Liver and bladder morbidity in a Schistosoma mansoni and haematobium co-endemic area in the Democratic Republic of Congo
Sylvie Linsuke, Joule Madinga, Clémentine Roucher, Mamy-Irène Miantezila, Sylvain Baloji, Michel Disonama, Jean-Pierre Van Geertruyden, Katja Polman, Pascal Lutumba

TL;DR
This study found high rates of liver and bladder disease in a Congolese village where two types of schistosomiasis coexist, with mixed infections increasing bladder disease risk.
Contribution
The study provides new insights into the health impacts of mixed Schistosoma infections in a co-endemic region of the DRC.
Findings
Bladder morbidity was significantly higher in individuals with mixed Schistosoma infections compared to those with single S. haematobium infections.
Liver morbidity was common but not significantly different between mixed and single S. mansoni infections.
Age was a strong risk factor for both liver and bladder morbidity, with older individuals showing higher odds of disease.
Abstract
Both Schistosoma (S.) mansoni and S. haematobium are co-endemic in many regions of the Democratic Republic of the Congo (DRC). However, little is known about the clinical implications of mixed Schistosoma infections for the affected communities. This study determined Schistosoma-related morbidity patterns in single and mixed Schistosoma infections in DRC. Between November 2015 and March 2016, we conducted a community-wide study in the rural community of Kifwa II village, west of the DRC. According to WHO guidelines, Schistosoma-specific morbidity was assessed using ultrasound. Data were summarized using descriptive statistics, the Chi-square test, and logistic regression. Ultrasound examinations were performed on 825 individuals aged 1–80 years. The results indicated that 68% (559) of the participants had bladder morbidity, with a higher prevalence observed in those with mixed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
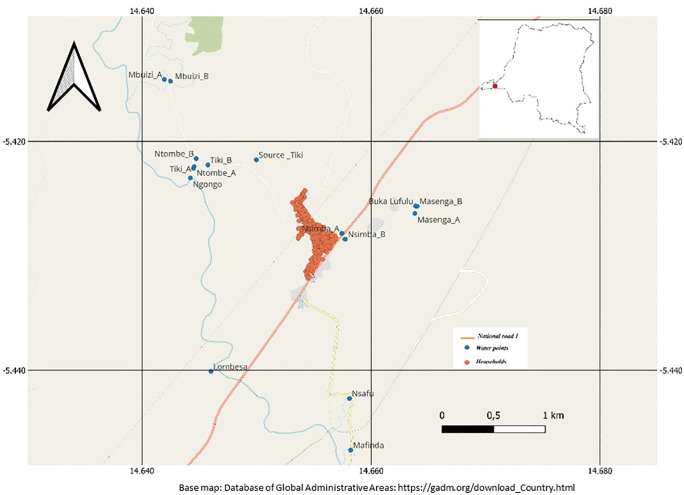 Fig 1
Fig 1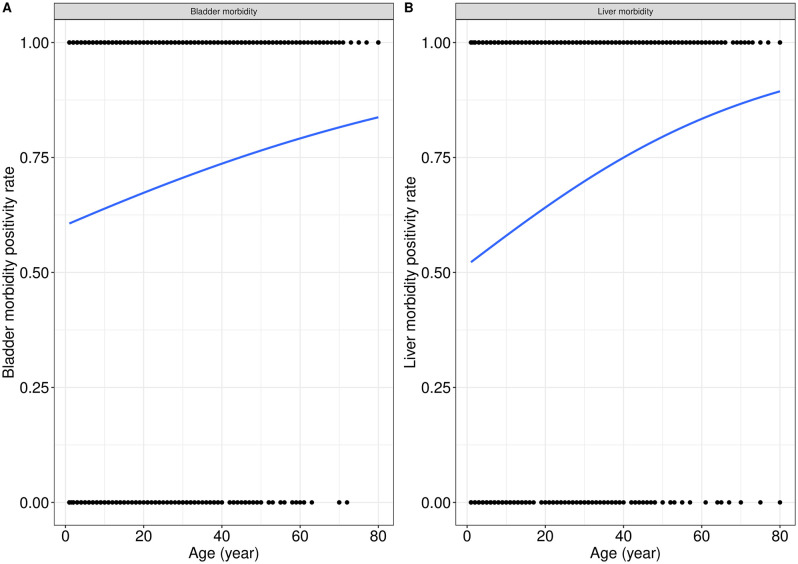 Fig 2
Fig 2- —Institute of Tropical Medicine in Belgium, Antwerp, Belgium, and the National Institute for Biomedical Research, Kinshasa, Democratic Republic of the Congo
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Parasite Biology and Host Interactions · Research on Leishmaniasis Studies
Background
Schistosomiasis is a chronic and devastating disease responsible for substantial morbidity, especially in rural areas of Sub-Saharan Africa (SSA), where the disease remains a major public health problem [1]. Globally, an estimated 779 million persons worldwide are at risk of schistosomiasis, 254 million are infected and 20 million have severe consequences [2]. In 2021, the global burden of schistosomiasis was estimated at 1,862,252 (1,038,122-2,984,204) disability-adjusted life-years lost; 90% of this burden occurred in SSA [3,4]. Two major Schistosoma species prevail in SSA: Schistosoma (S.) mansoni and S. haematobium, responsible for intestinal and urogenital schistosomiasis, respectively [1].
In endemic areas, chronic infection with schistosomiasis can cause important health problems, mostly among children, including anemia, malnutrition, stunting, and impaired cognitive development [5–8]. Moreover, if left untreated, the inflammatory and granulomatous immune responses of the host’s organism to worm eggs trapped in organ tissues can lead to permanent organ damage of the urinary or intestinal tracts [5,9–18]. Lesions are located according to the oviposition site of the Schistosoma species involved: S. mansoni causes liver lesions, whereas S. haematobium causes bladder lesions [1,9].
Schistosomiasis-related morbidity is heterogeneously distributed within the human population and is generally associated with high infection intensity [19–21]. Bladder morbidity has been reported to be more frequent in children, while liver morbidity is more frequent in adults [22–25]. Regarding gender, males are reportedly more prone to schistosomiasis-related morbidity compared to females [22–26]. However, most of these epidemiological studies were conducted in mono-endemic areas or reported only one Schistosoma species [13,27–33], and little is known about schistosomiasis-related morbidity in areas co-endemic for both S. mansoni and S. haematobium, where mixed infections are commonplace. The available studies showed that overall mixed infection with S. mansoni and S. haematobium reduces the risk of liver and splenic pathology while increasing urogenital pathology [34,35].
The Democratic Republic of the Congo (DRC) is endemic to schistosomiasis, with 15 million infected persons (7.3% within SSA and 6.6% worldwide) [36–39]. Both S. mansoni and S. haematobium have been prevalent in the country, with a large overlap of S. haematobium- and S. mansoni-endemic areas [37,40]. However, there is a paucity of published information on the prevalence of S. mansoni and S. haematobium mixed infections in the country. In a recent study conducted in the same region as for the current study, we found 38.4% of mixed infections among school-aged children [40]. Similarly, little is known about the extent of Schistosoma-related morbidity in the country for both single and mixed infections. Data reporting morbidity due to Schistosoma infections in the DRC is old and limited to clinical observations [28,40–50], except for one study conducted in Ituri in the northeast of DRC on morbidity related to S. mansoni using ultrasound data [27]. So far, no studies have addressed the morbidity of S. haematobium or mixed infections in DRC. The current study aims to determine patterns of S. haematobium-specific bladder morbidity and S. mansoni-specific hepatic morbidity in a co-endemic rural community and compare morbidity in those with mixed Schistosoma infections to those with single infections.
Materials and methods
Ethical statement
Ethical approval was received from the Ethics Committee of the School of Public Health of Kinshasa University (approval No ESP/CE/050/2014) in DRC, the Institutional Review Board of the Institute of Tropical Medicine of Antwerp (approval No 852/12) and the University of Antwerp (approval No 12/50/423) in Belgium. The study was also authorized by DRC’s Ministry of Health (MoH). Written informed consent was obtained from all participants before their inclusion. For participants under 18 years, written informed consent was obtained from their parents or legal guardians with the verbal consent of the children if aged more than 14 years.
Study setting and design
A community-based cross-sectional study was conducted between November 2015 and March 2016 among communities living in a rural area of Kifwa II village (Fig 1), located in the western part of the DRC between -5°25’1” degrees latitude south and 14°39’19.1” degrees longitude east. Its surface is 9965 km^2^ with an estimated population of around 1,400 inhabitants. The climate is tropical with two seasons. The dry season is between June and September, and the rainy season is between October and May, interrupted by a small dry season in February. The village is located alongside the Ngongo River and is home to several water points, including Ngongo, Mbwizi, Tiki, Ntombe, Masenga, Nsimba, Lombesa, N’Samfu, Buka Lufulu, and Kiminga (Fig 1). These various sources are also used for irrigation activities, as most residents are involved in agriculture, which remains their primary economic activity. Besides, the residents of this village do not have access to water in their households and instead rely on the various rivers (Fig 1) for their water supply. Based on information collected from local health zone leaders, Kifwa II village is endemic to both S. mansoni and S. haematobium. However, before the current study there were no public health interventions targeting schistosomiasis in the area.
Map of the Study site showing Kifua II village in the DRC.(The base layer of the figure in this paper was obtained from the database of Global Administrative Areas: https://geodata.ucdavis.edu/gadm/gadm4.1/shp/gadm41_COD_shp.zip).
Data collection and processing
The study participants included community members of Kifua II village. Eligible participants were residents aged ≥ 1 year who had lived in the area for at least one year, had no recent history of taking anthelminthic drugs, and willing to provide urine and stool samples. Those who refused to give consent were not included in the study. Before starting the survey, the researchers’ team visited the study area and informed the chief of the village about the study objectives. The heads of the households were also informed about the study. Eligible participants who gave informed consent (or parental consent for minors) were invited to provide two stool and two urine samples on consecutive days within one week for the diagnosis of helminth infections (Schistosoma spp. and other intestinal helminths). Each participant received two pre-labeled, clean and dry 50ml containers with a unique identification number (ID) and was instructed to fill them with at least half volume of urine and stool respectively. Clear instructions for the hygienic collection procedure were given. Samples were collected in the morning between 8:00 AM and 12:00 PM, as most of the people left the village for farming activities thereafter. They were then logged on a registration form upon receipt for proper tracking, and transferred in cool boxes to the laboratory of IME/Kimpese for analyses according to the standard operating procedures of the study. After completing the parasitology assessment, all participants were invited to the village’s health center for an ultrasound examination to detect organ pathologies due to S. mansoni and S. haematobium infections. Demographic data were also recorded from all participants using a structured pre-tested questionnaire.
Parasitology examination
Two stool and two urine samples were collected on two consecutive days and processed microscopically using standard parasitological procedures as recommended by the WHO guidelines for estimating infection prevalence and intensity [51].
For stool, duplicate Kato-Katz thin smears were prepared from each sample (2x2 smears per participant) and examined microscopically for egg counts expressed as eggs per gram (epg) [52]. Briefly, the stool was pressed through a metal mesh (Sterlitech Corporation, nylon screen, 100 mesh) to remove large particles. Then, a portion of 25 mg of the sieved fecal material was transferred to produce thick Kato-Katz smears on a slide. This was covered with a piece of cellophane soaked in a glycerol and methylene blue solution. All slides were examined under a microscope within 24 hours by two independent trained technicians to detect and count S. mansoni eggs. Infection load was calculated by finding the average of the number of egg counts from 4 slides, multiplied by 24 to estimate the epg of stool. Intensity of S. mansoni infection was reported as the number of eggs per grams (epg) and classify as per WHO guidelines [51] into light (1–99 epg), moderate (100–399 epg), or heavy (≥400 epg) infection.
For urine, 10 mL samples were processed using membrane filtration (2 × 1 slide per participant) and examined for S. haematobium eggs [53,54]. As previously described, 10 ml of urine from each sample was collected in a syringe after gently shaking and filtering through a 12 µm Isopore membrane filter. The membrane filter was then placed on a slide, dropped with Lugol’s iodine, and examined immediately under a microscope. The number of eggs observed in the preparation was recorded. Intensity of S. haematobium was reported as the number of eggs per 10 ml of urine (ep10 ml), and infection intensity was categorised per WHO guidelines [51] into light (1–49 eggs) or heavy (≥50 eggs).
To ensure quality, a senior technician who was blinded to the results of the other two technicians re-examined 10% of the randomly selected slides of all positive and negative stool and urine samples.
Ultrasound examination
Ultrasound examinations were performed on all participants using a portable ultrasound machine (SonoAcerR3) with a convex 3.5 MHz transducer. All ultrasound examinations were performed independently by two trained physicians who were not informed about the parasitological results of the participants. Based on the Niamey protocol, S. mansoni and haematobium-related morbidity indicators were evaluated [55,56]. S. mansoni-specific liver morbidity was determined by the presence of the liver image pattern. Liver image pattern was graded to A, B, C, D, E, and F (A = no sign of periportal fibrosis, B = incipient periportal fibrosis not excluded, C = periportal fibrosis possible, D = periportal fibrosis probable, E = advanced periportal fibrosis, and F = very advanced periportal fibrosis). Based on the degree of fibrosis, liver image patterns A and B were considered normal or not specific to S mansoni infection, and liver image patterns C, D, E, and F were considered S. mansoni-specific morbidity. For S. haematobium-specific morbidity, urinary bladder morbidity was determined using the WHO score [55,56]. A score of 0 was considered normal ultrasound or absence of bladder anomalies, and a score ≥1 indicated bladder abnormalities, which increased in severity (scores 1, 2, and 3), and was considered as S. haematobium-specific urinary bladder morbidity.
Data analysis
Data were double-entered into Access software, and statistical analyses were performed using Stata software 12.0. Descriptive analysis was applied to summarize the data. These include frequency and proportions for categorical variables, means with standard deviations, or medians with interquartile range for continuous variables, depending on the distribution. The geometric mean of egg counts (GM epg or GM ep 10ml for S. mansoni and S. haematobium, respectively) was calculated individually for participants who were positive for Schistosoma infections, after log-transformation to determine Schistosoma infections intensity. The chi-square test (χ2) was estimated to compare proportions between groups. Logistic regression using generalized linear models was used to assess the effect of participant age on the bladder and liver morbidity positivity rate. Besides, multivariable logistic regression models were developed to determine the predictors of schistosomiasis-related morbidity. Gender, age, S. haematobium infection, and S. mansoni infection were included as potential risk factors. To assess the impact of mixed infections on morbidity, participants were categorized into four groups: (i) single S. haematobium infection, (ii) single S. mansoni infection, (iii) co-infection with S. haematobium and S. mansoni, and (iv) uninfected individuals, who served as the reference group. Only variables with a likelihood ratio p-value <0.25 were included in the multivariable analysis for each model. The final model was selected using a backward elimination based on the smallest Akaike information criterion (AIC). The results were reported as adjusted OR (aOR), and a p-value of <0.05 is considered significant.
Results
General characteristics of participants
Complete data (parasitological and ultrasound data) were obtained from 825 participants, of which 393 (47.6%) were males and 432 (52.4%) were females. The median age of all participants was 15 years (IQR: 7–36 years; Range: 1–80 years) (Table 1). Parasitological examination revealed the overall prevalence rate of Schistosoma infection at 77.2% (637/825), with S. haematobium at 57.9% (478/825), S. mansoni at 57.6% (457/825 of whom 38.3% (316/825) were mixed infections. Distributions of single and mixed Schistosoma infections according to gender and age are summarized in Table 1.
Table 1: General characteristics of study participants and Schistosomiasis prevalence pattern according to gender and age.
Schistosoma-related specific morbidity prevalence and infection status
Overall, 67.8% (559/825) of the study participants had bladder morbidity, with the most important type of bladder morbidity score observed among the study participants being a score 2 (73.3%; 410/559), followed by the score ≥3 (25.8%; 144/559). A small proportion of participants, 0.9% (5/559), presented a bladder morbidity score of 1 (Table 2). Out of 559 individuals with bladder morbidity, 116 (20.8%) were not infected, 103 (18.4%) had a single S. haematobium infection, and 246 (44.0%) had a mixed infection (Table 2). Furthermore, the prevalence rate of bladder morbidity was higher among those with mixed infection compared to those with a single infection (χ2 = 11.1; p = 0.001).
Table 2: S. haematobium-associated bladder morbidity and Schistosoma species infection status among the study participants.
The overall prevalence rate of liver morbidity among the study participants was 64.6% (533/825). Grade C (86.3%; 460/533) was the most common liver image pattern, followed by D (11.1%; 59/533) in the study participants. Severe liver morbidity (liver image pattern E and F) was only shown in 2.6% (14/533) of the study participants (Table 3). Of 533 participants who had liver morbidity, 113 (21.2%) were not infected, 114 (21.4%) had a single S. mansoni infection, and 207 (38.8%) had a mixed infection (Table 3). However, there was no difference in the prevalence rate of liver morbidity among those infected with a single S. mansoni and those with mixed infection (χ2 = 1.9; p = 0.174).
Table 3: S. mansoni-associated liver morbidity and Schistosoma species infection status among the study participants.
Of the 825 individuals screened by ultrasound in this study, 690 presented with Schistosoma-related morbidity. Of these individuals, 149 (21.6%) tested negative for schistosomiasis, with no differences between this group and those who were infected. However, stratified analysis by gender and age showed no difference in infection prevalence by gender. Age, however, showed a significant difference in prevalence, particularly among those aged 11–20 (p = 0.001) and 51–60 (p = 0.029). Characteristics and distribution of individuals with any morbidity without infection are shown in Table 4.
Table 4: Distribution of participants with morbidity according to infection status, stratified by gender and age.
Age-related patterns of specific morbidity
Fig 2A and 2B illustrates the effects of participant age on bladder and liver morbidity positivity rates. It can be observed from Fig 1A and 1B that bladder and liver morbidity positivity rates increased as participant age increased (X1=13.67, p=0.0002 (Fig. 2A), and X2= 38.3, p = 0.0001 (Fig. 2B)).
Association between age of participants and bladder and liver morbidity.
Risk factors of bladder and liver morbidity
Bladder morbidity was significantly associated with age (Table 5), particularly in participants aged 11–20 years (aOR=1.6, p = 0.035), 21–30 years (aOR=1.7, p = 0.046), 41–50 years (aOR=2.2, p = 0.005), 51–60 years (aOR=3.2, p = 0.001), and over 60 years (aOR=3.6, p = 0.006). Liver morbidity was also strongly age-dependent, with significantly higher odds observed in participants aged 11–20 years (aOR=1.5, p = 0.048), 21–30 years (aOR=1.7, p = 0.026), 41–50 years (aOR=3.2, p < 0.001), 51–60 years (aOR=4.5, p < 0.001), and over 60 years (aOR=3.1, p = 0.011).
Table 5: Predictors of bladder and liver morbidity in Kifwa II community, DRC.
In unadjusted analysis, S. haematobium infection was significantly associated with bladder morbidity (cOR=1.8; 95% CI: [1.3–2.4]; p < 0.001). Similarly, S. mansoni infection showed an increased risk of bladder morbidity (cOR = 1.5; 95% CI: [1.1–2.0]; p = 0.006). However, after adjustment, there was a strong interaction between both Schistosoma infections with bladder morbidity (Interaction OR=2.4; 95% CI: [1.3–4.4]; p = 0.006), and the individual infections were no longer significant in the adjusted model (S. haematobium: aOR = 1.2 (95% CI: [0.8–1.9]; p = 0.451); S. mansoni: aOR = 0.8 (95% CI: [0.5–1.3]; p = 0.37) (S1 Table). Therefore, we performed a stratified analysis by infection status which confirmed that co-infected participants (S. mansoni + S. haematobium) had a significantly higher risk of bladder morbidity (cOR = 2.2; 95% CI: [1.5–3.2]; p < 0.001) compared to those with single infections. Furthermore, after adjusting for age and & gender, the risk of bladder morbidity remained significantly higher among participants with mixed infection (aOR =2.3, 95% CI: 1.5–3.5; p < 0.001) compared to those with single infections.
For liver morbidity, neither S. haematobium (OR = 1.5; 95% CI: [1.1-2.0]; p = 0.006) nor S. mansoni (OR = 1.5; 95% CI: [1.1-2.0]; p = 0.006) infection increased the risk of bladder morbidity (OR = 1.5; 95% CI: [1.1-2.0]; p = 0.006) in the unadjusted analysis. After adjustment, there was no significant interaction between liver morbidity and both infections (OR=1.4 [95% CI: 0.9-2.0], p = 0.125). Gender was also not a predictor of liver morbidity (OR=0.9 [0.7-1.2], p = 0.553). Therefore, we adjusted for age only, which showed no significant association between liver morbidity and S. mansoni (OR=1.3 [95% CI: 1.0-1.8], p = 0.062) or S. haematobium (OR=1.0 [95% CI: 0.7-1.4], p = 0.975).
Discussion
The current study used ultrasound to assess schistosomiasis-related morbidity in a setting where S. haematobium and S. mansoni are co-endemic, thus contributing to a better understanding of the effect of mixed infection on bladder and liver morbidity patterns.
Overall, we found a high prevalence of both bladder (68%) and liver (64.6%) schistosomiasis-specific morbidity, which indicates a hyperendemicity profile for the disease in this study area, given their high prevalence. Previous studies conducted in mono or co-endemic conditions have shown that the prevalence of morbidity related to schistosomiasis can vary considerably across different regions [20,22,27,33,57,31]. The difference in prevalence may be attributed to variations in study populations and local factors such as the extent of schistosomiasis transmission or a history of mass treatment [19,20]. Our study was conducted in a praziquantel-naïve population exposed to infected water daily through farming and other at-risk water contact activities, which could explain the high prevalence of schistosomiasis-related morbidity.
The prevalence of bladder morbidity was found to be higher in participants with mixed infections compared to those with a single S. haematobium infection. In contrast, no difference in the prevalence rate of liver morbidity was observed between those coinfected compared to those with a single S. mansoni infection. This agrees with a similar study from Mali [35] in which the authors reported higher bladder morbidity in mixed compared to single S. haematobium infections, even if lower liver morbidity was found in mixed compared to single S. mansoni infections. Conversely to our findings, a lower S. haematobium-associated urogenital morbidity was shown in the coinfected participants in Kenya relative to single S. haematobium infections [54].
Additionally, while other similar studies in co-endemic areas have found that the prevalence of morbidity linked to S. haematobium appears to increase with co-infection, and at the same time, that related to S. mansoni tends to decrease or conversely [21,23,35], our study showed a similar trend in the prevalence of bladder and liver morbidity. This interesting result requires further investigation.
Interestingly, nearly a fourth of individuals (21.6%) who presented with morbidity were negative for the infection. This result must be interpreted in the context of the limitations of parasitological techniques in detecting low infection or other underlying disease conditions which have not been investigated in this study [58–60]. Therefore, it is possible that some of those who tested negative were actually infected, which has implications for recommendations regarding control measures. However, given the profile of the research area, these results are not surprising. The observed morbidity in this group may be due to the long-term, chronic effects of past infection rather than active infection.
Demographic (age and sex) patterns of schistosomiasis-associated morbidity in our study contrasted with those from other studies [22–26]. The likelihood of both bladder and liver morbidity increases with age. In fact, we found that age was correlated with the risk of both bladder and liver morbidity. For instance, in contrast to other studies where children were more at risk of bladder morbidity while adults were more at risk for hepatic fibrosis [22–25], our study found that adults were systematically more at higher risk of both bladder and liver morbidity. Regarding sex, no significant difference was found between males and females, which differ from other studies that reported males being more at risk for bladder morbidity and hepatic fibrosis than females [22–26].
Our findings confirmed that mixed infection increased significantly the risk of bladder morbidity (aOR=2.3; p < 0.001). Our results on bladder morbidity are in line with a study conducted in Mali [35], which found that bladder pathology was increased in co-infections over S. haematobium mono-infections. However, there is a contrast between one study in Kenya [54] and another in Senegal [22], which found that bladder pathology decreased in co-infections. This suggests a protective effect of current S. mansoni infection on bladder morbidity. Increased bladder morbidity could be explained by interspecies competition. It has been hypothesized that males of S. haematobium outcompete males of S. mansoni, leading to a shift in worm pair location. This results in preferential egg entrapment and pathology in the bladder rather than the liver [34,61,61–65]. In the study, as mentioned earlier conducted in Senegal [22], the reduced bladder morbidity was explained by the production of more ectopic S. mansoni than ectopic S. haematobium eggs resulting from heterologous pairs made of the competitively stronger male of S. haematobium and S. mansoni female. It was speculated that these heterologous pairs would produce less pathogenic eggs than homologous S. haematobium worm pairs or that their eggs would deviate to other sites [20,22,34,66]. Of note, nothing is known yet about the pathogenicity of eggs from heterologous pairs, and further studies are warranted to understand this phenomenon better. Another hypothesis from the Senegalese study is the chronology of the invasion by each Schistosoma species [67–69]. In Senegal, S. haematobium transmission occurred later than that of S. mansoni, raising the possibility that cross-resistance from S. mansoni may have conferred some protection in individuals with mixed infections. This hypothesis could not be evaluated in our study, as ectopic eggs were not examined and the historical sequence of Schistosoma species introduction in the study area is unknown. Unlike the protective effect reported in Senegal [23], we observed that co-infection with S. haematobium and S. mansoni was associated with an increased risk of bladder morbidity. The mechanisms underlying this association remain unclear, highlighting the need for further studies exploring immune-pathological interactions*.*
Regarding liver morbidity, our results showed no significant risk factor except age, which is in line with the aforementioned study in Senegal [22] but in contrast with the aforementioned study in Mali [35] and another study in Cameroun [34] where a decreased risk for abnormal liver imaging and hepatomegaly was found for coinfected versus S. mansoni mono-infected. More research is needed to better understand the effect of mixed infection on liver morbidity.
We acknowledge that our study has certain limitations. Firstly, the present study included the entire population, including children less than two years of age. As the anatomical structures of the liver and bladder are still developing at this age, it is debatable whether the observed prevalence of lesions in this group is accurate. However, given the high endemicity of schistosomiasis in our research area, with infections occurring at a time when organs are still developing, the potential severity of tissue lesions could be significantly greater. Furthermore, we did not consider other infections that can cause hepatomegaly and splenomegaly, particularly in children, such as malaria [13], which is also prevalent in the study area. Nevertheless, given that only 25 children under two years old were included in our study (13 of whom showed lesions), we believe this would not influence the overall age trend of bladder and liver morbidity. Another limitation was that the parasitological techniques used (the Kato-Katz method and filtration technique for analysis of the stool and urine samples, respectively) were ineffective in detecting low infection or after treatment with praziquantel. This likely resulted in an underestimation of the prevalence. Therefore, other techniques are necessary. In this study, however, we improved the sensitivity of these methods by collecting multiple samples: two stool samples and two urine samples on consecutive days.
In summary, the results of this study could have implications for disease control. Currently, mass drug administration with praziquantel tackles disease morbidity in school-aged children. However, our results showed that this morbidity is common in all ages and increases with age, suggesting a need for control measures also for adults. This includes regular MDA with praziquantel, considering the adult population. Community-based interventions like improved WASH infrastructure and health education to encourage behavioural change are also crucial for long-term control.
Supporting information
S1 DataMorbidity database.(XLSX)
S1 TableThe interaction model evaluated the effect of mixed infection compared to S. haematobium and S. mansoni mono-infection on bladder morbidity and liver morbidity.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gryseels B, Polman K, Clerinx J, Kestens L. Human schistosomiasis. Lancet. 2006;368(9541):1106–18. doi: 10.1016/S 0140-6736(06)69440-3 16997665 · doi ↗ · pubmed ↗
- 2World Health Organization. Number of people requiring preventive treatment for schistosomiasis. https://archive.ourworldindata.org/20250909-093708/grapher/population-requiring-preventive-chemotherapy-for-schistosomiasis.html. 2024. Accessed 2025 October 5.
- 3World Health Organization. Global health estimates 2021: Disease burden by cause, age, sex, by country and by region, 2000-2021. Geneva: World Health Organization. 2024. https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates
- 4Institute for Health Metrics and Evaluation IHME. Global burden of disease 2021: findings from the GBD 2021 study. Seattle, WA: IHME. 2024. https://vizhub.healthdata.org/gbd-results/
- 5King CH, Dangerfield-Cha M. The unacknowledged impact of chronic schistosomiasis. Chronic Illn. 2008;4(1):65–79. doi: 10.1177/1742395307084407 18322031 · doi ↗ · pubmed ↗
- 6Friedman JF, Kanzaria HK, Mc Garvey ST. Human schistosomiasis and anemia: the relationship and potential mechanisms. Trends Parasitol. 2005;21(8):386–92. doi: 10.1016/j.pt.2005.06.006 15967725 · doi ↗ · pubmed ↗
- 7Ezeamama AE, Bustinduy AL, Nkwata AK, Martinez L, Pabalan N, Boivin MJ, et al. Cognitive deficits and educational loss in children with schistosome infection-A systematic review and meta-analysis. P Lo S Negl Trop Dis. 2018;12(1):e 0005524. doi: 10.1371/journal.pntd.0005524 29329293 PMC 5766129 · doi ↗ · pubmed ↗
- 8Jukes MCH, Nokes CA, Alcock KJ, Lambo JK, Kihamia C, Ngorosho N, et al. Heavy schistosomiasis associated with poor short-term memory and slower reaction times in Tanzanian schoolchildren. Trop Med Int Health. 2002;7(2):104–17. doi: 10.1046/j.1365-3156.2002.00843.x 11841700 · doi ↗ · pubmed ↗