Individualized nutritional care including adherence support improves health-related quality of life in individuals with severe chronic obstructive pulmonary disease: a randomized controlled trial
Maria H. Hegelund, Christian Ritz, Mette F. Olsen, Christian Mølgaard, Thyge L. Nielsen, Andreas V. Jensen, Christian Søborg, Lone Braagaard, Rikke Krogh-Madsen, Birgitte Lindegaard, Daniel Faurholt-Jepsen

TL;DR
A study found that personalized nutrition plans with support improved quality of life and physical function in people with severe COPD.
Contribution
The study demonstrates that individualized nutritional care with adherence support can enhance HRQoL in severe COPD patients.
Findings
Individualized nutritional care improved HRQoL (EQ-5D-5L) by 0.053 compared to standard care.
Participants in the intervention group performed more chair stands, indicating better physical function.
Protein and energy intake increased significantly in the intervention group.
Abstract
Undernutrition and reduced health-related quality of life (HRQoL) are common in severe chronic obstructive pulmonary disease (COPD) and may exacerbate functional decline. This study evaluated whether individualized nutritional care with adherence support improves HRQoL in individuals with severe COPD at risk of undernutrition. Secondary outcomes included physical function, anthropometry, body composition, and dietary intake. In this 3-month, single-center, open-label randomized controlled trial, 87 adults with severe COPD were randomized 1:1 to individualized nutritional care or standard care. The intervention comprised tailored dietary plans, adherence support (phone calls, reminders), optional oral nutritional supplements and weight diary. The primary outcome was HRQoL (EQ-5D-5 L). Secondary outcomes were disease-specific HRQoL (CAT), chair stand test, grip strength, anthropometry,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
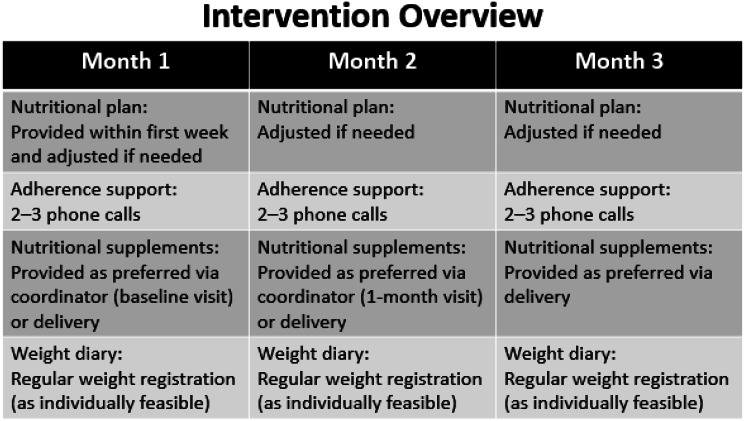 Figure 1
Figure 1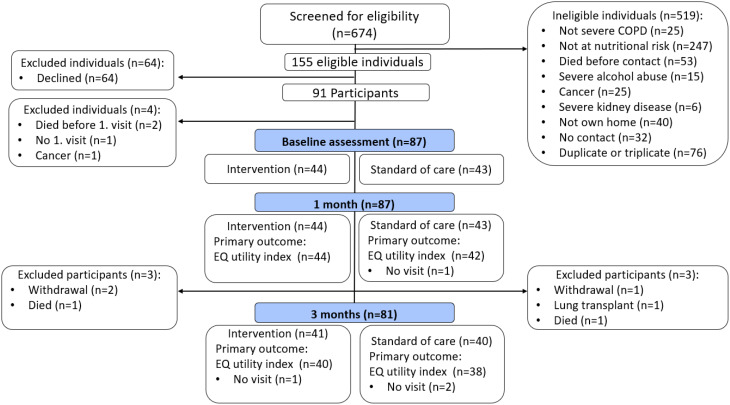 Figure 2
Figure 2- —Copenhagen University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Obstructive Pulmonary Disease (COPD) Research · Respiratory Support and Mechanisms · Frailty in Older Adults
Introduction
Chronic obstructive pulmonary disease (COPD) is a major global health concern. In Denmark, approximately 50,000 individuals have severe COPD [1]. Low health-related quality of life (HRQoL) is common in severe COPD due to high symptom burden, low functional ability, anxiety, and depression [2]. Undernutrition, characterized by an insufficient intake relative to biological needs, is also prevalent in COPD [3]. Undernutrition and COPD may be bidirectionally linked: undernutrition can worsen disease progression [3], while COPD-related low appetite and dyspnoea contribute to inadequate food intake [3]. This combination is often associated with reduced mobility and further reductions in HRQoL [4, 5]. Acute exacerbations and infections exacerbate these problems, often causing unintentional weight loss that is difficult to reverse without nutritional support [6, 7]. Increased energy expenditure due to breathing difficulties further complicates nutritional balance [3, 7]. Anxiety and depression are common but often overlooked in COPD, with negative effects on HRQoL, functional ability, and social interactions [8–12].
Systematic reviews suggest that dietary therapy in COPD can improve food intake, anthropometric measures, functional capacity, and HRQoL [13, 14]. However, most studies are over 30 years old, with small sample sizes (6 out of 8 studies included fewer than 30 participants) [14], and only one RCT included individuals with severe COPD, with just 10 participants [15]. Nutritional care remains underprioritized in COPD treatment [16], and despite evidence of potential benefits, interventions are still insufficiently developed and evaluated.
We hypothesized that individualized nutritional care, including adherence support, would improve HRQoL compared with standard care in individuals with severe COPD. The primary outcome was HRQoL, while secondary outcomes included disease-specific quality of life, anthropometric measures, body composition, functional ability, and energy and protein intake.
Methods
Trial design
This single-center, open-label randomized controlled trial (RCT) compared individualized nutritional care, including adherence support, with standard care in adults with severe COPD. Participants were randomly allocated 1:1 to intervention or control. Enrollment was completed by March 2023.
Participants and recruitment
Potential participants were identified from hospital electronic medical records. Random selection was performed using R [17]. Additional recruitment included oral invitations during hospitalization or outpatient visits at the department, primarily for conditions related to COPD, including acute exacerbations and respiratory tract infections. Eligible participants were ≥ 35 years, had severe COPD, could eat orally, lived at home, were undernourished or at risk of undernutrition, and were clinically stable, defined as having no current acute exacerbation or respiratory tract infection at the time of the enrollment. Participants could be informed about the study during hospitalization, but final enrollment and baseline assessment were postponed until clinically stability was achieved. Exclusion criteria included inability to provide informed consent, active solid cancer, severe renal failure, or severe alcohol abuse.
Setting
The study was conducted at the Department of Pulmonary and Infectious Diseases, Copenhagen University Hospital – North Zealand, Denmark. Baseline and follow-up data were collected in participants’ homes by the study coordinator.
Standard care
At the pulmonary outpatient clinic, standard care for severe COPD includes assignment to a specialized nurse, annual physician–nurse consultations covering disease progression, symptom management, prognosis, and advance care planning, telephone access to specialized nurses on weekdays, and periodic rehabilitation programs focused on exercise and COPD education, with limited focus on nutrition [18–20].
Intervention
The 3-month intervention, illustrated in Fig. 1, was designed based on prior studies showing that individualized nutritional care improves intake, functional outcomes, and quality of life in COPD and older adults at risk of undernutrition [7, 21–23]. The intervention was delivered by the study coordinator and included:
- Individualized nutritional plan: Nutritional plans were tailored using baseline weight and dietary intake assessed by 24-hour dietary recall. Protein intake was targeted at approximately 1.5 g/kg/day [23], and energy intake at 30–45 kcal/kg/day depending on nutritional status and clinical need [7]. Plans were adapted to adress individual challenges such as dyspnea during meals, low appetite or fatigue.
- Adherence support: Evidence-based strategies including phone calls every 7–14 days, a fridge magnet reminder, and encouragement for regular weight tracking, designed to enhance engagement, support self-monitoring, and overcome common barriers to adherence in chronic disease nutritional interventions [7, 24–26]. During adherence calls, nutritional plans were adjusted based on participant progress, weight changes and, dietary intake and reported challenges (e.g., swallowing difficulties, dyspnea).
- Supplementation: Participants were offered oral nutritional supplements available through the hospital when needed to support achievement of protein and energy targets. For participants who declined supplements, alternative strategies were provided including guidance on high-protein and energy-dense foods and recipes.
The intervention followed a predefined protocol specifying assessment, target setting, follow-up frequency, and criteria for adjustment, while allowing flexibility to accommodate individual needs (Fig. 1).
After trial conduct, the original non-adherence definition [27] was found difficult to measure reliably. Adherence was therefore defined a priori, prior to data analysis, as ≥ 6 phone contacts, ≥ 4 dietary records, and an average energy and protein intake of ≥ 30 kcal/kg/day and ≥ 1 g/kg/day, with participants not meeting these criteria classified as low adherence.
Sample size calculation
No prior studies reported EQ-5D-5 L outcomes in a similar population. A prior COPD study using the Chronic Respiratory Disease Questionnaire (CRQ) reported a 10-point improvement in disease-specific HRQoL with a standard deviation 17 [28]. Despite differences between CRQ and EQ-5D-5 L, these data were used as a proxy. A total of 60 participants per group was estimated to provide 80% power at α = 0.05, assuming 20% drop-out.
Fig. 1. Schematic illustration of the intervention
Randomization and blinding
Participants were randomized using computer-generated block randomization in R. Allocation concealment was managed by an independent researcher. Group assignment was revealed to the study coordinator and participants after baseline assessment.
Data collection
Nutritional risk
Assessed using NRS-2002 (≥ 3 indicates risk) [29] and MNA-SF (scores 8–11: risk; 0–7: undernutrition) [30]. Participants meeting risk criteria on either tool were eligible if other inclusion criteria were met.
Baseline characteristics
Baseline characteristics included demographics, clinical factors, lifestyle, and physical and functional status. Demographics and social factors comprised age, sex, and living situation (solitary vs. cohabiting). Clinical characteristics included COPD diagnosis by spirometry (post-bronchodilator FEV1/FVC < 0.70), disease severity according to GOLD ABCD criteria, with severe COPD defined as GOLD 3–4 or GOLD 2 with high symptom/exacerbation burden [31]. Comorbidity burden was assessed using the Charlson Comorbidity Index, including both total number and specific comorbidities, while home oxygen use and presence of emphysema were obtained from medical records. Lifestyle factors included alcohol intake (categorized as within or above recommendations) and smoking status (never, previous, or current). Physical and functional status was assessed using the FRAIL scale (robust, pre-frail, frail) [32] and undernutrition defined according to ESPEN criteria, considering age, BMI, weight loss, and fat-free mass index (FFMI) [33].
Outcomes
Primary outcome
Generic HRQoL was assessed using the Danish EQ-5D-5 L, covering mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each domain was scored 1–5 and converted to a utility index (range − 0.624 to 1.000). Participants also rated overall health on the EQ VAS (0–100) [34].
Secondary and other outcomes
Disease-specific HRQoL was assessed with the COPD Assessment Test (CAT; 8 items, score 0–40, higher scores = worse HRQoL) [35, 36]. Anthropometry included height (from medical records, confirmed by participants), weight (0.1 kg, TANITA DC 430 SMA, Denmark), BMI (kg/m²), and waist, hip, and mid-upper arm circumferences (0.1 cm) [37, 38]. Body composition (FFMI, FMI (kg/m²)) was derived from bioelectrical impedance (TANITA DC 430 SMA). Nutritional intake (protein, energy) was estimated from 24-h recalls [39] and calculated using MADlog (Denmark). Functional measures comprised grip strength (kg; SAEHAN DHD-1 dynamometer, South Korea; 3 trials on dominant hand or 3 per hand if uncertainty of dominant hand, highest value recorded) [40] and the 30-s chair stand test (unmodified version) [41]. Physical activity (min/week) was assessed with the physical activity vital signs questionnaire [42] and categorized as < 150 or ≥ 150 min/week according to recommended levels [43]. Outcomes were assessed at baseline, 1 and 3 months.
Deviations from pre-registered outcomes
The trial was pre-registered at ClinicalTrials.gov (NCT04873856). During the study, some pre-specified outcomes could not be reported due to feasibility and data quality issues. Data on oxygen therapy and exacerbations were based on self-report and found to be unreliable, and medical record validation was not feasible; therefore, oxygen use was only reported at baseline. Hospital admissions and mortality, originally planned for 3-month follow-up, will instead be reported at 6- and 12-month follow-up. Anxiety and depression (HADS) were not analyzed as permission for the instrument was not obtained before study start. Finally, accelerometer-based physical activity data were not analyzed due to limited time and resources, although future analyses may include these data; only questionnaire-based physical activity data were used for this manuscript.
Statistical analysis
Analyses were conducted in Stata (StataCorp 2021, Stata Statistical Software: Release 17, College Station, TX: Stata Corp LLC). Continuous variables are presented as means with standard deviation (SD) or median with interquartile range (IQR), whereas categorical variables were reported as counts (%). Intention-to-treat analyses were conducted using linear mixed-effects models. These models included an intervention-by-time interaction as a fixed-effect, while between-participant variation was modeled with participant-specific random intercepts. Relevant covariates (as fixed effects) included variables with observed baseline imbalance. Pre-defined relevant covariates comprised age, sex, solitary-living, FEV1, smoking status, physical activity level, and the baseline value of the outcome. Per-protocol analyses compared fully adherent participants with the standard care group. Subgroup analyses of HRQoL (EQ utility index and the EQ domains) were conducted for undernourished, frail, solitary-living participants, participants with ≥ 1 cardiovascular comorbidity, and by sex on the primary outcome EQ utility index and the EQ domains. Estimated mean differences at 1 month and 3 months were reported together with the corresponding 95% confidence intervals (CI) and p-values. Statistical significance was declared for p-values below 0.05.
Ethical considerations and approvals
The study was approved by the local ethics committee (H-20060574), registered at ClinicalTrials.gov (identifier: NCT04873856) in April 2021, and conducted in accordance with the Declaration of Helsinki and the CONSORT guidelines [44]. Permission to use the EQ-5D-5 L and CAT instruments was obtained. Written and oral informed consent was obtained from all participants prior to enrolment.
Results
Of 674 individuals screened, 91 were included between May 2021 and March 2023. Eighty-seven completed the baseline, with 44 randomized to the intervention and 43 to standard care (approximately two-thirds female in each group). Seventy-eight (90%) participants completed the 3-month visit (Fig. 2). At baseline, the median (IQR) FEV1 was 31% (24–42) and 30% used home-based oxygen therapy. Comorbidity was common: 74% had at least one, and 30% had two or more. The most frequent comorbidities were cardiovascular diseases (37%) and osteoporosis (52%). Two thirds of the participants were undernourished and almost 40% were frail (Table 1).
Fig. 2. Flow of participants
Table 1. Baseline characteristics of 87 individuals with severe chronic obstructive pulmonary diseaseIntervention group(n = 44)Control group(n = 43)Age, years75 ± 771 ± 8Female sex, n (%)30 (68)29 (67)Living alone, n (%)25 (57)18 (42)Alcohol consumption > guidelines, n (%)9 (20)12 (27)Smoking,** n (%)** Never3 (7)1 (2) Previous26 (59)29 (67) Current15 (34)13 (30) Lung function Forced expiratory volume in 1 s, %30.5 (23.5–42)34 (24–42) Severe (30–49%), n (%)20 (45)19 (44) Very severe (< 30%), n (%)24 (55)24 (56)Pulmonary emphysema, n (%)41 (93)40 (93)Home-based oxygen therapy, n (%)13 (30)13 (30) Comorbidity burden Charlson comorbidity index5 (4–6)4 (3–5)Number of comorbidities^#^ 0, n (%)13 (30)9 (21) 1, n (%)15 (34)23 (53) ≥2, n (%)15 (36)11 (26) Nutritional risk MNA-SF score ≤ 11, n (%)43 (98)42 (98)NRS2002 score ≥ 3, n (%)33 (77)32 (76) Physical and functional status Frail, n (%)21 (48)12 (29)Undernourished^##^, n (%)28 (64)31 (72)Data reported as mean ± SD, median (IQR), or n (%). # Number of comorbidities included hypothyroid, Addison Disease, Struma, chronic pancreatitis, sarcoidosis, macroglobulinemia (Waldenstrom), rheumatoid arthritis, dementia, liver disease, cardiovascular disease, osteoporosis, and diabetes. ## Defined according to recommended guidelines by European Society for Clinical Nutrition and Metabolism
Health-related quality of life (primary outcome)
After three months, the intervention led to a higher HRQoL compared to standard care, with a mean difference (95% CI) in EQ utility index of 0.053 (0.003; 0.103, p = 0.04). Improvements were seen in mobility,* selfcare*, and usual activities with mean differences of -0.543 (-0.901; -0.185, p < 0.01), -0.686 (-1.016; -0.356, p < 0.01), and − 0.496 (-0.818; -0.175, p < 0.01), respectively. No between groups differences was seen in EQ VAS (-4.77, -12-12; 2.59, p = 0.20) (Table 2). Subgroup analyses showed benefits in HRQoL among undernourished participants, solitary-living participants, frail participants, and men with mean differences (95% CI) in the EQ utility index of 0.078 (0.013; 0.143, p < 0.01), 0.065 (0.005; 0.120, p = 0.03), 0.210 (0.137; 0.283, p < 0.01), and 0.104 (0.026; 0.181, p < 0.01), respectively. Effects across EQ domains varied by subgroup (Table 3). No intervention-related adverse events were observed during the study.
Other effects after three months
There was no difference between the groups in disease-specific HRQoL (CAT score). After three months, waist circumference was 1.22 cm higher in the intervention group (95% CI 0.01; 2.44, p = 0.049). No other anthropometric or body composition effects were observed. Protein and energy intake was higher in the intervention group with mean differences of 16 g (95% CI 6.01; 26.05, p < 0.01) and 326 kcal (95% CI 105.08; 547.74, p < 0.01), respectively. Functional ability was higher in the intervention group with a higher number of chair stands (mean difference 0.80, 95% CI 0.05; 1.55, p = 0.04), while no difference was seen in grip strength (Table 2).
Effects after one month
No differences were observed after one month in generic or disease-specific HRQoL, anthropometry, body composition, chair stand test, or grip strength. However, protein intake was higher in the intervention group (mean difference 12 g, 95% CI 1.87; 21.29, p = 0.02), while energy intake did not differ (Table 2). Subgroup analyses showed early HRQoL benefits: frail participants had higher EQ utility index (0.112, 95% CI 0.039; 0.185, p < 0.01) and reported improvements in mobility,* self-care*, and anxiety or depression. Undernourished participants reported improvements in usual activities and pain or discomfort. Women reported improvements in usual activities. Men reported improvements in pain or discomfort (Table 3).
Adherence and per protocol analyses
Fifteen participants were categorized as low adherent: one died, two had less than six contacts or fewer than four dietary registrations and twelve did not meet the threshold of both protein and energy intake. This corresponds to 83% of participants achieving high adherence to the intervention. Per-protocol analyses showed results largely consistent with the intention-to-treat analyses. Effect sizes (in favor of the intervention) were greater for the EQ utility index, the EQ domains mobility and selfcare, and energy intake at the 3-month follow-up visit. The mean differences for usual activities and protein intake were comparable to those in the intention-to-treat analyses. In contrast, the mean differences for the chair stand test and waist circumference were slightly attenuated and no longer statistically significant (Supplementary Table 1).
Table 2. Effect of individualized nutritional intervention including adherence support among individuals with severe chronic obstructive pulmonary disease at risk of undernutritionOutcome1 month (n = 87)3 months (n = 81)Mean difference (95% CI) P Mean difference (95% CI) P
Primary EQ utility index0.018 (-0.031; 0.066)0.480.053 (0.003; 0.103)0.04 * EQ mobility* -0.240 (-0.588; 0.107)0.18-0.543 (-0.901; -0.185)< 0.01 * EQ self-care* -0.316 (-0.637; 0.005)0.054-0.686 (-1.016: -0.356)< 0.01 * EQ usual activities* -0.227 (-0.539; 0.085)0.15-0.496 (-0.818; -0.175)< 0.01 * EQ pain or discomfort* -0.329 (-0.703; 0.046)0.09-0.245 (-0.633; 0.143)0.22 * EQ anxiety or depression* -0.138 (-0.443; 0.168)0.38-0.186 (-0.498; 0.126)0.24EQ VAS-0.86 (-8.00; 6.27)0.81-4.77 (-12.12; 2.59)0.20 Secondary/other COPD Assessment Test-0.36 (-1.92; 1.21)0.66-0.36 (-1.97; 1.25)0.66Body mass index, kg/m^2^0.09 (-0.17; 0.34)0.500.10 (-0.16; 0.36)0.44Fat-free mass index, kg/m^2^0.05 (-0.12; 0.22)0.58-0.01 (-0.20; 0.17)0.89Fat mass index, kg/m^2^0.01 (-0.17; 0.20)0.89-0.05 (-0.24; 0.14)0.59Grip strength, kg0.13 (-0.88; 1.15)0.800.09 (-0.94; 1.12)0.86Chair Stand Test0.22 (-0.50; 0.95)0.550.80 (0.05; 1.55)0.04Waist circumference, cm0.80 (-0.38; 1.99)0.181.22 (0.01; 2.44)0.049Hip circumference, cm0.09 (-0.88; 1.06)0.860.68 (-0.32; 1.68)0.18Upper-arm circumference, cm0.04 (-0.41; 0.49)0.870.31 (-0.15; 0.77)0.18Protein intake, g11.58 (1.87; 21.29)0.0216.03 (6.01; 26.05)< 0.01Energy intake, kcal155.97 (-59.72; 371.66)0.16326.41 (105.08; 547.74)< 0.01Physical activity, min/week26 (-76; 137)0.1843 (-149; 64)0.43Higher EQ utility index and VAS indicate better quality of life. A positive mean difference reflects a beneficial effect for utility and VAS, while a negative mean difference reflects benefit for domain scores (scored 1–5). The model was adjusted for baseline imbalances (age, grip strength, protein intake, Charlson index), predefined covariates (sex, living alone, FEV1, smoking, physical activity), and the baseline outcome value
Table 3. Effect of individualized nutritional intervention including adherence support on health-related quality of life among subgroups of severe chronic obstructive pulmonary diseaseOutcome1 month3 monthsMean difference (95% CI) P Mean difference (95% CI) P
Undernourished ( n ** = 59)** EQ utility index0.031 (0.031–0.093)0.310.078 (0.013; 0.143)0.02 * EQ mobility* -0.391 (-0.841; 0.058)0.09-0.587 (-1.053; -0.120)0.01 * EQ self-care* -0.225 (-0.613;0.163)0.26-0.796 (-1.201; -0.391)< 0.01 * EQ usual activities* -0.535 (-0.905; -0.166)< 0.01-0.886 (-1.271; -0.500)< 0.01 * EQ pain or discomfort* -0.523 (-1.001; -0.045)0.03-0.302 (-0.803; 0.199)0.24 * EQ anxiety or depression* -0.094 (-0.480; 0.293)0.63-0.226 (-0.625; 0.173)0.27 Solitary-living ( n ** = 43)** EQ utility value0.049 (-0.008; 0.104)0.090.065 (0.005; 0.124)0.03 * EQ mobility* -0.431 (-0.939; 0.078)0.10-0.868 (-1.405; -0.331)< 0.01 * EQ self-care* -0.282 (-0.660; 0.100)0.14-0.796 (-1.200; -0.395)< 0.01 * EQ usual activities* -0.198 (-0.694; 0.299)0.44-0.539 (-1.061; -0.018)0.04 * EQ pain or discomfort* -0.144 (-0.625; 0.336)0.56-0.191 (-0.697; 0.315)0.46 * EQ anxiety or depression* -0.132 (-0.564; 0.299)0.550.039 (-0.407; 0.484)0.87 Cardiovascular comorbidity ( n ** = 32)** EQ utility value0.021 (-0.054; 0.096)0.580.069 (-0.009; 0.147)0.08 * EQ mobility* -0.405 (-1.103; 0.393)0.26-0.137 (-0.859; 0.585)0.71 * EQ self-care* -0.268 (-0.800; 0.264)0.32-0.821 (-1.377; -0.265)< 0.01 * EQ usual activities* -0.224 (-0.702; 0.253)0.36-0.887 (-1.400; -0.394)< 0.01 * EQ pain or discomfort* -0.328 (-0.856; 0.201)0.23-0.364 (-0.921; 0.193)0.20 * EQ anxiety or depression* -0.014 (-0.430; 0.403)0.95-0.017 (-0.415; 0.449)0.94 Frail ( n ** = 33)** EQ utility value0.112 (0.039; 0.185)< 0.010.210 (0.137 0.283)< 0.01 * EQ mobility* -0.760 (-1.240; -0.281)< 0.01-1.183 (-1.661; -0.704)< 0.01 * EQ self-care* -0.706 (-1.211; 0.202)< 0.01-1.394 (-1.897; -0.890)< 0.01 * EQ usual activities* -0.383 (-0.838; 0.072)0.10-1.034 (-1.488; -0.580)< 0.01 * EQ pain or discomfort* -0.547 (-1.161; 0.067)0.08-0.453 (-1.067; 0.162)0.15 * EQ anxiety or depression* -0.717 (-1.152; -0.282)< 0.01-0.821 (-1.255; -0.387)< 0.01 Women ( n ** = 59)** EQ utility value0.012 (-0.044; 0.068)0.680.024 (-0.034; 0.082)0.42 * EQ mobility* -0.107 (-0.512; 0.298)0.60-0.458 (-0.880; -0.0365)0.03 * EQ self-care* -0.371 (-0.711; 0.031)0.03-0.761 (-1.116; -0.407)< 0.01 * EQ usual activities* -0.189 (-0.583; 0.206)0.35-0.276 (-0.686; 0.135)0.19 * EQ pain or discomfort* -0.219 (-0.662; 0.224)0.33-0.008 (-0.456; 0.472)0.97 * EQ anxiety or depression* -0.009 (-0.358; 0.340)0.96-0.012 (-0.369; 0.345)0.95 Men ( n ** = 28)** EQ utility value0.038 (-0.037; 0.113)0.320.104 (0.026; 0.181)< 0.01 * EQ mobility* -0.486 (-1.074; 0.103)0.11-0.637 (-1.242; 0.033)0.04 * EQ self-care* -0.375 (-1.026; 0.277)0.26-0.690 (-1.356; 0.023)0.04 * EQ usual activities* -0.271 (-0.705; 0.162)0.22-0.892 (-1.337; -0.446)< 0.01 * EQ pain or discomfort* -0.598 (-1.115; -0.081)0.02-0.697 (-1.229; -0.164)0.01 * EQ anxiety or depression* -0.400 (-0.943; 0.143)0.15-0.490 (-1.047; 0.067)0.09Higher EQ utility index and VAS indicate better quality of life. A positive mean difference reflects a beneficial effect for utility and VAS, while a negative mean difference reflects benefit for domain scores (scored 1–5). The model was adjusted for baseline imbalances (age, grip strength, protein intake, Charlson index), predefined covariates (sex, living alone, FEV1, smoking, physical activity), and the baseline outcome value
Discussion
This study demonstrates that individually tailored nutritional care including adherence support can improve HRQoL compared to standard care, particularly the physical domains, among individuals with severe COPD at risk of undernutrition. To our knowledge, this is the largest RCT of individualized nutritional care in this patient group.
Consistent with prior work, participants had markedly reduced HRQoL at baseline. The median EQ utility index of 0.65 was lower than in the general older population (0.80) [45] and comparable to previous COPD cohorts [46]. The observed mean difference of 0.053 is clinically meaningful, exceeding published thresholds for minimal important differences in COPD [46, 47]. Importantly, improvements were evident across all physical HRQoL domains and supported by gains in functional ability, as shown by the chair stand test. Functional limitations strongly affect HRQoL and can trigger a downward spiral of fatigue, dependence, social isolation, and psychological distress [48–50]. Our findings suggest that nutritional care may interrupt this trajectory.
Some participants in both groups attended outpatient pulmonary rehabilitation, which typically enhances physical performance. However, nutritional needs are often insufficiently addressed within rehabilitation programs [51]. By deliberately separating the interventions, we ensured that vulnerable individuals unwilling or unable to attend rehabilitation were not excluded. Nevertheless, future studies should explore combined approaches, as integrating tailored nutrition with structured physical training may yield greater improvements. Subgroup analyses indicated that undernourished, frail, and male participants benefitted the most. Although these analyses should be interpreted with caution due to small sample sizes, they underscore vulnerable subgroups that may gain the greatest benefit from individualized care.
The intervention improved nutritional intake but not anthropometry or body composition. This likely reflects baseline heterogeneity: although all participants were undernourished or at risk, BMI ranged from 12.9 to 24.6 kg/m², resulting in divergent nutritional goals. For some, the aim was maintenance; for others, weight gain. In this context, functional improvements may be more meaningful than anthropometric change.
Strengths of this study include the high retention rate, likely facilitated by home-based visits, and the use of EQ-5D-5 L, a validated HRQoL instrument in both Danish and COPD populations [46, 52]. Limitations include the open-label design, as neither participants nor outcome assessors were blinded, which may introduce measurement or reporting bias and increase awareness of dietary behaviors among participants in the control group. However, standardized assessment procedures and the use of validated outcome measures were applied to mitigate this risk. The single-center setting may restrict generalizability. COPD is a heterogeneous condition [53]; responses to nutritional care may therefore vary across disease phenotypes. The intervention was delivered as a multicomponent package, and the study was not powered to evaluate the relative contribution or effectiveness of individual components.
Despite these limitations, our findings underline the need for individualized nutritional care in COPD. Even among those with lower adherence, many participants reported increased awareness of nutritional needs. Current outpatient care often overlooks nutrition due to lack of expertise and clear responsibility [16]. The structured and protocol-based nature of the intervention suggests that similar nutritional care programs could be delivered in routine clinical practice as part of outpatient care by trained healthcare professionals following appropriate training. Given the preventive potential across HRQoL domains, a multidisciplinary approach—combining nutritional care, adherence support, physical training, psychiatry, and pharmacology—may yield broader and more sustained benefits.
Conclusion
Individualized nutritional care with adherence support improved HRQoL, particularly physical functioning, in individuals with severe COPD at risk of undernutrition. As HRQoL is a central treatment goal in advanced COPD, integration of structured nutritional care into clinical practice should be considered. Given the practical challenges of conducting large-scale randomized trials of individualized nutritional interventions in this population, implementation-focused studies in real-world clinical settings may be particularly relevant.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Novo Nordisk Foundation. Major research project will help 50,000 Danes who have chronic obstructive pulmonary disease [Internet]. 2020 [cited 2021 21 February]. Available from: https://novonordiskfonden.dk/en/news/major-research-project-will-help-50000-danes-who-have-chronic-obstructive-pulmonary-disease/.
- 2Møgelberg N, Tobberup R, Møller G, Godtfredsen NS, Nørgaard A, Andersen JR. High-protein diet during pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Dan Med J. 2022;69(11).36331152 · pubmed ↗
- 3O’Leary K, Liu L, Mc Clure JB, Ralston J, Pratt W. Persuasive reminders for health self-management. AMIA Annu Symp Proc. 2016;2016:994–1003.PMC 533328928269896 · pubmed ↗
- 4Gonçalves B, Lusher J, Cund A, Sime C, Harkess-Murphy E. Understanding the psychosocial burden of living with advanced COPD in context of palliative care: a mixed methods study. J Health Psychol. 2025:13591053251316504.10.1177/13591053251316504 PMC 1253487940079249 · doi ↗ · pubmed ↗
- 5Engström CP, Persson LO, Larsson S, Sullivan M. Health-related quality of life in COPD: why both disease-specific and generic measures should be used. Eur Respir J. 2001;18(1):69–76.10.1183/09031936.01.0004490111510808 · doi ↗ · pubmed ↗