Status and predictors of parental food literacy: an Egyptian insight to highlight gaps and challenges
Iman H. Kamel, Ammal M. Metwally, Raefa Refaat Alam, Amani E. Ali, Ghada A. Elshaarawy, Safaa I. Abd El Hady, Abdelrahman K. Hassanein

TL;DR
This study examines food literacy among Egyptian parents, finding that many struggle with interactive food literacy and identifying factors like education and diet that influence it.
Contribution
The study provides new insights into food literacy gaps and predictors among Egyptian parents using a validated questionnaire and multivariate analysis.
Findings
Only 24.5% of parents achieved sufficient awareness levels for total food literacy.
Interactive food literacy was the most challenging domain, with only 18.6% of parents performing adequately.
University-level education and regular mineral intake were significant predictors of adequate food literacy.
Abstract
There is growing consensus on the importance of food literacy (FL) in public health policies and interventions globally. This study assessed parental total FL status and detected gaps. Determinants contributing to FL adequacy were identified from the socio-demographic, nutrition, and health-related characteristics. A cross-sectional study on a diverse cohort of 1000 parents (718 mothers and 282 fathers) using a validated Short FL Questionnaire (SFLQ) was conducted to assess parental total FL status. SFLQ has three sections on functional (FFL; 6 indicators), interactive (IFL; 2 indicators), and critical (CFL; 4 indicators) FL. Parents were selected using multistage stratified random sampling from four governorates representing Egypt’s diverse geographic and socioeconomic contexts. BMI was calculated using self-reported height and weight. The chi-square test, t-test, one-way ANOVA, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
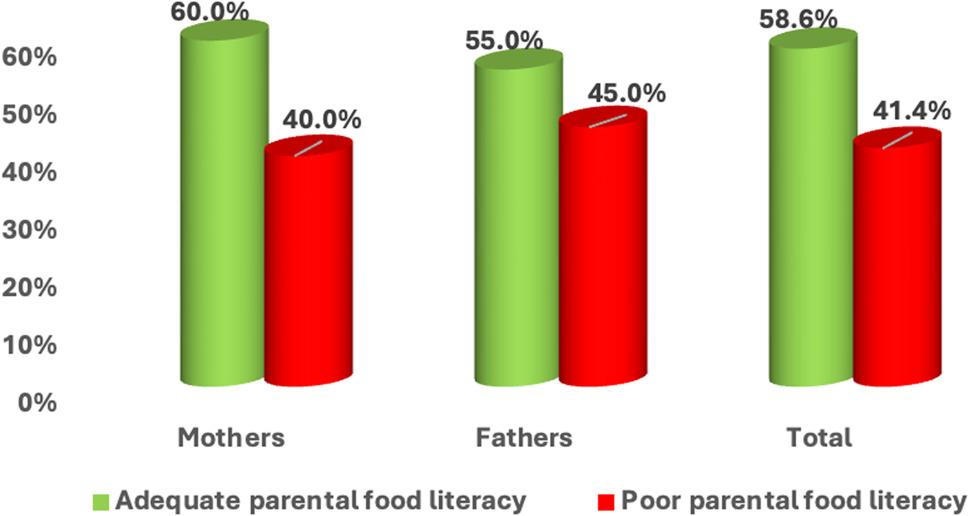 Figure 1
Figure 1- —National Research Centre Egypt
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Literacy and Information Accessibility · Obesity, Physical Activity, Diet · Food Security and Health in Diverse Populations
Introduction
The combined challenges of climate change, pollution, biodiversity loss, and the COVID-19 pandemic exacerbated by recent global crises such as Russia’s invasion of Ukraine have created a lasting cost-of-living emergency, increasing food insecurity and food prices worldwide [1]. These converging crises have not only disrupted global food systems but also heightened the urgency of improving population resilience through enhanced nutrition knowledge and behaviours [2, 3]. In this context, food literacy (FL) has emerged as a crucial determinant of individuals’ ability to make informed, sustainable, and health-promoting dietary choices, underscoring its growing recognition as a public-health priority for promoting healthier and more sustainable diets. International organizations such as the World Health Organization (WHO) and the Food and Agriculture Organization (FAO) have emphasized the need to strengthen FL to combat rising diet-related diseases and improve population dietary behaviours [4–6].
FL encompasses the knowledge, skills, and behaviours necessary to make informed food choices, plan and manage meals, and consume foods that meet individual dietary needs while supporting overall health [7–9]. Studies have linked FL to food habits, consumption patterns, and even school performance [10].
Despite global progress, malnutrition remains widespread in low and middle-income countries, including those of the Middle East and North Africa (MENA) region [11]. In Egypt, national data highlight a dual burden of under- and over-nutrition, with 7.8% of children aged 6–12 years being stunted and 8.0% overweight. Maternal education emerged as the most influential determinant for both outcomes [12, 13].
In many low- and middle-income contexts, FL remains an emerging concept [14, 15]. The scarcity of regional data underscores the urgent need to evaluate FL across diverse demographic groups to inform culturally appropriate interventions. Because parents play a central role in shaping children’s dietary behaviours, assessing their FL levels offers an actionable pathway for designing targeted strategies to improve family nutrition and reduce childhood stunting and obesity [4, 5].
While maternal influences on child feeding are well established, the paternal role in nutrition decision-making has been relatively under-explored in Egypt and similar settings. Fathers increasingly contribute to household food purchasing, budgeting, and role-modelling of eating behaviours [16, 17]. Understanding their FL is therefore essential for developing family-centred and gender-responsive interventions. Focusing on paternal FL in this study allows identification of specific gaps, behavioural patterns, and opportunities to engage fathers as equal partners in promoting household nutrition and child health.
Despite growing global recognition of FL’s importance, comprehensive assessments of parental FL in Egypt and the broader MENA region remain scarce. Most existing studies have focused on individual nutrition knowledge or maternal literacy in isolation, without examining the multidimensional nature of FL across diverse parental populations or exploring gender-specific patterns and socioeconomic determinants simultaneously. Furthermore, no previous research has systematically mapped domain-specific gaps in functional, interactive, and critical FL components among Egyptian parents, nor identified the specific indicators that pose the greatest challenges to parental nutrition competency.
Our research question was whether the prevalence of adequate TFL among Egyptian parents differs by sex, what domain-specific gaps exist across functional, interactive, and critical FL, and which socio-demographic, nutritional, and health-related factors predict adequate TFL.
We hypothesized that TFL adequacy is higher among mothers than fathers and is positively associated with higher educational attainment and healthier diet-related behaviors.
Accordingly, the present study aimed to assess parental TFL status and identify domain-specific gaps across its three core components; functional (FFL, six indicators), interactive (IFL, two indicators), and critical (CFL, four indicators) and to examine the socio-demographic, nutritional, and health-related determinants of adequate TFL among Egyptian parents; additionally, the study sought to generate evidence-based recommendations for targeted, culturally appropriate interventions to strengthen parental FL and improve family nutrition outcomes.
This study represents a large multi-governorate, community-based investigation of parental FL in Egypt, offering novel insights into gender differences, socioeconomic gradients, and the relationship between health behaviors and FL competencies, thereby filling a critical knowledge gap and establishing a foundation for evidence-informed public health policy.
Methodology
Study design and participants
A cross-sectional study was conducted on a diverse cohort of Egyptian parents to assess their FL. The sample was collected over one year, from Jan 2022 to December 2022. Eligible participants were one of the parents (mother or father) of adolescents aged 10–19 years who were present at home during the interview.
Participants were enrolled from households in the main districts of four governorates representing different geographic regions of Egypt: Cairo (Greater Cairo region), Fayoum (Upper Egypt), Al Dakahleya, Delta region), and Marsa Matrouh (Border/Frontier region). Each region has distinct dietary patterns and cultural habits. Parents were randomly enrolled during a community house-to-house survey. The household sampling frame was derived from a concurrent national screening program for children at risk of autism [18], which provided comprehensive household registries with adolescents aged 10–19 years across multiple governorates (i.e., household lists for field visits in the covered communities, not restricted to screen-positive cases). Importantly, the autism screening served only as a mechanism for household identification and did not influence parent selection or participation in the current study. All parents meeting the inclusion criteria (having at least one adolescent aged 10–19 years and being present at home during the visit) were eligible regardless of their child’s autism screening results. This approach helped ensure that the FL assessment remained independent and broadly reflective of parents in the surveyed communities rather than being restricted to families with particular health concerns.
Details of the selected governorates, localities, and socioeconomic classifications are presented in Supplementary Table S1 (Targeted Households for Parents).
Sample size and type
A sample size of 895 was calculated [19] to produce a two-sided 98% confidence interval with a distance from the mean (2%) to the limits equal to 0.700 when the estimated standard deviation is 9.0 of Egyptian parental literacy as per the finding of an Arab study [6]. with an added 15% expected loss of indicators to be answered, the sample size was 1030 targeted parents of either a mother or a father. The study sample consisted of 1,000 parents (718 mothers and 282 fathers) with the age range (25–60 and 26–65 years respectively) who completed their questionnaire. The participation rate was 95.24%, with a 4.76% declining rate of participation. 50 participants were enrolled from each social class in the targeted governorate with a total of 150 mothers or fathers per Cairo governorate and 300 per the other 3 targeted governorates. Only one of the two parents from the same house was enrolled in the study.
A multistage stratified random-sampling design was applied to ensure national representativeness. The first stage involved stratifying the sampling frame by socioeconomic status (wealth index) based on the Economic Research Forum and CAPMS classification [20], identifying three strata: low, medium, and high. Within each socioeconomic stratum, cities (Kism) in urban areas and local village units (Markaz) in rural areas were listed. From each stratum, three urban cities and three rural villages were randomly selected using a computer-generated random-number sequence.
In the second stage, within each selected locality, systematic random sampling was employed. Lists of households with adolescents aged 10–19 years were obtained from local health units and community registers in collaboration with the Ministry of Health and Population. From these lists, every household was selected using a predefined sampling interval calculated according to the total number of eligible households in each locality. For each locality, the sampling interval (k) was computed as the ratio of the total number of eligible households to the target number of households to be visited, and the locality-specific values of HH, target sample size, and k are presented in Supplementary Table S1 (Targeted Households for Parents). Within each selected household, one parent; either the mother or the father, depending on who was available was interviewed, ensuring that only one parent per household participated to maintain the independence of observations. This multistage systematic random-sampling approach ensured adequate representation of Egypt’s cultural, dietary, and socioeconomic diversity and enhanced the reproducibility of the study design.
Study tools and data collection
Data were collected through structured interviews or self-administered questionnaire. The questionnaire was designed to gather information on demographic characteristics, socioeconomic status, FL, vitamin and mineral intake, and health status. The questionnaire was administered in an average of 20 min. The questionnaire was filled in either a printed or an electronic form. Trained field workers conducted the interviews to ensure consistency and accuracy in data collection. The questionnaire was filled out online using survey monkey platform according to the following references:
Socio-demographic variables
according to Assad & Kraft, 2012: Data collected on age, gender, education level, marital status, number of children, employment status, monthly income, and household crowding index [21–23]. The household crowding index was calculated as the number of co-residents (excluding newborns) divided by the number of rooms (excluding kitchens and bathrooms).
Health status
Chronic diseases were assessed through self-reported data. Participants were asked if they had been diagnosed with any chronic conditions with special emphasis on diabetes, hypertension, or cardiovascular diseases. Vitamin and mineral intake were assessed through self-reported binary questions regarding regular use of dietary supplements. Participants were asked whether they regularly consumed vitamin supplements (including vitamins A, C, D, B12, and folic acid) and mineral supplements (including calcium, iron, magnesium, and zinc) with yes/no response options. This assessment reflected supplement use only and did not quantify daily intake amounts, evaluate dietary sources, or assess adequacy against recommended dietary allowances.
FL
Parental FL was assessed using a validated FL questionnaire, which included sections on functional, interactive, and critical FL. The Arabic version of the short FL questionnaire (SFLQ) according to Gréa Krause et al. 2020 and Koca and Arkan 2020 were used for parental FL (FL) assessment [24, 25], The Arabic version of the questionnaire that was adapted to the local context was used before by Hoteit and her colleagues [6] in a multi-country Arab population sample that included Lebanese, Jordanian, and other MENA populations. However, it had not been specifically validated among Egyptian parents prior to this study. Therefore, we re-tested internal consistency in our sample. The SFLQ demonstrated good internal consistency with Cronbach’s alpha values of 0.79 (total scale), 0.74 (functional), 0.71 (interactive), and 0.76 (critical). These findings support the scale’s internal consistency and usability in the present Egyptian parent population. In addition, the questionnaire was reviewed by three Egyptian nutrition experts and piloted with 30 parents (excluded from the final analysis) to ensure cultural appropriateness and comprehension. We also added a limitation noting that future work should conduct comprehensive psychometric validation in Egypt (e.g., construct validity and test–retest reliability).
FL questionnaire was used to evaluate the parents’ ability to follow national and international sources regarding food information and apply this information in their daily lives to promote healthier eating behaviors. It includes 12 indicators with three FL dimensions: functional FL (FFL; 6 indicators), interactive FL (IFL; 2 indicators), and critical FL (CFL; 4 indicators). Each question has a score range of 4- or 5-point Likert scale: strongly disagree to strongly agree and a higher score indicates better FL. The scoring criteria of the parental FL range from 7 to 52 with an average score ≥ 36. Moreover, the FFL sub-dimension assesses the parents’ food practical skills and knowledge. The IFL sub-dimension explores the parents’ ability to participate in discussions and make decisions about food choices for their entire family. While CFL sub-dimension focuses on parents’ critical thinking skills related to food and nutrition. Scores were calculated for each section and an overall FL score was derived.
The indicators under each component of parental FL are as follows
Six indicators (5 awareness and one practice) under the FFL include: Knowing where one can get the information needed when having indicators or concerns about proper nutrition; Understanding nutritional information presented in the form of leaflets (e.g., labels, brochures), nutritional facts labeled on food products, nutrition programs on television or radio, dietary recommendations from nutrition professionals, or nutritional advice from family members or friends; Knowing the food pyramid well; Awareness of the official recommendations regarding fruit and vegetable consumption; Awareness of the official recommendations regarding salt consumption in food; Difficulty of preparing a complete meal with nutrients (such as proteins, starches, healthy fats, and vegetables).
The IFL includes two indicators
The ability to help a family member or friend with indicators about nutrition; and the ability to select the information about proper nutrition that seems right and relevant.
The CFL includes four indicators: Difficulty in evaluating the reliability of nutritional information found on websites or transmitted through the media (internet, social media, television, radio…); Difficulty in evaluating the validity of the advertisements that may link certain food products to how they affect health; Difficulty in determining whether a certain food fits with a healthy diet; Difficulty in evaluating how your current eating choices and habits affect your long-term health.
Body Mass Index (BMI)
BMI was calculated using self-reported height and weight. Participants were categorized into underweight, normal weight, and overweight/obese based on the World Health Organization (WHO) BMI classification. The BMI was calculated as weight (in kilograms) divided by height (in meters) squared based on the WHO growth standards with the help of the Anthro-Program of PC [26]. The classification of Parents’ BMI was as follows: underweight if BMI is less than 18.5, normal/healthy weight if BMI is 18.5 to 24.9, overweight if BMI is 25.0 to 29.9, and obese if BMI is 30.0 or higher [27].
Data processing
The studied participants were classified into four categories according to their acquired score in each component of FL: ≤25%, > 25%- 50%, > 50%- 75%, and > 75%. The total food-literacy score was calculated by summing responses across all 12 indicators of the SFLQ, with possible scores ranging from 7 to 52 points. Based on the validated scoring criteria for the Arabic version of the SFLQ, parents were categorized into two outcome groups: adequate food literacy (FL) (total score ≥ 36) and poor FL (total score < 36). This cut-off enables a clear distinction between parents who achieve a satisfactory level of FL and those requiring targeted interventions. The awareness level of each indicator will determine the objectives to be achieved to increase awareness of the FL set of indicators. When 50% or more participants were unaware of one or more Indicators, this set of indicators is a gap and challenging to achieve. According to the assessment results, the target objectives were set to be realistic and achievable: For any indicator whose measure was 50% or less, the target has to reach 75%. For any indicator measuring > 50% to 75%, the target will be set to reach > 70–80%. For any indicator measuring > 75%, the target is to sustain the indicator. The total FL score was calculated by summing responses across all 12 indicators of the SFLQ, with possible scores ranging from 7 to 52 points. Based on the validated scoring criteria for the Arabic version of the SFLQ, parents were categorized into two groups [6]: adequate FL (total score ≥ 36) and poor FL (total score < 36). This dichotomization allows for clear identification of parents who have achieved a satisfactory level of FL versus those who require targeted interventions.
Statistical analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 26.0 [28]. Frequency and percentages were computed for comparisons between qualitative variables. Continuous data was expressed as mean and standard deviation (SD). Pearson’s chi-square test (χ²), Fisher’s exact test, and Z test were used for qualitative comparisons, while independent t-tests and one-way ANOVA were used to compare mean values across groups.
To evaluate the degree of association between parental BMI, vitamin and mineral intake, and FL, odds ratio (OR) with 95% confidence interval (CI) were calculated. These variables were examined bidirectionally; both as correlates and predictors to explore their associative relationships with FL rather than implying causation. Multivariable logistic regression analysis was performed to identify the significant predictors of adequate total parental FL among the studied parents. Missing values were handled using complete-case (listwise) deletion within each analysis, and denominators are presented as available. For multivariable modelling, predictors with zero-cell counts or no meaningful variability (i.e., complete or quasi-complete separation) were not entered into the regression model; accordingly, job status was excluded because all fathers were employed, making this variable non-informative and highly collinear with gender. Potential multicollinearity among predictors was assessed using variance inflation factor (VIF) and tolerance values. All variables demonstrated acceptable collinearity thresholds (VIF < 2.5; tolerance > 0.4), confirming the absence of significant multicollinearity. A p-value < 0.05 was considered statistically significant.
Results
Demographic characteristics, socioeconomic factors, health status, and nutritional supplementation
Of the targeted eligible sample, 1,000 parents completed the interview (participation rate: 95.24%), while 50 parents declined participation (4.76%). Table 1 presents the characteristics of the 1,000 participating parents, stratified by gender and organized into three thematic domains.
Table 1. Parental socio-demographic, health, and nutrition status characteristics according to genderVariablesMothers(n=718; 71.8%)n (%)Fathers(n=282; 28.2%)n (%)P valueAge by years (mean ± SD)42.2 ± 6.347.5 ± 5.4<0.001Marital status Married611 (85.1)275 (97.5)<0.001 Not married (Divorced or Widowed)107 (14.9)7 (2.5)Number of children ≤ 3 children638 (88.9)260 (92.2)0.116 > 3 children80 (11.1)22 (7.8)Household crowding index^§^ Not crowded (≤ 1)513 (71.4)76 (27.0) <0.001** Crowded (> 1)205 (28.6)206 (73.0)Education level Never attend school9 (1.3)29 (10.3)<0.001** School level114 (15.9)97 (34.4) University level595 (82.9)156 (55.3)Job-status Not employed50 (7.0)0 (0.0)<0.001** Employed (Full-time job, Part-time job,668 (93.0)282 (100.0) Self-employed)Monthly income Less than 5000 EP100 (35.5)172 (61.0)<0.001** 5000- 10000 EP72 (25.5)55 (19.5) More than 10000 EP110 (39.0)55 (19.5)History of chronic diseases No226 (31.5)147 (52.1)<0.001** Yes492 (68.5)135 (47.9)Weight status (BMI) Underweight13 (1.8)1 (0.4) 0.038* Normal-weight206 (28.7)99 (35.1) Overweight / obese499 (69.5)182 (64.5)Vitamin Intake No489 (68.1)139 (49.3) <0.001** Yes229 (31.9)143 (50.7)Mineral Intake No551 (76.7)236 (83.7)0.016* Yes167 (23.3)46 (16.3)§Household crowding index = number of co-residents (excluding newborns) ÷ number of rooms (excluding kitchens and bathrooms) [22, 23]. Test of significance: χ² test, Fisher’s exact test, and t-test between two means*Significance levels: p < 0.05 (significant); **p < 0.01
Sociodemographic profile
Most parents were aged ≥ 40 years (59.1%), with mothers representing 61.8% of participants. Most mothers were employed (93.0%), while all fathers were employed (100.0%); only 7.0% of mothers reported not being employed (p < 0.001). University education was reported by 82.9% of mothers and 55.3% of fathers (p < 0.001). The majority of families belonged to the medium socioeconomic category (56.3%) and lived in non-crowded households.
Health-related characteristics
Chronic diseases were significantly more prevalent among mothers (68.5%) than fathers (47.9%, p < 0.001). Overweight and obesity were common in both groups, affecting 69.5% of mothers and 64.5% of fathers (p = 0.038).
Nutritional supplementation
Nutritional Supplementation: Fathers reported higher vitamin supplement use than mothers (50.7% vs. 31.9%, p < 0.001), while mineral supplement intake was higher among mothers than fathers (23.3% vs. 16.3%, p = 0.016).
Figure 1 shows the distribution of parental food literacy (FL) by gender based on the total Short Food Literacy Questionnaire (SFLQ) classification (adequate FL ≥ 36; poor FL < 36). Overall, 58.6% of parents demonstrated adequate FL and 41.4% had poor FL (descriptive). Adequate FL was 60% among mothers and 55% among fathers. The difference in the prevalence of adequate FL between mothers and fathers was assessed using a Z test for two proportions (p = 0.15).
Fig. 1. Percent distribution of parental total FL (SFLQ score categories: adequate ≥ 36; poor < 36) according to gender. Test of significance: Z test between two proportions comparing the prevalence of adequate FL between mothers and fathers (p = 0.15)
Mean scores and awareness levels of FL components
Female parents consistently scored significantly higher across all FL components (all p < 0.001): FFL (17.6 ± 3.7 vs. 15.9 ± 4.3), IFL (6.6 ± 2.4 vs. 5.8 ± 2.1), CFL (12.0 ± 2.5 vs. 10.4 ± 3.1), and total FL (36.2 ± 7.8 vs. 32.1 ± 9.0). Overall, only 24.5% of parents achieved sufficient awareness for total FL. Component-specific analysis revealed that awareness remained limited for FFL (20.4% sufficient), IFL (18.6% sufficient), and CFL (20.3% sufficient). Examination of individual indicators highlighted that more than half of the parents exhibited poor awareness in several domains (Table 2). Within the IFL component, 62.4% were unaware of how to select appropriate nutrition information, and 68.3% lacked the ability to help family or friends with such information, indicating weak communication and information-sharing skills. For FFL, three of six indicators were identified as challenging: understanding nutritional facts on food labels (68.8% unaware), knowing where to obtain reliable nutrition information (61.2% unaware), and knowledge of the food pyramid (56.1% unaware). By contrast, CFL showed comparatively better performance, with most indicators falling in the neutral range (25–50% unaware) and one indicator in the sufficient range (< 25% unaware), reflecting relatively stronger evaluation and judgment skills. Collectively, these results underscore that parents possess higher critical reasoning than functional or interactive competencies, emphasizing the need for interventions that strengthen practical nutrition comprehension and application within households.
Table 2. Awareness indicators level of components of parental FLDeterminants#Parental total FL(n=1000) n (%)Challenging category (> 50% were unaware):FFL component include: 1. Knowing where one can get the information needed when having concerns about proper nutrition.612 (61.2) 2. Understanding nutritional information and facts presented in leaflets, on television or radio, from nutrition professionals, or from family members or friends. 688 (68.8) 3. Knowing the food pyramid well.561 (56.1)IFL sub-dimension includes: 4. The ability to help a family member or friend with information about nutrition. 683 (68.3) 5. The ability to select the information about proper nutrition that seems right and relevant. 624 (62.4)Neutral category (25-50% were unaware or inexperienced):FFL sub-dimension includes: 6. Awareness of the official recommendations regarding fruit and vegetable consumption 345 (34.5) 7. Awareness of the official recommendations regarding salt consumption in food 357 (35.7) 8. Difficulty of preparing a complete meal with nutrients (such as proteins, starches, healthy fats, and vegetables 330 (33.0)CFL sub-dimension includes: 9. Difficulty in evaluating the reliability of nutritional information found on websites or transmitted through the media (internet, social media, television, radio... 310 (31.0) 10. Difficulty in evaluating the validity of the advertisements that may link certain food products to how they affect health. 275 (27.5) 11. Difficulty in determining whether a certain food fits with a healthy diet;285 (28.5)Sufficient category (<25% were unaware or inexperienced):CFL sub-dimension includes: 12. Difficulty in evaluating how your current eating choices and habits affect your long-term health245 (24.5)# Determinants refers to the individual FL indicators/items assessed within each domain (FFL/IFL/CFL) and categorized by the proportion of parents reporting being unaware/inexperienced (challenging/neutral/sufficient)
Correlates of FL components
As shown in Table 3, age, gender, family structure, socioeconomic status, and nutritional supplementation showed significant associations with multiple FL domains. Parents aged ≥ 40 years had higher CFL scores (11.7 ± 2.8 vs. 11.1 ± 2.6, p = 0.011), while female parents consistently scored higher across all components (all p < 0.001). Larger family size (> 3 children) and lower crowding indices were associated with better functional and interactive FL (p < 0.05 and p < 0.001, respectively).
Educational attainment and income level demonstrated strong positive gradients—university-educated and higher-income parents achieved significantly higher FL scores across all components (all p < 0.001).
Unemployed parents also exhibited higher FL scores than employed parents (all p < 0.001), suggesting greater availability for food-related tasks.
Although chronic disease presence did not significantly influence FL, overweight and obese parents displayed higher scores across components (all p < 0.05).
Regular vitamin and mineral supplement use was strongly associated with improved FL in all domains (all p < 0.001). These findings collectively highlight the influence of socioeconomic and lifestyle factors on parental FL, underscoring the role of education, income, and household environment in shaping FL outcomes.
Table 3. Correlates of the epidemiological factors and supplement intake with parental FL componentsVariablesFFL^(a)^(n=1000)(mean ± SD)IFL^(b)^(n=1000)(mean ± SD)CFL^(c)^(n=1000)(mean ± SD)Total FL^(d)^(n=1000)(mean ± SD)Age group < 40 years16.9 ± 3.66.1 ± 2.111.1 ± 2.634.1 ±7.9 ≥ 40 years17.2 ± 4.06.4 ± 2.411.7 ± 2.835.3 ± 8.4 P value0.3640.1610.0110.094Gender Female17.6 ± 3.76.6 ± 2.412.0 ± 2.536.2 ± 7.8 Male15.9 ± 4.35.8 ± 2.110.4 ± 3.132.1 ± 9.0 P value<0.001**<0.001**<0.001**<0.001**Marital status Married17.1 ± 3.96.4 ± 2.311.6 ± 2.835.1 ± 8.2 Not married (Divorced or Widowed17.1 ± 4.46.2 ± 2.611.4 ± 3.034.7 ± 9.2 P value0.8350.4980.4580.590Number of children in the household ≤ 3 children 17.1 ± 3.96.3 ± 2.411.5 ± 2.834.9 ± 8.5 > 3 children17.9 ± 3.87.0 ± 1.711.9 ± 2.136.8 ± 6.5 P value0.0430.0010.0530.026*Household crowding index^§^ Not crowded (≤ 1)17.6 ± 3.96.5 ± 2.612.0 ± 2.736.1 ± 8.3 Crowded (> 1)16.5 ± 4.06.2 ± 2.010.9 ± 2.833.6 ± 8.2 P value<0.0010.061<0.001**<0.001Education level School level15.5 ± 3.55.6 ± 2.010.4 ± 2.731.5 ± 7.5 University level or higher17.9 ± 3.66.7 ± 2.412.2 ± 2.436.8 ± 7.5 P value<0.001<0.001**<0.001**<0.001Job status Not employed20.5 ± 4.47.3 ± 2.213.1 ± 2.540.8 ± 8.3 Employed (Full-time job, Part-time job, Self-employed)17.0 ± 3.8 6.3 ± 2.4 11.5 ± 2.8 34.8 ± 8.2 P value<0.0010.004**<0.001**<0.001Monthly income Less than 5000 EP15.5 ± 4.45.5 ± 2.410.1 ± 3.431.1 ± 9.5 More than 5000 EP17.5 ± 3.76.6 ± 2.311.9 ± 2.536.0 ± 7.7 P value<0.001<0.001**<0.001**<0.001Parent has one or more chronic disease. No17.2 ± 4.06.4 ± 2.011.4 ± 2.635.0 ± 7.9 Yes17.1 ± 3.96.3 ± 2.511.7 ± 2.935.1 ± 8.6 P value0.5650.4780.1080.948Weight status (BMI) UnderweightNormal weight16.1 ± 2.316.7 ± 4.85.7 ± 0.66.0 ± 2.411.1 ± 1.610.8 ± 3.333.0 ± 3.733.4 ± 10.0 Overweight/obese17.4 ± 3.56.5 ± 2.411.9 ± 2.535.8 ± 7.4 P value0.025*0.001<0.001**<0.001Vitamin Intake No16.6 ± 4.25.9 ± 2.511.1 ± 2.933.6 ± 8.8 Yes18.1 ± 3.37.1 ± 2.012.4 ± 2.437.6 ± 6.7 P value<0.001<0.001**<0.001**<0.001Mineral Intake No16.6 ± 3.96.0 ± 2.311.2 ± 2.733.8 ± 8.2 Yes19.0 ± 3.37.7 ± 2.213.1 ± 2.639.7 ± 7.0 P value<0.001<0.001**<0.001**<0.001**§Household crowding index = number of co-residents (excluding newborns) ÷ number of rooms (excluding kitchens and bathrooms) [22, 23]. Test of significance: t-test between two means and ANOVA between groups. *Significance levels: * p < 0.05; **p < 0.01), (a) Functional FL; (b) Interactive FL; (c) Critical FL; (d) Total FL
Associations between parental FL and health-related factors
As shown in Table 4, parents with poor FL were significantly more likely to be underweight (OR = 3.3, 95%CI: 0.9–12.0), whereas those with adequate FL were more frequently overweight or obese (OR = 0.5, 95%CI: 0.4–0.6, p < 0.01). Poor FL was also associated with lower supplement use: non-use of mineral supplements (OR = 3.8, 95%CI: 2.6–5.5, p < 0.01) and vitamin supplements (OR = 2.4, 95%CI: 1.5–3.2, p < 0.01).
Table 4. Bivariate associations between parental TFL and selected health-related variablesVariablesStudied parents (n=1000)BMIVitamins intakeMinerals intakeUnderweight n= 14, n (%)Overweight/ Obese n= 681, n (%)Normal weight n= 305, n (%)No n=628 n (%)Yes n=372 n (%)No n=787 n (%)Yes n=213 n (%)Parental FL Poor (n=414)11 (78.6) 242 (35.5) 161 (52.8) 308 (49.0) 106 (28.5) 373 (47.4) 41 (19.2) Adequate (n=586)3 (21.4)439 (64.5)144 (47.2)320 (51.0)266 (71.5)414 (52.6)172 (80.8)OR(95% CI)3.3(0.9-12.0)0.5(0.4-0.6) **2.4 (1.5-3.2) **3.8 (2.6-5.5) **Test of significance: χ² test and odds ratio (OR) with 95% confidence interval (CI), Significance levels: * p < 0.05; **p < 0.01)
Predictors of adequate FL
Table 5 presents the multivariable logistic regression model (enter method) examining independent predictors of adequate TFL among parents. The model demonstrated a good overall fit (χ² = 98.4, p < 0.001; Nagelkerke R² = 0.42). Using the table’s stated reference categories (< 40 years, female, married, ≤ 3 children, not crowded (≤ 1), school education, not employed, income < 5000 EGP, normal-weight), four variables remained statistically significant in the adjusted model. Parents aged ≥ 40 years had higher odds of adequate TFL compared with those < 40 (AOR = 1.59, 95%CI: 1.09–2.32, p = 0.016). Parents with university education or higher were more likely to demonstrate adequate TFL than those with school education (AOR = 2.67, 95%CI: 1.82–3.92, p < 0.001). Living in a crowded household (> 1) was associated with higher odds of adequate TFL compared with not crowded households (AOR = 1.52, 95%CI: 1.06–2.17, p = 0.012). Regarding weight status, overweight/obesity was associated with higher odds of adequate TFL versus normal weight (AOR = 1.62, 95%CI: 1.19–2.21, p = 0.002), while underweight was not significant (p = 0.799). Mineral intake showed a strong positive association with adequate TFL (AOR = 3.97, 95%CI: 2.49–6.33, p < 0.001), whereas vitamin intake was not significant (p = 0.859). Gender, marital status, number of children,, monthly income, and having ≥ 1 chronic disease were not significant predictors in the multivariable model (all p > 0.05).
Table 5. Multivariable logistic regression model for prediction of adequate parental TFLVariablesβAORP value95% CI for AORLowerUpperAge group < 40 years (ref.)1 ≥ 40 years0.4651.5920.0161.0922.321Gender Females (ref.)1 Males0.1521.1640.4340.7961.702Marital status Married (ref.)1 Not married (Divorced or Widowed)0.1450.1560.5500.7181.860Number of children in the household ≤ 3 children (ref.)1 > 3 children0.1721.1880.5030.7181.968Household crowding index Not crowded (≤ 1) (ref.)1 Crowded (> 1)0.4191.5200.0121.0642.173Education level School level (ref.)1 University level or higher0.9812.667<0.0011.8163.916Monthly income Less than 5000 EP (ref.)1 More than 5000 EP0.3401.4050.1490.8852.231Parent has one or more chronic disease No (ref.)1 Yes-0.1030.9020.5480.6451.262Weight status (BMI) Normal-weight (ref.)1 Underweight-02100.8100.7990.1614.089 Overweight/obese0.4831.6210.0021.1872.213Vitamins intakeNo (ref.) No1 Yes-0.0340.9660.8590.6611.411Minerals intake No (ref.)1 Yes1.3793.970<0.0012.4886.333Constant0.000Variable(s) entered in each model: age, gender, BMI, education level, marital status, number of children, job status, monthly income, household crowding index, one or more chronic diseases, vitamin intake, and mineral intake. Test of significance: Binary logistic regression model.AOR Adjusted Odds Ratio,CI Confidence Interval, (ref.) indicates the reference category (AOR = 1.00) as labelled in the table. Significance levels: p < 0.05; p < 0.01)
Discussion
This study provides the first comprehensive assessment of parental FL in Egypt, identifying key gaps, strengths, and determinants across a diverse population sample. The analysis revealed clear gender-specific differences, distinctive behavioural patterns in supplement use, and multifactorial relationships between sociodemographic characteristics, health status, and FL adequacy. These insights carry important implications for developing targeted, evidence-based interventions aimed at enhancing nutritional knowledge, decision-making, and healthy behaviours among Egyptian parents.
FL awareness level
The present study revealed that only 24.5% of parents achieved sufficient awareness of TFL, while more than half demonstrated limited understanding of its functional and interactive dimensions. IFL showed the weakest performance, with over 60% of parents reporting difficulty in selecting appropriate nutrition information or assisting others in interpreting it. This pattern underscores substantial gaps in practical and communication-based nutrition competencies among Egyptian parents.
Comparable findings have been reported in regional studies showing that individuals often possess basic nutritional knowledge but lack the capacity to apply or communicate it effectively [29–32]. In our context, limited access to culturally tailored educational materials and a scarcity of family-cantered nutrition programs may contribute to this gap. In line with previous research from Egypt and other MENA countries [30, 33, 34], the present results highlight that functional literacy (reading labels, identifying nutrient content) remains insufficient, while critical evaluation skills are relatively better developed.
These results have direct implications for intervention design. Public health initiatives should prioritize improving parents’ practical food-handling and interpretation skills through community-based workshops and school-linked programs that emphasize the everyday application of nutrition information [30, 33–35]. Integrating FL modules into school curricula and primary healthcare counselling has been shown to strengthen both functional and interactive competencies and to enhance nutrition-related decision-making at the household level [36–38]. Tailored interventions should also consider gender and socioeconomic differences observed in this population to ensure equitable reach and impact, as earlier studies have underscored the modifying role of these determinants in shaping FL and dietary behaviours [6, 39–42]. A comprehensive scoping review of food and nutrition literacy programs published in 2023 also highlighted the effectiveness of various educational initiatives in improving FL [43].
FL status
There are some controversial results about gender literacy. Our findings align with previous studies indicating that women generally have higher levels of nutritional knowledge and food literacy compared to men [6, 39–47]. Women were also reported to be better at critically assessing the reliability and validity of nutritional information compared to men [29]. It was found that women were more likely to engage in discussions about nutrition and seek out nutritional information compared to men [46]. However, other studies did not find gender differences in food literacy [42, 48].
However, when adjusting for potential confounders, the strength of these associations shifted. Although female parents demonstrated higher mean scores for functional, interactive, and critical food literacy components in the bivariate analysis, gender did not retain statistical significance as an independent predictor of TFL in the multivariable regression model. This attenuation suggests mediation by socioeconomic variables—particularly education, employment, and household income. Similarly, several other variables that showed significant bivariate associations (e.g., BMI and supplement use) lost significance in the adjusted model, indicating potential confounding by socioeconomic position and access to nutrition information.
The documented gender difference in our study may also reflect traditional gender roles, where women often take primary responsibility for food preparation and nutrition within households. These findings underscore the importance of gender-sensitive educational strategies that empower both parents to strengthen their FL and promote equitable household nutrition decisions.
Health-related correlates of FL
Both nutritional supplement intake and weight status were strongly related to FL, functioning as both predictors and outcomes. Fathers reported higher vitamin supplement use than mothers (50.7% vs. 31.9%, p < 0.001), while mineral supplement intake was also slightly higher among fathers (16.3% vs. 23.3%, p = 0.016. These findings align with research demonstrating that supplement use reflects greater nutrition awareness and self-efficacy [49–51].
Interestingly, the study found that both overweight/obese and unemployed parents exhibited higher FL levels than their counterparts, findings that appear counterintuitive at first glance. In the case of overweight and obese parents, this relationship may reflect heightened health awareness and self-monitoring behaviours following exposure to medical advice, dietary counselling, or chronic disease risk awareness. This could enhance FL without necessarily translating into behavioural change or weight loss. Several studies have similarly reported that individuals with diet-related conditions often acquire greater nutrition knowledge through treatment or self-education, yet struggle with sustained dietary adherence or lifestyle modification [6, 50, 51].
Likewise, unemployed parents demonstrated higher FL scores than employed counterparts. This may be explained by increased time availability, greater involvement in meal planning and preparation, or caregiving responsibilities; especially among mothers allowing more opportunities to apply FL skills. Similar observations have been reported in population-based studies where greater time for food-related activities was associated with improved FL, cooking confidence, and dietary diversity [52–54]. Alternatively, this finding could also indicate that employment constraints and time scarcity among working parents reduce opportunities to apply or practice FL skills in daily life, a pattern supported by prior research on time-related barriers to healthy food behaviours [55, 56].
Thus, while unemployment may coincide with higher FL scores, it does not necessarily imply healthier overall lifestyles, emphasising the need for workplace-based nutrition education and time-efficient strategies that enable employed parents to maintain adequate FL and dietary quality. Moreover, higher FL does not always equate to healthier dietary practices or optimal body weight. Instead, they highlight the complex interplay between knowledge, behaviour, and contextual constraints emphasizing the need for integrated interventions that combine FL education with behavioural and environmental supports to facilitate healthier outcomes.
Socioeconomic determinants of FL
The findings of our study highlight the multifaceted nature of FL and the influence of demographic and socioeconomic factors. Education, income, employment status, and household conditions collectively shaped parental FL levels, confirming similar global trends [57–60]. Parents aged 40 years and above had significantly higher mean scores for CFL compared to those under 40 years, reflecting greater experience and exposure to health information over time [40, 41]. Likewise, parents with a university-level education or higher exhibited substantially higher FL scores across all domains. Education remained the strongest independent predictor in the regression model (AOR = 2.67; 95%CI: 1.82–3.91), reinforcing its critical role in shaping health literacy globally [57–60].
Monthly income and employment status were significantly associated with FL in the bivariate analysis but not as independent predictors after adjustment, suggesting that education mediates their influence. The relationship between household crowding and FL presented an intriguing pattern: while bivariate analyses showed lower FL scores among larger households, regression analysis revealed that moderate crowding predicted higher odds of adequate FL (AOR = 1.52; 95%CI: 1.03–2.24). This reversal likely reflects the confounding effect of socioeconomic status—smaller households in our sample were also more affluent and highly educated. After adjustment, the positive association suggests that shared living environments may foster collective food-related learning, intergenerational knowledge transfer, or improved resource management, all of which can enhance FL [14, 61–63].
The domain-specific patterns observed in this study provide insight into how identified determinants shape different facets of FL. Higher educational attainment was most strongly associated with better interactive and critical food literacy. This supports evidence that education enhances individuals’ capacity to interpret, communicate, and evaluate nutrition information rather than simply recall it [61, 64, 65]. Conversely, parents with lower education may possess basic functional skills yet lack the confidence or communication strategies needed to discuss nutrition effectively with family members. This explains the particularly low IFL scores observed in this group. Moreover, mineral-supplement users scored higher across all domains, possibly reflecting greater exposure to health counselling, medical advice, or self-directed information seeking, which reinforces interactive and critical competencies [52, 66, 67]. These findings indicate that interventions targeting at-risk groups; such as less-educated parents or those with limited healthcare engagement should prioritize interactive skills, including how to locate, discuss, and translate nutritional information into practical household behaviours.
Implications for public health policy
The findings of this study have significant implications for strengthening public health strategies in Egypt and similar middle-income contexts. Enhancing parental FL requires a multi-level approach that combines education, community engagement, and supportive policy frameworks.
At the program level, interventions should integrate FL training into primary healthcare and school-based programs, expand community learning initiatives, and design gender-responsive modules that empower both mothers and fathers as active nutrition gatekeepers [38, 57, 59, 68–70]. Given that fathers in this study reported higher supplement use but lower FL scores, male-focused awareness and counselling programs could effectively bridge behavioural–knowledge gaps and promote shared responsibility for family nutrition [33, 46, 71–74].
At the policy level, FL should be mainstreamed within national nutrition and health promotion agendas through intersectoral collaboration among the Ministries of Health, Education, and Social Solidarity. Policymakers should ensure equitable access by prioritizing low-income and less-educated families [2, 38, 57, 75] and incorporating FL indicators into national monitoring systems to evaluate progress [36–38].
At the household and community levels, improving parental FL can generate intergenerational benefits—parents with higher FL are more capable of modelling healthy eating, guiding children’s food choices, and fostering dietary diversity [49, 61, 63, 66]. Evidence from Egyptian adolescents also confirms that adequate parental FL substantially increases adolescent nutrition literacy and micronutrient adequacy, underscoring the importance of family-cantered and life-course-oriented interventions [43].
Beyond its individual and household-level importance, parental FL exerts a critical intergenerational influence on children’s nutrition literacy, dietary diversity, and health behaviours. Parents with higher FL demonstrate better capacity to model healthy eating, structure balanced meals, and guide children’s food choices, thereby improving adolescents’ Total Nutrition Literacy and related health outcomes [69]. Evidence from Egyptian adolescents shows that adequate parental FL nearly doubled the odds of achieving adequate TNL and significantly increased vitamin and mineral intake, confirming its pivotal role in shaping youth dietary outcomes. These findings underscore the need for family-cantered nutrition-education policies that empower both mothers and fathers as co-educators and role models in promoting healthy eating patterns across generations.
Strengthening FL across these levels can ultimately contribute to healthier dietary behaviours, improved nutrition outcomes, and the reduction of Egypt’s dual burden of undernutrition and obesity [12, 13, 33, 35, 76].
Strengths and limitations
This study, while providing valuable insights into the factors influencing parental FL, among Egyptian parents, has some limitations that should be acknowledged: First, its cross-sectional design precludes establishing causal relationships between FL and its associated variables. Accordingly, variables such as BMI, vitamin intake, and mineral intake were analysed as correlates rather than direct outcomes or causes of FL. The observed associations should therefore be interpreted as descriptive and associative, not causal. The use of an autism screening program’s household registry as a sampling frame did not introduce systematic bias, as parent selection was independent of screening outcomes and based solely on the presence of adolescents in the household.
The reliance on self-reported data for assessing FL and dietary supplement intake may introduce bias, potentially leading to overestimation or underestimation of responses.
Although the FL questionnaire was validated and culturally adapted, it may not have captured the full spectrum of FL dimensions. Similarly, vitamin and mineral intake was assessed through simple self-reported supplement use rather than comprehensive dietary tools, limiting the ability to evaluate total nutrient intake and adequacy. Future studies should employ validated dietary assessment instruments, such as food frequency questionnaires or repeated 24-hour dietary recalls, to generate more accurate nutrient profiles. Although the SFLQ demonstrated good reliability in our sample (Cronbach’s α = 0.79), future research should conduct comprehensive validation studies including construct validity and test-retest reliability specifically for the Egyptian context.
Despite the use of a multistage stratified random sampling approach to ensure representation across Egypt’s main regions and socioeconomic strata, participation depended on the availability of one parent during household visits; typically, the parent present at home during daytime hours which may have introduced minor selection bias, particularly underrepresenting employed fathers. Nevertheless, the probabilistic sampling design and large sample size helped mitigate this limitation. Additionally, several potentially confounding variables, such as physical activity levels, detailed dietary patterns, and broader lifestyle behaviours, were not assessed and may have influenced the observed associations. Future longitudinal studies incorporating these variables could better clarify causal pathways and contextual determinants of FL among Egyptian parents.
Despite these limitations, the study has several notable strengths. It is the first nationally representative investigation of parental FL in Egypt, encompassing diverse geographic, cultural, and socioeconomic contexts. The multistage stratified design enhanced representativeness and generalizability of the findings across Egypt’s population.
This study also provides the first empirical mapping of specific gaps in parental FL indicators; particularly functional and interactive competencies thereby offering actionable insights for targeted public health interventions. Furthermore, the large sample size and comprehensive analytic approach, including multivariable regression modeling, enabled robust identification of key predictors of FL.
Key determinants identified; such as age, educational attainment, mineral supplement intake, and overweight/obesity highlight the multidimensional nature of FL and its links to both sociodemographic and health-related factors. Collectively, these insights establish a strong foundation for designing culturally tailored, gender-responsive, and cost-effective strategies to strengthen parental FL and promote healthier family nutrition practices in Egypt.
Conclusions and recommendations
In conclusion, this study provides the first comprehensive assessment of parental FL in Egypt, revealing that while 58.6% of parents demonstrated adequate overall FL, substantial gaps persist in interactive and functional domains. Mothers consistently outperformed fathers across all FL dimensions; however, this difference was largely explained by educational and socioeconomic factors rather than gender alone. The most critical gaps were related to difficulties in selecting appropriate nutrition information, assisting others with dietary decisions, interpreting nutrition labels, and identifying reliable sources of information.
Interestingly, adequate FL was positively associated with overweight and obesity. This suggests that increased nutritional awareness does not automatically translate into healthier weight outcomes. This pattern may reflect greater health consciousness among overweight individuals or barriers that hinder the practical application of nutrition knowledge in daily life. Hence, improving FL alone may not be sufficient to prevent obesity unless accompanied by behavioural, structural, and environmental supports.
Improving parental FL therefore requires multifaceted, equity-oriented interventions that enhance practical food-handling, label-reading, and communication skills while addressing structural and time-related barriers to healthy eating. Educational programs targeting fathers and younger parents, as well as community-based and workplace initiatives, could yield sustainable improvements in household nutrition.
Integrating FL education into school curricula and primary healthcare systems will promote intergenerational learning and empower families to make informed food choices. By fostering both knowledge and supportive environments, policymakers can help translate awareness into action, thereby advancing progress toward healthier diets and reducing Egypt’s dual burden of undernutrition and obesity.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1UN DESA. The Sustainable Development Goals Report 2023: Special Edition - July 2023. New York, USA: UN DESA. 2023. Available from: https://unstats.un.org/sdgs/report/2023/. Accessed 2024 August 22.
- 2UNICEF Middle East and North Africa Regional Office. Nutrition Strategic Direction 2030: MENA region. UNICEF MENA; 2024. Available from: https://www.unicef.org/mena/media/25906/file/Nutrition%20Strategic%20Direction%202030%20MENA%20Main%20Document.pdf%20.pdf. cited 08 Nov 2025.
- 3World Health Organization. Physical Status: The Use and Interpretation of Anthropometry. Report of a WHO Expert Committee. Technical Report Series No. 854. Geneva, Switzerland: World Health Organization. 1995. 10.1037/e 412352004-001.8594834 · pubmed ↗
- 4World Health Organization (WHO). Promoting healthy diets. WHO Western Pacific Region; c 2023. Available from: https://www.who.int/westernpacific/activities/promoting-healthy-diets. cited 08 Nov 2025.