Effect of Different Sodium Hypochlorite Concentrations on Post Endodontic Pain: A Systematic Review and Meta‐Analysis of Randomized Controlled Trials
Kavalipurapu Venkata Teja, Kaligotla Apoorva Vasundhara, Romeo Patini, Salvatore Scolavino, Gianrico Spagnuolo, Flavia Iaculli, Mariangela Cernera

TL;DR
This study reviews whether different concentrations of sodium hypochlorite affect post-root canal pain, finding no significant difference but suggesting lower concentrations may cause less pain.
Contribution
The study provides a systematic review and meta-analysis comparing low and high sodium hypochlorite concentrations for post-endodontic pain outcomes.
Findings
No significant difference in post-operative pain between low (<5%) and high (≥5%) sodium hypochlorite concentrations.
Lower concentrations (<5%) were associated with less pain in some studies, though not consistently significant.
Only one study reported higher pain with lower sodium hypochlorite concentrations.
Abstract
The aim of the present systematic review and meta‐analysis was to evaluate the effect of different concentrations of sodium hypochlorite (NaOCl) on post‐operative pain following root canal treatment. The current study was conducted according to PRISMA guidelines and registered on PROSPERO (CRD42023451576). The research question was formulated according to PICO strategy and aimed at determining if different concentrations of NaOCl would have influenced post‐operative pain in adults following endodontic treatments. A comprehensive literature search was performed manually and through multiple electronic databases, using predefined keywords and MeSH terms. Randomized controlled trials (RCTs) comparing different NaOCl concentrations (< 5% vs. ≥ 5%) and reporting post‐operative pain in adults were included. The risk of bias was assessed using the Cochrane RoB 2 tool. Meta‐analyses were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
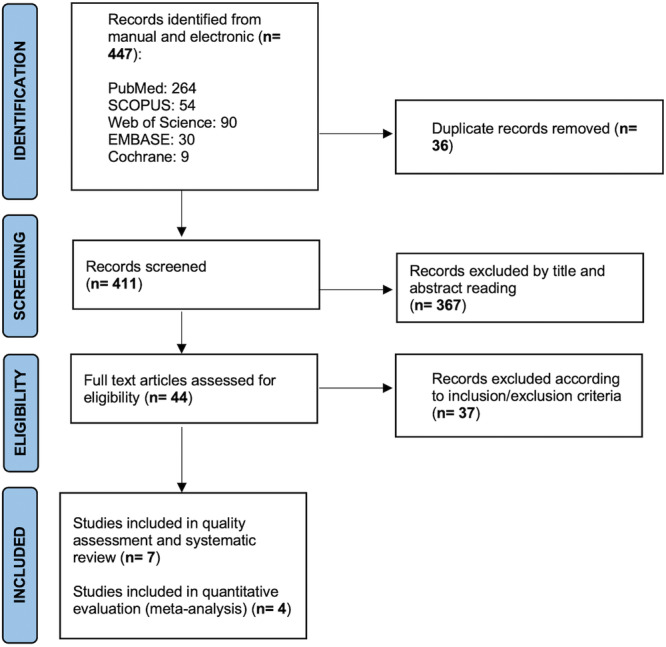 Figure 1
Figure 1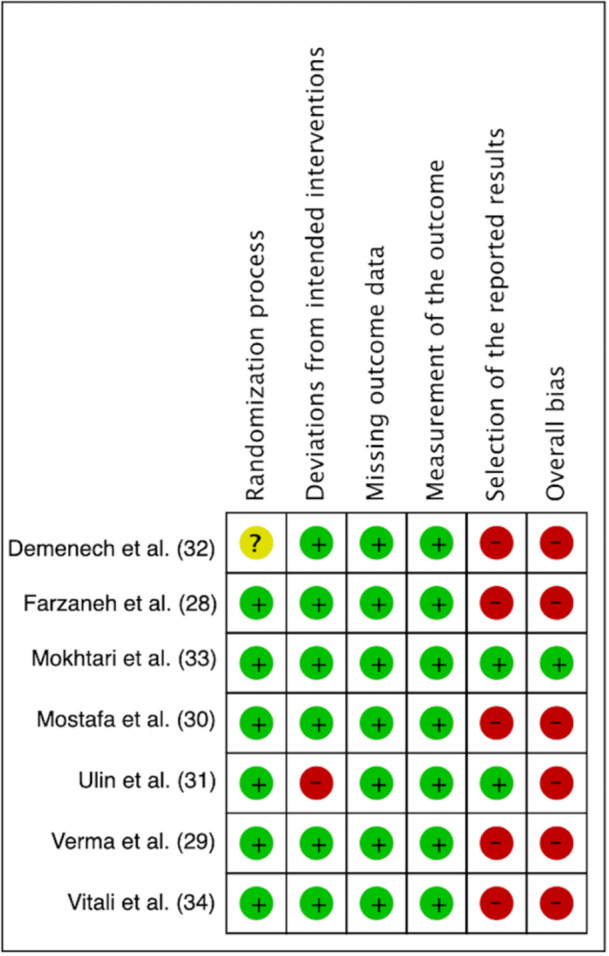 Figure 2
Figure 2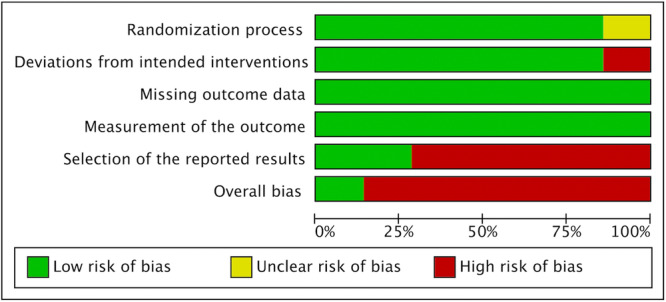 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6| PubMed | ((((((((((root canal irrigants) AND (sodium hypochlorite)) AND (different concentration)) OR (various concentration)) AND (post operative pain)) OR (post endodontic pain)) AND (randomized controlled trial))) AND (non randomized controlled trial)) AND (clinical study) |
| Web of Science | Root canal irrigants (All Fields) and sodium hypochlorite (All Fields) and different concentration (All Fields) or various concentration (All Fields) and post operative pain (All Fields) or post endodontic pain (All Fields) and randomized controlled trial (All Fields) and non‐randomized controlled trial (All Fields) and clinical study (All Fields) |
| Cochrane | Root canal irrigants in Title Abstract Keyword OR sodium hypochlorite in Title Abstract Keyword OR different concentration in Title Abstract Keyword AND post operative pain in Title Abstract Keyword AND clinical trial in Title Abstract Keyword |
| SCOPUS | (ALL (root AND canal AND irrigants) AND ALL (sodium AND hypochlorite) AND ALL (different AND concentration) AND ALL (post AND operative AND pain) OR ALL (post AND endodontic AND pain) AND ALL (randomized AND controlled AND trial) AND ALL (clinical AND study) AND ALL (non AND randomized AND controlled AND trial)) |
| Embase | (((‘root canal irrigants’/exp OR ‘root canal irrigants’ OR ((‘root’/exp OR root) AND canal AND irrigants)) AND (‘hypochlorite sodium’/exp OR ‘hypochlorite sodium’) AND (‘different concentration’ OR (different AND (‘concentration’/exp OR concentration))) OR ‘various concentration’ OR (various AND (‘concentration’/exp OR concentration))) AND (‘post operative pain’/exp OR ‘post operative pain’ OR (post AND operative AND (‘pain’/exp OR pain))) OR ‘post endodontic pain’ OR (post AND endodontic AND (‘pain’/exp OR pain))) AND (‘randomized controlled trial’/exp OR ‘randomized controlled trial’ OR (randomized AND controlled AND (‘trial’/exp OR trial))) AND (‘non randomized controlled trial’ OR (non AND randomized AND controlled AND (‘trial’/exp OR trial))) AND (‘clinical study’/exp OR ‘clinical study’ OR ((‘clinical’/exp OR clinical) AND (‘study’/exp OR study))) |
| N | Author | Year | Country | Tooth group | Patients’ number | Patient's age | Sex | N visit | Temporary dressing | Shaping Instrument | Coronal sealing |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Farzaneh et al. | 2018 | Iran | First and second mandibular molars with irreversible pulpitis. No AP | 110 | 28.56 ± 8.68 | 20M 35F | Single visit | NO | RaCe rotary instrument | ND |
| 28.34 ± 7.61 | 19M 36F | ||||||||||
| 2 | Verma et al. | 2019 | India | First and second mandibular molars, non vital and AP | 90 | 28.58 ± 7.61 | 21M 22F | Two visits | Calcium hydroxide paste + Cavit | Mtwo | Composite |
| 29.23 ± 7.93 | 18M 25F | ||||||||||
| 3 | Mostafa et al. | 2020 | Egypt | First and second mandibular molars, non vital, with or without AP | 303 | 32.14 ± 5.79 | 62M 92F | Two visits | No intracanal medication + Cavit | ProTaper Universal | Temporary filling |
| 31.60 ± 5.87 | 68M 86F | ||||||||||
| 4 | Ulin et al. | 2020 | Sweden | All teeth, vital and non vital, with or without AP | 211 | 51.6 ± 15.9 | 65M 87F | Single visit/two or more | Calcium hydroxide + zinc oxide‐eugenol cement | ProTaper, WaveOne, BioRace | Temporary filling (permanent restoration by referring dentist) |
| 51.5 ± 16.0 | 67M 78F | ||||||||||
| 5 | Demenech et al. | 2021 | Brazil | All teeth, vital and non vital, with or without AP | 169 | 34.7 ± 12.1 | 16M 27F | Single visit | NO | WaveOne Gold, ProDesign Logic | Glass ionomer cement |
| 37.8 ± 12.0 | 16M 26F | ||||||||||
| 6 | Mokhtari et al. | 2023 | Iran | First and second mandibular molars with irreversible pulpitis. No AP | 72 | 28.42 ± 9.27 | 8M 4F | Single visit | NO | Denco | Temporary filling |
| 31 ± 6.84 | 6M 6F | ||||||||||
| 7 | Vitali et al. | 2024 | Brazil | First or second mandibular molars, non vital, with AP | 154 | 33.51 ± 12.01 | 37M 40F | Single visit | NO | Reciproc | Composite |
| 33.75 ± 11.38 | 33M 44F |
| Quality Assessment, Outcome: Pain after NaOCl irrigation at different concentrations | ||||||
|---|---|---|---|---|---|---|
| Question: Among low and high concentration which one is more prone to cause pain after irrigation? | ||||||
| Number of studies according to meta‐analysis (n) | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias |
| n.4 Figure | RCT | High | Serious | Not serious | Serious | Undetected |
| n.4 Figure | RCT | High | Serious | Not serious | Serious | Undetected |
| n.4 Figure | RCT | High | Serious | Not serious | Serious | Undetected |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndodontics and Root Canal Treatments · Dental Erosion and Treatment · Legionella and Acanthamoeba research
Introduction
1
Endodontic treatment should not only focus on microbial elimination from the root canal system but also on mitigating the pain caused by various preoperative and postoperative factors (Smith et al. 2017). Pain management should take into account a variety of pre, intra and postoperative factors (Arias et al. 2013). Several variables such as type of irrigant, irrigation activation, extrusion of irrigants (Liapis et al. 2021; Karatas et al. 2021), flare‐up (Bassam et al. 2021), instrumentation techniques (Western and Dicksit 2017), debris extrusion (Adiguzel et al. 2019), occlusal reduction (Nguyen‐Nhon et al. 2020) could influence pain during and after the endodontic procedure. In addition, some mechanical factors might provoke post‐operative pain including enlargement of apical foramen (Silva et al. 2013), failure to maintain apical patency (Yaylali et al. 2018), over instrumentation of the root canal, movement kinematics (Adiguzel et al. 2019) and root canal sealers (Ferreira et al. 2020).
Evidence has proven that primary endodontic infections are predominated by gram positive microorganisms (Chávez de Paz 2004; Narayanan and Vaishnavi 2010). Prostaglandins (PGs)—a major component of the cell wall—contribute to trigger and up regulate the inflammatory process (Grga et al. 2013). Indeed, PGs cause vasodilation, increase vascular permeability, decrease the threshold of nociceptors that on turn evoke post‐operative pain. Moreover, it's been reported that the presence of PGE2, PGF2α, and PGA2 has a significant role in generating endodontic pain (Siqueirajr et al. 2002). Lipoteichoicacid (LTA), a component of gram‐positive bacterial cell wall, has shown to influence inflammatory mediators (Park et al. 2013). Enterococcus faecalis, a gram‐positive bacteria, possess polyglycerol phosphate‐type LTA (EfLTA) that plays an important role in biofilm formation and bacterial adhesion (Hong et al. 2016). In addition, LTA induces proinflammatory mediators and instigate the release of proinflammatory cytokines such as Tumor Necrosis Factor alpha (TNF‐a), Interleukin‐1 (IL‐1), Interleukin‐ 8 (IL‐8), Interleukin‐12 (IL‐12) (Henderson 1996; Parolia 2015). These proinflammatory cytokines cause further release of substance P that might increase endodontic pain (Jain et al. 2013). Furthermore, the extrusion of dentinal debris during root canal treatment, in combination with microbial agents and chemical disinfectants, may induce an acute inflammatory reaction in the periapical tissues, thereby causing post‐endodontic pain (Teja et al. 2025). Sodium hypochlorite (NaOCl), the mostly used endodontic irrigant, presents several properties as antimicrobial effect, canals lubrication, smear layer formation prevention and pulp tissue dissolving, and it's been demonstrated to be effective in inactivating and eliminating LTA (Marending et al. 2007). However, its extrusion into the periradicular area may result in significant adverse tissue reactions and pain due to its caustic nature (Prasad et al. 2024). Although it's been demonstrated that higher NaOCl concentrations are associated with post‐operative pain occurrence (Prasad et al. 2024; Sabino‐Silva et al. 2023), its optimal safe concentration as well as the persistence of pain within the first 72 h should be further elucidated. Therefore, the aim of the present systematic review and meta‐analysis was to assess the influence of different concentrations of NaOCl on post‐operative pain following root canal treatment.
Material and Methods
2
The current systematic review was prepared in agreement with the PRISMA guidelines statement (Page et al. 2021) and the review protocol was listed on PROSPERO (CRD42023451576).
The review addressed a focused question by using the participant, intervention, comparison, outcomes, study design (PICOS) criteria as follows: “Does different concentrations of sodium hypochlorite influence post‐operative pain in adults following root canal treatment in randomized clinical trials?”
Population: Healthy subjects > 18 years old.
Intervention: Root canal treatment of dental elements with necrosis or irreversible pulpitis.
Comparison: Different concentrations of sodium hypochlorite used during root canal treatment.
Outcome: Post‐operative pain incidence.
Study: Randomized clinical trials.
Search Strategy
2.1
A comprehensive literature search was conducted through multiple electronic databases (PubMed, Scopus, Web of Science, EMBASE, Cochrane) up to December 2024 using specific keywords and Mesh terms as reported in Table 1. A manual search restricted to papers published between January 2000 and December 2024 was also conducted in these peer‐reviewed journals dealing with endodontic sciences: Journal of Endodontics, International Endodontic Journal, Australian Endodontic Journal, European Endodontic Journal, and Clinical Oral Investigation. Moreover, reference sections of the included articles were manually assessed to identify further papers for potential inclusion.
Eligibility Criteria
2.2
The papers were selected in agreement with the following criteria:
Inclusion criteria
- –Papers published in Peer‐reviewed Journals;
- –Full text articles published in English language;
- –Randomized clinical trials evaluating the effect of different concentrations of sodium hypochlorite (NaOCl) on post‐operative pain in adult patients underwent non‐surgical root canal therapy;
- –Randomized clinical trials conducted in accordance to Declaration of Helsinki guidelines developed by World Medical Association.
Exclusion criteria
- –Animal studies, in vitro studies, review articles, case reports, and case series.
- –Clinical and randomized controlled trials conducted on patients underwent retreatment.
- –Gray literature.
Selection of Studies
2.3
Two independent calibrated reviewers (M.C. and F.I.) screened the retrieved papers and identified relevant studies after removing duplicates. Based on the eligibility criteria, studies were evaluated by title and abstract. Then, full texts of possibly relevant papers were retrieved and evaluated. Any disagreements between examiners were solved by a third investigator (G.S.). Agreement level within the two examiners was recorded using Cohen's kappa coefficient (k).
Data Extraction
2.4
Data extraction forms were independently filled by the two examiners (M.C. and F.I.), for further analysis. The following information was reported: authors, year, country, tooth group, patients' number, patients' age, sex, number of visits, temporary dressing, shaping instrument, coronal sealing, pre‐operative sealing, use of painkillers before and after root canal therapy, NaOCl percentages, additional irrigation protocol, obturation material, obturation technique, pain evaluation scale, follow‐up time and main findings. When pain levels were not reported as numbers, the data were extracted from bar graphs or provided images using a specific tool (https://automeris.io/).
Risk of Bias and Quality Assessment
2.5
Qualitative assessment was independently performed by two examiners (M.C. and F.I.) on the included papers by means of a revised Cochrane risk‐of‐bias tool for randomized trials (RoB 2) (Sterne et al. 2019) on Review Manager 5.2 software (RevMan, The Nordic Cochrane Centre, Copenhagen, Denmark). Five domains were addressed to report the risk of bias: randomization processes, deviations from intended interventions, missing outcome data, measurement of the outcome and selection of the reported result. Based on the above‐mentioned criteria, the studies were categorized as “low risk,” “some concerns,” or “high risk.” Overall low risk of bias for a study was given when all the domains were scored as “low risk.” “Some concerns” was given to study with at least one domain scored as “some concerns.” Finally, a study was considered to have an overall high risk of bias when at least one domain was scored as “high risk” or more than two domains were scored as “some concerns.” An additional analysis of the overall quality of evidence for each meta‐analysis was independently conducted using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) system.
Data Synthesis
2.6
Data extraction was conducted independently and in duplicate by two examiners (M.C. and F.I.). Since the differences in reporting pain incidence among studies (i.e., pain scales applied differently), the pain occurrence was considered as present (summarizing together all levels of pain) or absent at every evaluated time points. Meta‐analyses were conducted with a fixed‐effect model only if the included studies were homogeneous in terms of study population demographics. Only in case of a not‐negligible heterogeneity across included articles, thus meaning clinical and methodological diversity across studies or the presence of studies with small sample size, a random‐effect model was used; moreover, a value of I ^2^ exceeding 50% was considered as predictive of non‐negligible heterogeneity. Meta‐analyses were conducted only for comparisons with at least four included studies.
Assessment of Heterogeneity and Statistical Analysis
2.7
The Review Manager (RevMan) software was used for assessing the heterogeneity across the included papers (The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager [RevMan] v. 5.2. Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration; 2013). The comparability of the observed differences across the results with chance alone was calculated by the authors using the χ ^2^ test and the I ^2^ test. Heterogeneity was considered significant if p value was < 0.1 (Review Manager 5.2 software—RevMan, The Nordic Cochrane Centre, Copenhagen, Denmark). Moreover, the I ^2^ test was considered as measure of heterogeneity across studies, as follows (Higgins et al. 2003):
- –0%–40%: negligible
- –30%–60%: moderate
- –50%–90%: substantial
- –75%–100%: considerable.
Results
3
Study Selection
3.1
The electronic and manual search resulted in 447 papers. After duplicates removal, a total of 411 records underwent evaluation by title and abstract. Then, full texts of the remaining 44 papers were retrieved and evaluated in agreement with the eligibility criteria. Finally, 7 papers were included in the current systematic review and processed for qualitative analysis (Farzaneh et al. 2018; Verma et al. 2019; Mostafa et al. 2020; Ulin et al. 2020; Demenech et al. 2021; Mokhtari et al. 2023; Vitali et al. 2024); in addition, 4 studies (Farzaneh et al. 2018; Verma et al. 2019; Demenech et al. 2021; Vitali et al. 2024)—that were enough homogenous in terms of study population demographics—were subjected to quantitative evaluation (meta‐analysis) (Figure 1). Cohen's kappa value for global inter‐reviewer agreement was almost perfect, being 0.89. Characteristics and outcomes of included papers are reported in Table 2.
PRISMA flow‐chart.
Study Characteristics
3.2
All included papers were randomized clinical trials reporting on non‐vital permanent teeth or teeth with signs and symptoms of irreversible pulpitis, thus candidate to root canal therapy. Five studies enrolled first and second mandibular molars (Farzaneh et al. 2018; Verma et al. 2019; Mostafa et al. 2020; Mokhtari et al. 2023; Vitali et al. 2024), while 2 papers included all teeth (Ulin et al. 2020; Demenech et al. 2021). Clinical procedures and protocols were different among studies. Specifically, root canal treatment was performed in a single visit in the majority of the studies (Farzaneh et al. 2018; Demenech et al. 2021; Mokhtari et al. 2023; Vitali et al. 2024), whereas 2 studies have performed therapy in two visits (Verma et al. 2019; Mostafa et al. 2020), using only in 1 paper (Verma et al. 2019) calcium hydroxide paste as medicament. In the study conducted by Ulin et al. (2020), authors state that root treatment was obtained in one, two or even more visits, using calcium hydroxide as pulp dressing material. Root canal shaping was obtained with different systems of mechanical instrumentation and cold lateral condensation was the main used obturation technique (Farzaneh et al. 2018; Verma et al. 2019; Mokhtari et al. 2023), following by single cone (Mostafa et al. 2020), vertical condensation (Vitali et al. 2024) and hybrid technique (Demenech et al. 2021). Resin based sealer (AH Plus, Dentsply Sirona) was applied in 6 out 7 study whereas one study used zinc oxide based sealer (Verma et al. 2019). Regarding irrigation protocol, the concentration of NaOCl used in the included studies ranged from 0.5% to 8.25% (0.5%, 1%, 1.3%, 2.5%, 5%, 5.25%, 8.25%) and ethylenediaminetetra‐acetic acid (EDTA) (15% or 17%) was applied as additional irrigant in all studies. Each study compared different low and high NaOCl concentrations, that ranged from 0.5% to 2.5% and from 5% to 8.25%, respectively.
Disparities were noticed in all included articles regarding the type of coronal seal. Two studies have placed composite (Verma et al. 2019; Vitali et al. 2024), 1 study glass ionomer cement (Demenech et al. 2021) and other 3 papers reported used temporary restoration (Mostafa et al. 2020; Ulin et al. 2020; Mokhtari et al. 2023). Farzaneh et al. (2018). did not provide the type of coronal seal placed.
Regarding pain assessment, co‐founding factors as pre‐operative pain evaluation was reported in 5 out 7 studies (Verma et al. 2019; Mostafa et al. 2020; Ulin et al. 2020; Demenech et al. 2021; Mokhtari et al. 2023). Accordingly, pain killers were administrated from 6 h to 3 days before endodontic treatment. Pain was evaluated using numeric visual analogue scale (VAS) (Farzaneh et al. 2018; Verma et al. 2019; Ulin et al. 2020; Demenech et al. 2021; Mokhtari et al. 2023) and numerical rating scales (NRS) (Mostafa et al. 2020; Vitali et al. 2024) at different time points. The first pain evaluation ranged from 0 h (immediately post‐treatment) to 12 h. In 3 studies the first pain assessment was performed directly 24 h post‐therapy (Verma et al. 2019; Ulin et al. 2020; Demenech et al. 2021).
The maximum follow‐up time was 7 days for all studies (Farzaneh et al. 2018; Mostafa et al. 2020; Ulin et al. 2020; Mokhtari et al. 2023), except for Demenech et al (2021) that reported values at 3 days and Vitali et al. (2024) that additionally reported pain assessment at 14 and 30 days. The qualitative review suggested that four studies showed no significant difference in post‐operative pain using low and high concentration of NaOCl (Verma et al. 2019; Ulin et al. 2020; Demenech et al. 2021; Mokhtari et al. 2023). On the other hand, 2 studies reported less post‐operative pain when low concentration of NaOCl was adopted, respectively 1.3% versus 5.25% (Mostafa et al. 2020) and 2.5% versus 8.25% (Vitali et al. 2024). Finally, controversial results were showed by Farzaneh et al. (2018) reporting that 3 days after root canal therapy the use of 5.25% NaOCl was related to significantly less pain than 2.5%.
Risk of Bias
3.3
The Cochrane Risk of Bias tool (RoB 2) was applied to assess quality of the included papers. Among them, 6 were categorized as having an overall high risk of bias (Farzaneh et al. 2018; Verma et al. 2019; Mostafa et al. 2020; Ulin et al. 2020; Demenech et al. 2021; Vitali et al. 2024) while the study conducted by Mokhtari et al. (2023) revealed an overall low risk (Figure 2). The shortcomings mostly concerned the deviations from the intended interventions (domain #2) for 1 study (Ulin et al. 2020) and the selection of the reported result (domain #5) in five papers (Farzaneh et al. 2018; Verma et al. 2019; Mostafa et al. 2020; Demenech et al. 2021; Vitali et al. 2024) (Figure 3).
Review authors’ judgment about each risk of bias item for each included study.
Review authors' judgment about each risk of bias item presented as percentages across all included studies.
Results of the Meta‐Analyses and Quality Assessment
3.4
Meta‐analyses were performed comparing the patients' perceived pain (presence or absence) when comparing different NaOCl concentrations in 3 different time‐frames: 24, 48, and 72 h after root canal treatment. The included studies were categorized based on low and high concentrations, using the following ranges as reference: low concentrations from 0.5% to 2.5% and high concentrations from 5% to 8.25%. The 3 meta‐analyses reported data of 480 patients for each time‐frame but none of them detected a statistically significant difference in perceived pain after using NaOCl at different concentrations (odds ratio: 0.69; 95% CI: 0.23–2.09; p value: 0.51, odds ratio: 0.56; 95% CI: 0.11–2.76; p value: 0.47, and odds ratio: 0.73; 95% CI: 0.12–4.34; p value: 0.73) at 24 (Figure 4), 48 (Figure 5) and 72 h (Figure 6), respectively. Conducted meta‐analyses reported notable heterogeneity according to I ^2^ values (I ^2^ = 83%, I ^2^ = 86%, and I ^2^ = 87%, respectively). The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) was used as a system to provide information on the certainty of the conclusions and the strength of the evidence (Table 3). Although the meta‐analyses drew conclusions from randomized clinical trials, considered to be the best‐available evidence, they were assessed to have only moderate strength of evidence because of high heterogeneity across all included studies and a general presence of wide confidence intervals in all meta‐analyses.
Forest plot of comparison: Pain after different NaOCl irrigation; outcome: Pain after 24 h.
Forest plot of comparison: Pain after different NaOCl irrigation; outcome: Pain after 48 h.
Forest plot of comparison: Pain after different NaOCl irrigation; outcome: Pain after 72 h.
Discussion
4
Pain control is a critical aspect of root canal therapy and its subsequent stages (Venkata Teja et al. 2021). One major factor contributing to post‐operative pain is the improper usage of irrigants. NaOCl, known for its potent antimicrobial and tissue‐dissolving properties, is widely used in concentrations ranging from 0.5% to 8% (Teja et al. 2022). However, due to various reported complications, there is no consensus on the ideal concentration for clinical use. To the best of our knowledge, no systematic review and meta‐analysis have been published evaluating different concentrations of NaOCl and their effect on post‐operative pain until 72 h after treatment. Therefore, the current study aimed to evaluate the relationship between NaOCl concentration and pain occurrence following root canal treatment.
Meta‐analyses conducted at 24, 48, and 72 h after treatment revealed no significant differences in post‐operative pain between high and low NaOCl concentrations, although lower concentrations were linked to less pain occurrence. The use of NaOCl at higher concentrations enhances its antimicrobial activity and tissue‐dissolving capacity; however, it also increases cytotoxicity (Parirokh et al. 2012; Zehnder 2006). When extruded into the periapical tissues, NaOCl cytotoxicity may lead to patient discomfort, highlighting the importance of careful concentration selection and proper irrigation technique (Parirokh et al. 2012; Zehnder 2006; De Santis et al. 2022). Evaluation range of post‐treatment pain should at least consider 3 days, that's the interval time in which post‐endodontic flare‐up is mainly represented (Shamszadeh et al. 2020). Prasad et al. (2024) recently reported a significantly lower incidence of post‐endodontic pain when lower concentrations of NaOCl were applied at 24 and 48 h after treatment. Accordingly, the quantitative analyses in the present study extended pain assessment to 72 h.
Each of the included study compared different NaOCl concentrations categorized as “low” and “high” that ranged from 0.5% to 2.5% and from 5% to 8.25%, respectively. Although the considerable heterogeneity among studies—6/7 of the included papers reported an overall high risk of bias—a low concentration of NaOCl seemed to be associated with less pain, significantly in 2 papers (Mostafa et al. 2020; Vitali et al. 2024) and not significantly in 4 articles (Verma et al. 2019; Ulin et al. 2020; Demenech et al. 2021; Mokhtari et al. 2023). Only Farzaneh et al. (2018) observed significantly less pain using 5.25% NaOCl than of 2.5%, 3 days after root canal treatment. In addition, only 4 studies (Farzaneh et al. 2018; Verma et al. 2019; Demenech et al. 2021; Vitali et al. 2024) underwent quantitative evaluation, since 2 papers (Ulin et al. 2020; Mokhtari et al. 2023) provided comparison of different low concentrations of NaOCl (0.5% vs. 3% and 0.5% vs. 1%, respectively), and the study conducted by Mostafa et al. (2020) reported pain levels 1, 2 and 7 days after the first visit (i.e., irrigation and instrumentation) and on the second visit immediately after root filling, without any additional follow‐up time.
The inconsistencies between reported outcomes may be due to different variables that affect pain incidence, such as long preparation time, irrigation technique, instrumentation technique, used sealer and overfilling (Gupta et al. 2021). The same Authors stated that their outcomes might be attributed to the pre‐operative pulpal and periapical status of the included teeth. Indeed, Farzaneh et al. (2018). treated vital dental elements with inflamed pulps and no periapical reaction, therefore the presence of normal periapical structures seemed to avoid extrusion of the irrigants and debris as well as the use of 5.25% NaOCl had higher dissolution capacity of the remaining apical pulp that resulted in less inflammation. Additional co‐morbidities such as number of visits and intracanal medication might be related to inflammatory response (Emara et al. 2019; Erdem Hepsenoglu et al. 2018). Half of the papers included in the current systematic review reported root canal treatment in a single visit, while the other half in 2 appointments. Moreover, the intracanal dressing was not comparable and the effectiveness of coronal sealing was impossible to evaluate. These aspects might contribute to pain occurrence and should be deeply evaluated. The histopathological status of the pulp and the presence of peri‐apical tissue reaction also played an important role in the release of signaling molecules that might trigger the up‐regulation of inflammation and pain incidence (Guivarc'h et al. 2017; Xu et al. 2022; Iaculli et al. 2022).
Different pain assessment methods were used across studies, as NRS and VAS. Although the assessed pain levels were comparable, NRS generally showed higher compliance and responsiveness compared to VAS (Armogida et al. 2022). Future studies should ensure detailed reporting of pain assessment methods and consider the potential bias in self‐reported outcomes. It should be also considered variability in inclusion criteria among studies, related to pre‐operative pain presence as well as use of pain killers before treatment. There is a need of standardized criteria to reduce heterogeneity and future trials should maintain balanced baseline variables and minimize factors leading to post‐operative pain.
Although clinical effectiveness of NaOCl is evident, the proper concentration to obtain positive effects and to limit the drawbacks need to be further elucidated. Since the current evidence is limited, additional well‐designed trials with standardized methods are warranted to provide more reliable clinical guidance.
Conclusion
5
Within the limits of the current systematic review and meta‐analysis, it could be concluded that there was no difference in post‐endodontic pain levels using different concentrations of NaOCl. However, concentration of NaOCl < 5% might be associated with less pain incidence.
Author Contributions
Study design and data extraction: Kavalipurapu Venkata Teja. Data extraction and interpretation: Kaligotla Apoorva Vasundhara. Meta‐analysis: Romeo Patini. Artworks and literature search: Salvatore Scolavino. Critical revision and results interpretation: Gianrico Spagnuolo. Search strategy and writing and editing of original manuscript: Flavia Iaculli. Search strategy, data interpretation and supervision: Mariangela Cernera.
Funding
The authors received no specific funding for this work.
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adiguzel, M. , P. Tufenkci , and I. Pamukcu . 2019. “Comparison of Postoperative Pain Intensity Following the Use of Three Different Instrumentation Techniques: A Randomized Clinical Trial.” Journal of Dental Research, Dental Clinics, Dental Prospects 13: 133–140.31592309 10.15171/joddd.2019.021PMC 6773924 · doi ↗ · pubmed ↗
- 2Arias, A. , J. C. de la Macorra , J. J. Hidalgo , and M. Azabal . 2013. “Predictive Models of Pain Following Root Canal Treatment: A Prospective Clinical Study.” International Endodontic Journal 46: 784–793.23402273 10.1111/iej.12059 · doi ↗ · pubmed ↗
- 3Armogida, N. G. , C. Rengo , M. Cernera , F. Iaculli , and G. Spagnuolo . 2022. “Transepithelial Gingival Depigmentation Using a New Protocol With Q‐Switched Nd:YAG: An In Vivo Observational Study.” Dentistry Journal 11, no. 1: 2.36661539 10.3390/dj 11010002 PMC 9857459 · doi ↗ · pubmed ↗
- 4Bassam, S. , R. El‐Ahmar , S. Salloum , and S. Ayoub . 2021. “Endodontic Postoperative Flare‐Up: An Update.” Saudi Dental Journal 33: 386–394.34803278 10.1016/j.sdentj.2021.05.005PMC 8589595 · doi ↗ · pubmed ↗
- 5Chávez de Paz, L. 2004. “Gram‐Positive Organisms in Endodontic Infections.” Endodontic Topics 9: 79–96.
- 6Demenech, L. S. , J. V. de Freitas , F. S. F. Tomazinho , F. Baratto‐Filho , and M. C. L. Gabardo . 2021. “Postoperative Pain After Endodontic Treatment Under Irrigation With 8.25% Sodium Hypochlorite and Other Solutions: A Randomized Clinical Trial.” Journal of Endodontics 47: 696–704.33607121 10.1016/j.joen.2021.02.004 · doi ↗ · pubmed ↗
- 7Emara, R. S. , H. M. Abou El Nasr , and R. M. El Boghdadi . 2019. “Evaluation of Postoperative Pain Intensity Following Occlusal Reduction in Teeth Associated With Symptomatic Irreversible Pulpitis and Symptomatic Apical Periodontitis: A Randomized Clinical Study.” International Endodontic Journal 52: 288–296.30171777 10.1111/iej.13012 · doi ↗ · pubmed ↗
- 8Erdem Hepsenoglu, Y. , T. F. Eyuboglu , and M. Özcan . 2018. “Postoperative Pain Intensity After Single‐ Versus Two‐Visit Nonsurgical Endodontic Retreatment: A Randomized Clinical Trial.” Journal of Endodontics 44: 1339–1346.30054099 10.1016/j.joen.2018.05.017 · doi ↗ · pubmed ↗