, the stricture regressed to 8 mm and was dilated to 11 mm with a 40 mg triamcinolone injection. A trial of compounded viscous budesonide (2 mg BID) was started but discontinued after 2 months because of lack of improvement and patient's concerns about side effects. Over the next 10 months, he underwent 3 additional EGDs with serial dilations and triamcinolone injections, eventually reaching 15 mm despite 4–5-month intervals.
He was subsequently monitored clinically, satisfied with his swallowing, and declined further EGDs. He remained asymptomatic until dysphagia reoccurred after 4 years. EGD revealed a 9 mm stricture (Figure 1), dilated to 13.5 mm with triamcinolone injection. He remains well under clinical follow-up.
DISCUSSION
Although esophageal IgG4-RD has been reported, its natural history and treatment lines remain unclear. It is often omitted from expert reviews on immune-mediated esophageal conditions and strictures, highlighting the need for enhancing clinicians' awareness of this rare but treatable disorder.^3^
The typical presentation is progressive solid food dysphagia and variable-length inflammatory stricturing, as seen in our case. Esophageal involvement may also manifest as pseudotumors or mimic achalasia or esophagitis dissecans superficialis.^4–6^ Our patient exhibited a localized gastroesophageal junction stricture, with characteristic histopathology of dense lymphoplasmacytic infiltrates and an IgG4-to-IgG plasma cell ratio exceeding the reported cut-off of 40%–50%.^7^ Demographically, our case aligns with the literature, which shows a male predominance and peak incidence above age 50.^8^ Notably, only 2 cases have been documented in patients older than 80 years, matching our patient's age.^9^ While a few cases have demonstrated gastric, hepatic, or pulmonary involvement, our patient had no extra-esophageal disease and had normal serum IgG4 levels.^10,11^
Treatment options previously included surgery when malignancy or achalasia were suspected.^8,12^ This is generally unnecessary once this benign condition is correctly identified. Most cases report a combination of endoscopic dilation and medical therapy.^13,14^ Medical management as summarized in (Table 1) is largely extrapolated from other IgG4-RD, particularly autoimmune pancreatitis, where systemic corticosteroids are first-line.^4^ While effective in some, long-term steroid use is limited by side effects, as in our patient. Steroid-sparing agents such as rituximab and mycophenolate mofetil have shown partial benefit in isolated reports, but were not used in our patient because of limited evidence and patient's adverse events concerns.^6,8^
Unlike pancreatic disease, luminal involvement is endoscopically accessible, enabling intralesional therapy. A similar approach has been applied in periorbital IgG4-RD, where local steroid injections proved effective.^18^ Several studies, including randomized trials, have shown that intralesional steroid injections during dilation prolong intervals between sessions in benign esophageal strictures, with a favorable safety profile.^3,19^ Though not previously reported in esophageal IgG4-RD, we found this a rational option to our patient given the immune-mediated disease nature and his localized stricturing. He tolerated repeated triamcinolone injections without adverse effects and experienced clinical and endoscopic improvement despite infrequent dilation sessions.
The disease's natural history remains poorly defined due to limited follow-up in most reports. Only 6 published cases included follow-up beyond 1 year after diagnosis, among them, 2 were followed after complete endoscopic or surgical disease resection, neither requiring further treatment.^5,20^ The others received medical therapies with mixed outcomes: one responded adequately and transitioned from corticosteroids to azathioprine monotherapy, while the others showed limited response (one to swallowed fluticasone, the other to various immunosuppressants).^6,9,14^ Our patient was followed clinically and endoscopically for 6 years, representing the longest follow-up duration reported to our knowledge. Notably, 4 of those years were without medical or endoscopic intervention, during which he experienced an unexpected slow symptoms progression. This variability may reflect disease behavior heterogeneity, with individual factors such as diet and symptom perception possibly contributing.^21^
Esophageal IgG4-RD should be considered in benign strictures, even without extra-esophageal involvement. Biopsies and appropriate staining are essential, especially with plasma cell infiltrates. Intralesional steroids appear safe and potentially effective. A watch-and-wait approach seems reasonable in those with indolent off-treatment course.
DISCLOSURES
Author contributions: B. Alhanaktah and B. Ismail led the conception and design of the manuscript. Clinical data collection was performed by E. Chishti and NR Shelman. B. Alhanaktah and B. Ismail wrote the first draft of the manuscript, and all authors provided comments on this version. All authors read and approved the final manuscript. B. Ismail is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stone JH. Ig G 4-related disease: Lessons from the first 20 years. Rheumatology. 2025;64(Supplement_1):i 24–7.40071397 10.1093/rheumatology/keaf 008 · doi ↗ · pubmed ↗
- 2Katz G Stone JH. Clinical perspectives on Ig G 4-related disease and its classification. Annu Rev Med. 2022;73(1):545–62.34669430 10.1146/annurev-med-050219-034449 · doi ↗ · pubmed ↗
- 3Thanawala SU Lynch KL. Management of esophageal strictures. Gastrointest Endosc Clin N Am. 2025;35(3):623–36.40412994 10.1016/j.giec.2025.02.002 · doi ↗ · pubmed ↗
- 4Wallace ZS Katz G Hernandez-Barco YG Baker MC. Current and future advances in practice: Ig G 4-related disease. Rheumatol Adv Pract. 2024;8(2):rkae 020.38601138 10.1093/rap/rkae 020PMC 11003820 · doi ↗ · pubmed ↗
- 5Ekinci N Unal Kocabey D Gun E Aslan F. Giant Ig G 4-related pseudotumor of the esophagus resected with endoscopic submucosal dissection: A case report and review of the literature. Turk Patoloji Derg. 2021;37(3):258–63.33432560 10.5146/tjpath.2020.01515 PMC 10510622 · doi ↗ · pubmed ↗
- 6Dumas-Campagna M Bouchard S Soucy G Bouin M. Ig G 4-related esophageal disease presenting as esophagitis dissecans superficialis with chronic strictures. J Clin Med Res. 2014;6(4):295–8.24883156 10.14740/jocmr 1845 w PMC 4039102 · doi ↗ · pubmed ↗
- 7Dominguez‐Muñoz JE Vujasinovic M de la Iglesia D European guidelines for the diagnosis and treatment of pancreatic exocrine insufficiency: UEG, EPC, EDS, ESPEN, ESPGHAN, ESDO, and ESPCG evidence‐based recommendations. United Eur Gastroenterol J. 2025;13(1):125–72.10.1002/ueg 2.12674 PMC 1186632239639485 · doi ↗ · pubmed ↗
- 8Obiorah I Hussain A Palese C Azumi N Benjamin S Ozdemirli M. Ig G 4-related disease involving the esophagus: A clinicopathological study. Dis Esophagus. 2017;30(12):1–7.10.1093/dote/dox 09128881885 · doi ↗ · pubmed ↗