Debonding of the orthodontic brackets; is diode laser a safer method? Experimental invitro study
Eman M. Salem, S. M. Khattab

TL;DR
This study investigates whether a 940 nm diode laser can safely remove orthodontic brackets while reducing damage to tooth enamel.
Contribution
The study evaluates the effectiveness of diode laser irradiation in reducing bracket bond strength and enamel damage during bracket debonding.
Findings
Laser treatment significantly reduced shear bond strength in metallic brackets compared to controls.
Laser-treated brackets showed smoother enamel surfaces and fewer cracks compared to non-laser-treated controls.
The laser had limited effect on ceramic brackets at the tested power setting.
Abstract
Bracket debonding remains a clinical challenge in orthodontics, particularly when removing ceramic brackets, due to the potential risk of enamel cracks and surface damage. Recently, laser-assisted techniques have been investigated to facilitate safer and less traumatic bracket removal. This study aimed to evaluate the effect of 940 nm diode laser irradiation on the debonding process of metallic and ceramic orthodontic brackets by assessing shear bond strength (SBS) and enamel surface morphology using scanning electron microscopy (SEM). Thirty two extracted human premolars were randomly divided into four experimental groups: Group A (Control–Metallic),Group B (Control–Ceramic),Group C (Laser–Metallic), and Group D (Laser–Ceramic).Brackets were bonded using a light-cured adhesive and subjected to diode laser irradiation at 940 nm, 1 W, for 5 seconds in the laser-treated groups. SBS was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
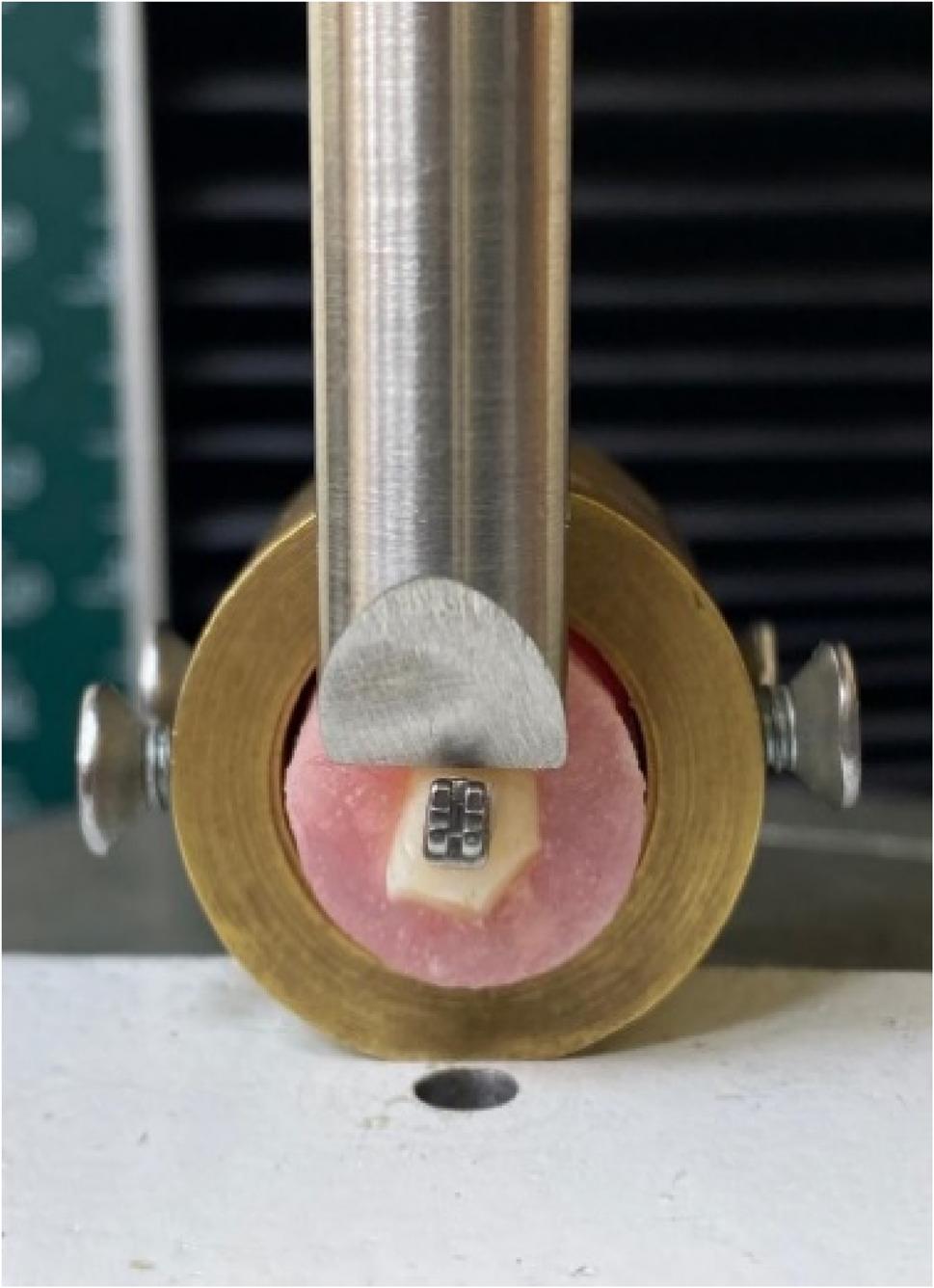 Figure 1
Figure 1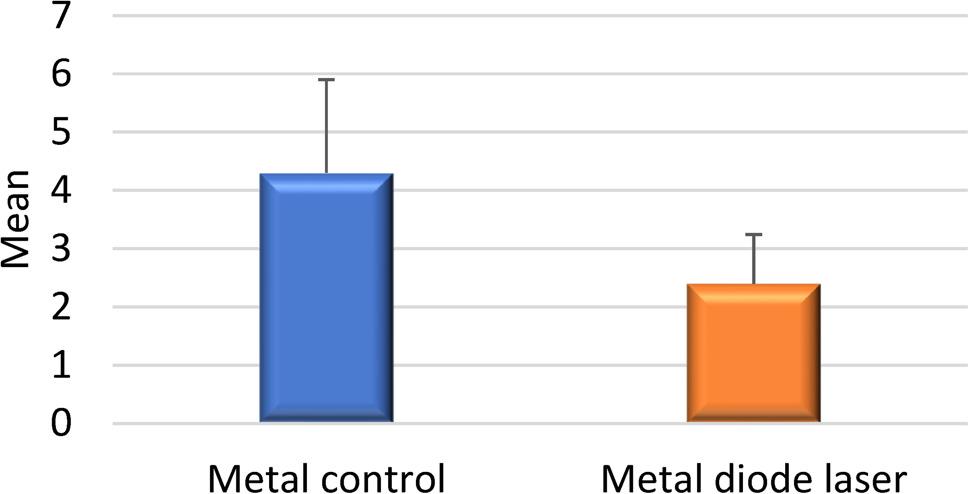 Figure 2
Figure 2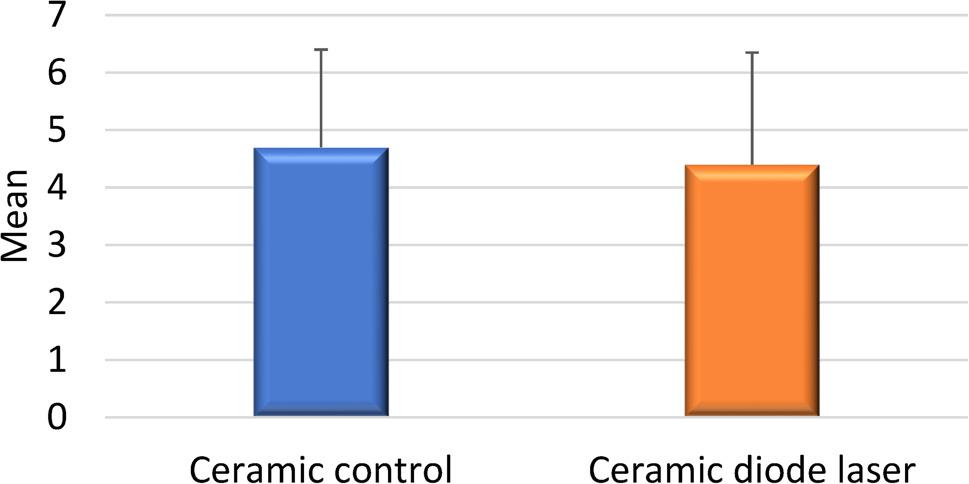 Figure 3
Figure 3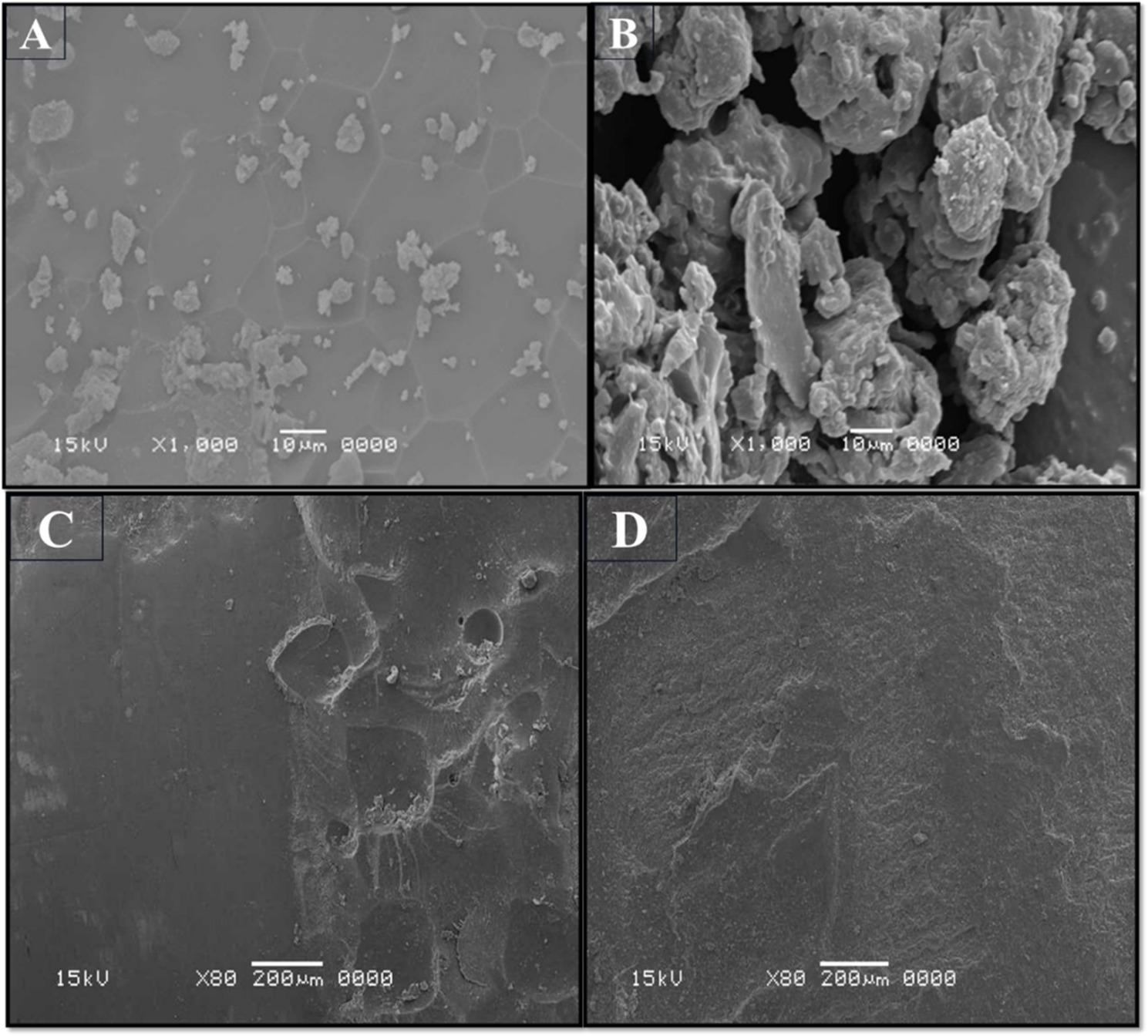 Figure 4
Figure 4- —Pharos University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLaser Applications in Dentistry and Medicine · Dental materials and restorations · Dental Erosion and Treatment
Introduction
Orthodontic treatment aims to achieve ideal occlusion and facial harmony; however, the final step—debonding of brackets—remains a critical and sometimes hazardous procedure. Excessive force during bracket removal can lead to enamel fractures, cracks, or surface loss, compromising the esthetic outcome and patient satisfaction [1]. The risk of enamel damage is particularly high when ceramic brackets are used, due to their high brittleness and low fracture toughness, which cause stress concentration at the adhesive–enamel interface during mechanical debonding [2].
Conventional mechanical removal methods rely on pliers or torsional forces to detach the bracket, often generating uncontrolled shear stresses that propagate through the enamel prisms. These stresses can cause irreversible enamel cracks, residual adhesive remnants, or even bracket fracture [3, 4]. To minimize these complications, laser-assisted debonding techniques have been proposed as a more conservative and patient-friendly alternative [5].
Different laser systems, such as CO₂, Er: YAG, Nd: YAG, and diode lasers, have been investigated for orthodontic bracket debonding [6]. The principle is based on localized heating of the adhesive resin, leading to its softening and subsequent reduction in shear bond strength (SBS). The laser type and wavelength determine how energy is absorbed and distributed across the bracket–adhesive–enamel complex [3].
Among these systems, diode lasers, typically operating between 810 nm and 940 nm, are especially advantageous because of their compact design, affordability, and selective absorption by pigmented adhesive components [3]. When used appropriately, diode laser energy can soften the resin without causing excessive intrapulpal temperature rise, maintaining thermal safety thresholds (< 5.5 °C) [4].
Laser–enamel interactions also depend on bracket material. Metallic brackets reflect a considerable portion of laser energy, reducing heat transmission to the adhesive, whereas ceramic brackets, being translucent, allow deeper light penetration and greater thermal diffusion [7]. Consequently, the optimal laser parameters differ for metallic and ceramic brackets to achieve efficient debonding without damaging enamel tissue.
Recent studies have shown that diode laser irradiation can significantly reduce SBS values for both bracket types while maintaining enamel integrity and pulpal safety [8]. However, reported outcomes remain inconsistent due to variations in power output, exposure time, and study design [8]. A 2022 BMC Oral Health study by Khalil et al. demonstrated the potential of diode laser-assisted debonding but highlighted the need for further research focusing on microstructural enamel changes rather than bond strength alone [9].
Therefore, this study aimed to evaluate the effect of 940 nm diode laser irradiation on the debonding of metallic and ceramic orthodontic brackets, analyzing both quantitative (SBS) and qualitative (SEM) outcomes. The novelty of this investigation lies in its focus on the histologic and microstructural preservation of enamel, providing insight into whether diode laser use can offer a safer and more biologically conservative method for bracket removal compared with conventional techniques.
Materials and methods
Study design and ethical approval
This was an in-vitro experimental study designed to evaluate the effect of 940 nm diode-laser irradiation on the debonding of metallic and ceramic orthodontic brackets, assessing both shear bond strength (SBS) and enamel surface morphology.
The protocol was approved by the Institutional Review Board of the Faculty of Dentistry, [Pharos University, Alexandria, Egypt under ethical code 393.]. The study followed the ethical standards of the Helsinki Declaration for research using human tissues.
Tooth selection and storage
Forty five (45) freshly extracted human premolars were collected from orthodontic patients aged 15–25 years who required extractions for therapeutic reasons. Inclusion criteria were: intact buccal enamel, no caries, cracks, restorations, or fluorosis. Thus, the sample size after exclusion was thirty-two (32) teeth, Immediately after extraction, the teeth were cleaned of soft-tissue remnants and stored in 0.1% thymol solution at 4 °C to prevent microbial growth and preserve mineral content until testing [10].
Before bonding, the teeth were rinsed thoroughly with distilled water and mounted vertically in self-curing acrylic resin blocks so that only the crown was exposed.
Grouping of samples
Specimens were randomly allocated into four experimental groups (n = 8 each) according to bracket type and debonding technique (Table 1):
- AMetallic bracket Conventional mechanical debonding (control)
- BCeramic bracket Conventional mechanical debonding (control)
- CMetallic bracket Diode-laser–assisted debonding
- DCeramic bracket Diode-laser–assisted debonding
Table 1. Showing the results of SBS measuring for control groups Metal Control
Force
SBS
Ceramic Control
Force
SBS 199.57.4137.82.8266.74.9235.12.6324.51.8378.65.8463.04.7482.66.1547.93.5549.03.6656.64.2689.86.7755.14.1783.96.2852.33.9848.53.6Average4.3Average4.7
Bonding procedure
The buccal enamel surface of each specimen was polished with pumice slurry using a rubber cup for 10 s, rinsed, and air-dried. The surface was then etched with 37% phosphoric-acid gel for 30 s, rinsed with water for 20 s, and air-dried until a frosty white appearance was visible.
A thin layer of Transbond XT primer (3 M Unitek, USA) was applied followed by Transbond XT adhesive paste. Stainless-steel or ceramic premolar edgewise brackets (0.022-inch slot, American Orthodontics, USA) were positioned and pressed firmly in place; excess resin was removed (Fig. 1).
Fig. 1. Measuring the SBS for the metallic bracket
Polymerization was performed using an LED curing unit (Elipar S10, 3 M ESPE, USA) for 20 s total (10 s mesial + 10 s distal). All specimens were stored in distilled water at 37 °C for 24 h to complete resin polymerization [11].
Laser irradiation protocol
Groups C and D were irradiated with a 940 nm diode laser (Epic X, Biolase Inc., USA) in continuous-wave mode. The laser was delivered through a 300 μm fiber-optic tip positioned 2 mm from the bracket surface, moved in a sweeping horizontal motion across the bracket base.
Operating parameters were: 1 W output power, 5 s exposure time, and spot size ≈ 0.3 mm².
Energy was applied evenly across the bracket to heat the adhesive layer by thermal conduction while avoiding enamel overheating. The selected settings were based on previously validated intrapulpal safety thresholds (< 5.5 °C temperature rise) [12].
Shear bond strength (SBS) testing
After irradiation, each specimen was fixed in a universal testing machine (Instron 3345, USA). A chisel-shaped metal blade was applied parallel to the enamel surface at the bracket–adhesive interface, and load was applied at a crosshead speed of 0.5 mm min⁻¹ until bracket failure occurred.
The debonding force (N) was recorded and converted to SBS (MPa) using:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$SBS = \frac{Force \left(N\right)}{Bracket\:base\:area \left(mm^{2}\right)}$$\end{document}where the bracket-base area = 10.61 mm².
Scanning electron microscopy (SEM) analysis
Two representative teeth from each group were ultrasonically cleaned, dehydrated in ascending ethanol concentrations (70%, 80%, 90%, 100%), sputter-coated with gold, and examined using a scanning electron microscope (JEOL JSM-6510LV, Japan) at ×80, ×500, and ×1000 magnifications.
Images were analyzed for enamel micro-morphology, including cracks, prism patterns, resin remnants, and surface smoothness [13].
Statistical analysis
Data analysis was performed using IBM SPSS Statistics, Version 24.0. The Shapiro–Wilk test confirmed the normal distribution of SBS data (p > 0.05). Quantitative data were presented as means and standard deviations. Independent sample t-tests were used to compare two groups, while one-way ANOVA followed by post hoc testing was applied for comparisons across more than two groups. A significance level of p < 0.05 was used throughout.
Analysis revealed a statistically significant difference in SBS between the metallic control group and the laser-assisted metallic group. However, no significant difference was observed between the ceramic control and laser-treated ceramic groups (Figs. 2 and 3).
Fig. 2. Comparison between SBS in metal control and metal diode laser
Fig. 3. Comparison between SBS in Ceramic control and Ceramic diode laser
Wilk test confirmed data normality. One-way ANOVA followed by Tukey’s post-hoc test compared mean SBS among groups, while Kruskal–Wallis and. Significance was set at p < 0.05.
Results
Shear bond strength (SBS) results
Shear bond strength testing was conducted using a universal testing machine (Tinius Olsen, Model 5ST, England, 2018). For each test, the buccal surface of the tooth was aligned parallel to the applied force vector, and the bracket slot was positioned horizontally. A chisel-edge blade was placed at the bracket–enamel interface in shear mode until bond failure occurred. The debonding force was recorded in Newtons and converted into megapascals (MPa) by dividing the applied force by the surface area of the bracket base.
The mean SBS values for the four experimental groups were as follows:
- Group A (Control – Metal): 4.3 MPa.
- Group B (Control – Ceramic): 4.7 MPa.
- Group C (Laser – Metal): 2.4 MPa.
- Group D (Laser – Ceramic): 4.4 MPa.
A reduction of approximately 45% in SBS was observed in the laser-treated metallic bracket group (Group C) compared to its control (Group A), indicating a significant weakening effect of the diode laser on the adhesive bond. These values are presented in Tables 1 and 2.
Table 2. Showing the results of SBS measuring for lased groups **Metal ** Diode Laser
Force
SBS
**Ceramic ** Diode Laser
Force
SBS 118.11.3128.62.1234.22.5275.15.6318.11.3376.95.7448.53.6421.31.6529.92.2597.97.3633.12.5667.55.0735.42.6769.15.1846.93.5843.13.2Average2.4Average4.4
Scanning electron microscopy (SEM) results
Scanning electron microscopy (SEM) was employed to examine enamel surface morphology and potential damage at the microstructural level. All samples were sputter-coated with gold prior to imaging to improve conductivity and image clarity. SEM images were captured at two magnifications:80× magnification to assess the overall morphology of the debonded surface, and 1000× magnification at three specific locations: the enamel surface, the bonded region, and the bracket–enamel interface.SEM analysis revealed a higher incidence of enamel cracks and surface irregularities in the control groups (Groups A and B) compared to the laser-assisted groups (Groups C and D). The laser-assisted debonding process appeared to preserve enamel integrity more effectively displayed markedly smoother surfaces with fewer cracks and minimal adhesive remnants. Representative SEM images are shown in (Fig. 4).
Fig. 4. Scanning electron micrographs of enamel surfaces after bracket debonding. Groups A and B (controls) exhibit irregular enamel topography with surface projections and areas of plaque accumulation (×1000). Group C (metallic–laser) shows a smoother, more homogeneous surface with generalized flattening and a marked reduction in surface irregularities compared with the control (×80). Group D (ceramic–laser) also demonstrates a smooth, uniform enamel surface with fewer surface irregularities (×80)
Discussion
The present study aimed to assess the influence of 940 nm diode laser irradiation on the debonding efficiency of metallic and ceramic orthodontic brackets. The results revealed a statistically significant reduction in shear bond strength (SBS) following laser exposure in metallic brackets, whereas the effect was less pronounced in ceramic brackets. These findings indicate that diode laser–assisted debonding can facilitate safer removal of metallic brackets by minimizing the mechanical stress transmitted to the enamel surface.
Comparison with previous studies
The current findings are in agreement with previous investigations demonstrating that diode laser irradiation effectively reduces the adhesive bond strength between orthodontic brackets and enamel [14, 15]. Comparable results were reported in studies where laser exposure at controlled power levels decreased SBS while maintaining pulpal safety. Furthermore, smoother enamel surfaces were observed following laser-assisted debonding compared with conventional mechanical techniques [16].
Nevertheless, the extent of SBS reduction appears to depend strongly on laser parameters, including wavelength, output power, and exposure duration. Investigations employing higher power levels (2.5–5 W) achieved greater reductions in SBS but also noted an increased risk of intrapulpal temperature rise [14]. In the present study, the use of a 940 nm diode laser at 1 W for 5 s achieved an optimal balance between effective debonding and enamel protection.
Mechanism of laser action
The mechanism underlying laser-assisted debonding is primarily associated with the interaction of laser energy with bracket and adhesive materials. Although metallic brackets reflect part of the laser energy, adequate thermal conduction through the bracket base allows localized heating and softening of the adhesive interface. In contrast, ceramic brackets exhibit lower thermal conductivity and higher translucency, which may limit energy absorption and explain the minimal reduction in SBS observed in this group.
The softening of the resin matrix under laser exposure is thought to result from localized thermal expansion and partial degradation of the adhesive polymer, thereby facilitating bracket removal at lower mechanical stress levels. These observations are consistent with previous findings [17, 18].
Enamel surface morphology
Scanning electron microscopy (SEM) analysis further supported the protective role of diode laser irradiation on enamel integrity. Control specimens exhibited distinct surface irregularities, cracks, and residual adhesive remnants, whereas laser-treated specimens showed smoother, more homogeneous enamel surfaces, indicative of reduced mechanical damage.
Comparable results have been reported in earlier studies, where laser-induced softening of adhesive resin minimized the risk of enamel microcracks and improved the ease of adhesive removal [19, 20]. These outcomes suggest that diode laser–assisted debonding not only facilitates efficient bracket removal but also contributes to superior enamel preservation and improved post-treatment aesthetics.
Clinical implications
Clinically, the results highlight that diode laser–assisted debonding may serve as an effective adjunctive technique, particularly for metallic brackets. The observed reduction in the required debonding force may decrease the risk of enamel fractures and enhance patient comfort during bracket removal. Nevertheless, clinicians must adhere to evidence-based safety parameters to avoid excessive thermal effects within the pulp chamber. Although the present study did not measure intrapulpal temperature changes, prior ex vivo investigations have demonstrated that diode lasers operating at 1 W typically induce temperature increases below the critical threshold of 5.5 °C [14].
Accordingly, careful device calibration and operator training are essential prerequisites for the safe and effective clinical application of diode laser–assisted debonding.
Limitations
Several limitations should be acknowledged.
First, this was an in vitro study, which does not fully replicate the complex biological conditions of the oral cavity, such as pulpal circulation, saliva, and temperature fluctuations.
Second, pulpal temperature changes were not directly measured, which limits conclusions regarding thermal safety.
Third, the sample size was relatively small, and only one power setting (1 W) and exposure duration (5 s) were evaluated.
Future studies should employ larger sample sizes, different diode laser power settings, and in vivo models to confirm the optimal parameters for safe and effective bracket debonding.
Conclusion
Diode laser assisted debonding (Diode laser 940 nm ,1 W), is a promising tool in brackets debonding as it reduced the shear bond strength of the composite resin and reduced the occurrence of enamel cracks, thus it is a safer method for bracket debonding. But it should be used with the proper parameters, to be a safe method for preserving tooth tissue. Further research upon this field is mandatory.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen L, Hontsu S, Komasa S, Yamamoto E, Hashimoto Y, Matsumoto N. Hydroxyapatite film coating by er:yag pulsed laser deposition for the repair of enamel defects. Materials. 2021;14(7475). 10.3390/ma 14147475.10.3390/ma 14237475 PMC 865928134885628 · doi ↗ · pubmed ↗
- 2Ghaleb L, Al-Worafi NA, Thawaba A, et al. Evaluation of enamel surface integrity after orthodontic bracket debonding: comparison of three different systems. BMC Oral Health. 2024;24. 10.1186/s 12903-024-04138-4. Article 358.10.1186/s 12903-024-04138-4PMC 1095316138509532 · doi ↗ · pubmed ↗
- 3Matei GC, Peruzzo DC, Kantovitz KR et al. Effect of diode laser irradiation on bond strength of resin cements to high-translucent zirconia. J Clin Exp Dent. 2024. 10.4317/jced.61953 . (diode laser & bond strength to zirconia; relevant for laser-material interactions). (full text available in PMC) roderic.uv.es+1 .10.4317/jced.61953 PMC 1155910939544209 · doi ↗ · pubmed ↗
- 4Liebertpub systematic review (meta-analysis): The Effect of Various Lasers on the Bond Strength Between Orthodontic Brackets and Dental Ceramics — Photomed Laser Surg. 2023. 10.1089/photob.2023.0098 . (systematic review / meta-analysis reviewing laser effects on ceramic bracket SBS). liebertpub.com.10.1089/photob.2023.009837862260 · doi ↗ · pubmed ↗
- 5Matei GC et al. (related) — Effect of diode laser irradiation on bond strength of resin cements (PMC full text). This article is a recent, peer-reviewed source examining diode-laser interaction with dental restorative materials and is useful for mechanistic discussion (thermal effects / surface changes). pmc.ncbi.nlm.nih.gov.
- 6Additional 2020–2024 studies on lasers and enamel / debonding (useful for background & discussion): Colín-Ocampo JA et al., Cureus, CO₂. laser & SBS. (already above). Cureus Recent BMC Oral Health 2024 papers about enamel integrity / adhesive removal methods (Ghaleb 2024, Zheng 2024) — both already above and directly relevant. Bio Med Central+1. Bio Med Central+1.
- 7Unal M et al. Effect of acid etching and different er:yag laser procedures on microleakage …. 2013. 10.4012/dmj.2013-02323903636 · doi ↗ · pubmed ↗