Neuromuscular electrical stimulation for early rehabilitation in critically ill patients: a systematic review of applied protocols
Nils Daum, Nils Drewniok, Annika Bald, Laura Homann, Linus Warner, Flora T. Scheffenbichler, Antonia Leder, Max Liebl, Anett Reißhauer, Tobias Wollersheim, Stefan J. Schaller, Steffen Weber-Carstens, Julius J. Grunow

TL;DR
This paper reviews how electrical stimulation is used to help critically ill patients during early rehabilitation, highlighting the lack of standardized protocols.
Contribution
The study systematically characterizes the diversity and inconsistency of NMES protocols used in ICU patient rehabilitation.
Findings
44 studies with 2,553 patients used 50 different NMES protocols, showing significant variability.
Lower limb muscles were most commonly targeted using biphasic rectangular waveforms with varying pulse durations and frequencies.
The lack of standardization in protocols hinders clinical comparisons and outcomes.
Abstract
Neuromuscular electrical stimulation (NMES) is increasingly used to mitigate negative consequences of bed rest in critically ill patients, especially those unable to actively participate in mobilization. However, existing studies have shown inconsistent outcomes, potentially due to heterogeneous NMES protocols. This systematic review aimed to identify and characterize the NMES protocols applied in this context. A systematic literature search was conducted in MEDLINE, Cochrane Library, Pedro, and CINAHL up to August 18, 2025. Studies were selected based on predefined PICOS criteria, focusing on adult intensive care unit (ICU) patients receiving NMES for early rehabilitation. Only randomized controlled trials and observational studies were included. Data on protocol parameters and patient characteristics were extracted and descriptively analyzed. 44 studies with a total of 2,553…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
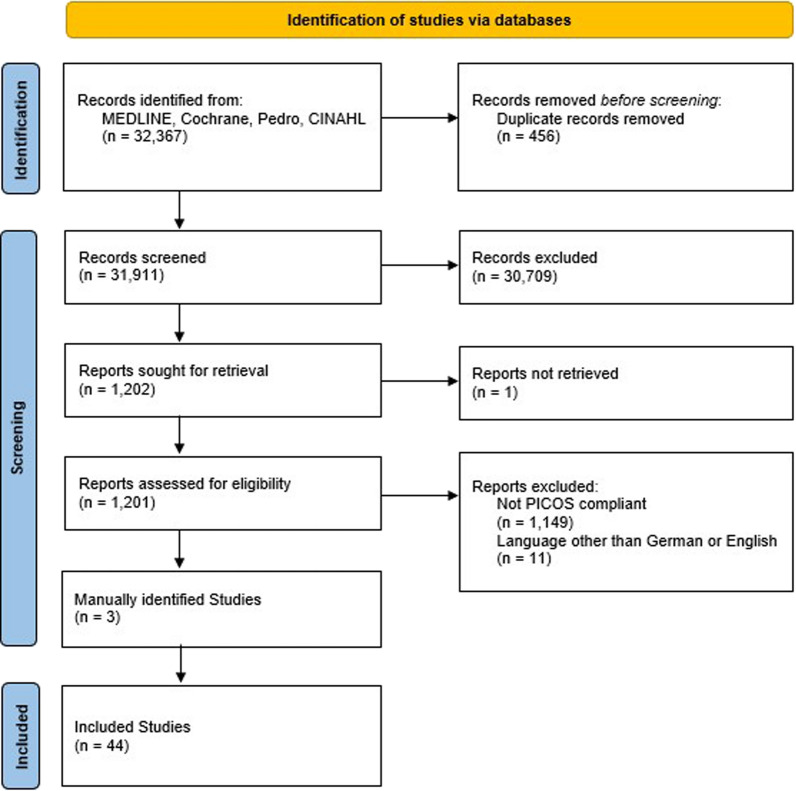 Figure 1
Figure 1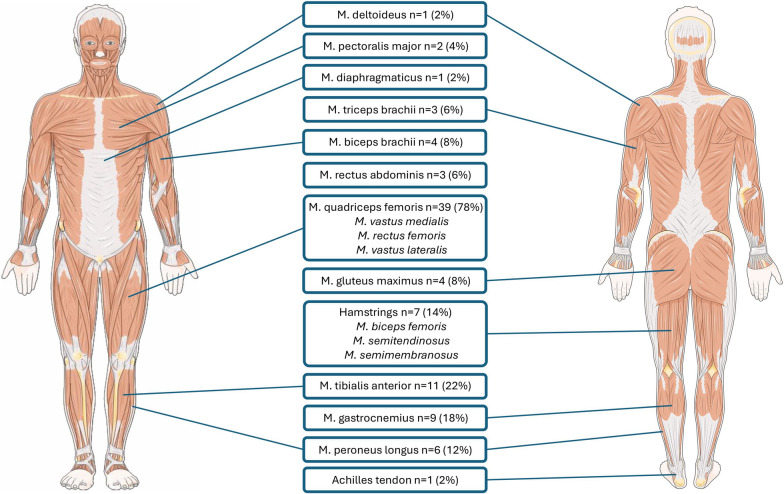 Figure 2
Figure 2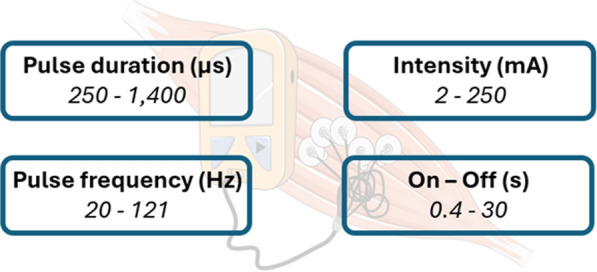 Figure 3
Figure 3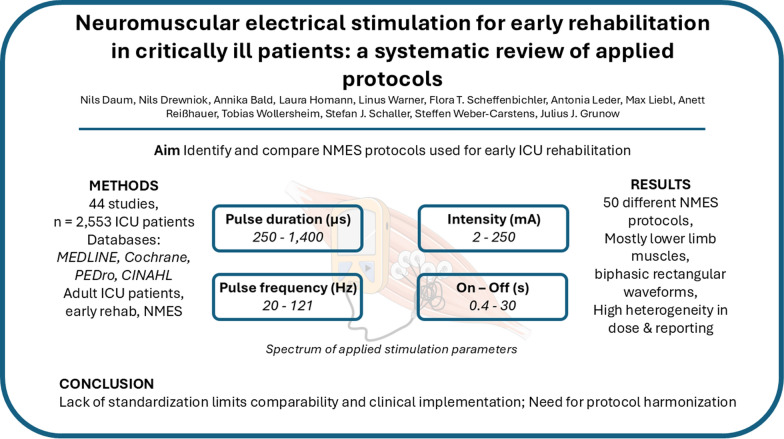 Figure 4
Figure 4- —Charité - Universitätsmedizin Berlin (3093)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Pressure Ulcer Prevention and Management · Planarian Biology and Electrostimulation
Introduction
Critical illness and intensive care unit (ICU) treatments are associated with short- and long-term physical impairments that substantially increase morbidity and mortality. Up to 80% of patients show physical impairments during the acute phase of critical illness [1], while increased mortality, delayed weaning from mechanical ventilation, prolonged hospitalization, and reduced quality of life are reported up to 5 years after discharge [2]. Therapeutic approaches to mitigate physical impairments include early mobilization. Early mobilization has been identified as a key intervention that can help prevent or mitigate the development of physical impairments by preserving neuromuscular function and promoting physical recovery in critically ill patients [3–7]. Additionally, early initiation of mobilization is crucial to positively impact the outcomes of critically ill individuals [8]. Active mobilization, as the most effective intervention, often encounters barriers in clinical practice, which are commonly linked to over-sedation [9, 10]. In these patients, active muscle contractions can be achieved through neuromuscular electrical stimulation (NMES), which employs electrical impulses to induce muscle contractions.
NMES has been incorporated into several international guideline recommendations as an adjunct to early mobilization [11–13]. Despite a considerable body of research, the available evidence remains inconsistent, which prevents the formulation of firm recommendations. This highlights a knowledge gap, as the effectiveness of NMES likely depends on standardized application. Studies and systematic reviews to date have yielded heterogeneous results, with some demonstrating clinical and molecular benefits while others showing no improvement [3, 8, 14–16]. Both EM and NMES share the commonality that the appropriate type and intensity of the intervention remain insufficiently studied [17, 18]. A potential source of the varying results might be the protocols used, which have never been systematically evaluated. Therefore, the aim of this systematic review was to identify and characterize different NMES protocols in ICU patients.
Methods
Protocol and registration
The protocol for this systematic review was registered on Open Science Framework (OSF) [19]. This study followed the Preferred Reporting Items for Systematic Reviews (PRISMA) reporting guidelines [20].
Selection criteria
Before the start of the systematic search, inclusion criteria were established by common consensus using the PICOS (participants, interventions, comparisons, outcomes, and study design) criteria (Table 1). Only full-text, peer-reviewed articles were included. Grey literature, conference abstracts, and unpublished studies were not considered, as detailed protocol descriptions were required for the objectives of this review.Table 1PICOS criteria for the inclusion criteria of the systematic literature reviewPCritically ill patients (≥ 18 years old) who were admitted to the ICUINeuromuscular Electrical Stimulation to improve muscle function or muscle massCStandard care or no stimulationOProtocol Parameters (e.g. Duration, Number of Sessions, Intensity (Minimal acceptable response, Maximal limit), Frequency, On-/Off-Time, Wave Length, Wave Form, Monopolar/bipolar, Muscle groups stimulated)SRandomized controlled trials (RCT) or observational studies
Studies were excluded if they met either of the following exclusion criteria:
- Studies that were not in the German or English language
- NMES with the goal of improving range of motion, spasticity or cardiovascular function
Information sources
The systematic search strategy was developed jointly by all authors, and after approval, the following databases were searched: MEDLINE via PubMed, Cochrane Library, Pedro, and CINAHL. The exact search strategy of the databases used is shown in Table A1 in the Appendix. The search extended from the inception of the respective database to August 18th, 2025. We additionally searched the reference list of review articles for relevant studies and added them manually.
Selection of studies
Two reviewers independently screened all studies from the systematic search by title and abstract for PICOS criteria using Rayyan [21]. Full-text articles were subsequently assessed for eligibility. Each study received two independent and blinded assessments, and disagreements were resolved by a third independent reviewer.
Data retrieval process
The included full texts were analyzed by one reviewer, and all relevant information was extracted. A second reviewer verified the accuracy of all transferred data. Data were obtained from both protocol descriptions and reported results whenever applicable, and any discrepancies between sources were resolved by consensus.
Data details and risk of bias
All relevant PICOS criteria were extracted from the included studies. In addition, we extracted study- and patient-specific characteristics. A descriptive analysis of the studies was performed. The risk of bias was assessed using the RoB-2 tool [22] for randomized controlled studies (RCTs) and ROBINS-E tool [23] for prospective studies. Two raters independently evaluated each study. In case of discrepancies, a third rater determined the final overall risk of bias.
Results
Selection of studies
Of the 32,367 studies screened, 44 met the inclusion criteria and were included in the descriptive analysis (Fig. 1).Fig. 1. Flowchart of the systematic search
Characteristics of included studies
A total of 40 included studies were designed as RCTs, including three that were explicitly conducted as pilot studies, and four as observational studies. Across these trials, a total of 50 distinct NMES protocols were applied to 2,553 patients. In five studies, two or more different NMES protocols were used concurrently (Table 2).Table 2. Study characteristicsAuthorYearStudy DesignSample Size (n)Study ArmsIntervention 1Intervention 2Intervention 3ControlAbu-Khaber [24]2013RCT80interindividualNMESUsual careAkar [25]2017RCT30interindividualNMES + PhysiotherapyNMES onlyPhysiotherapyBao [26]2022RCT60interindividualNMES (two muscles) + PhysiotherapyNMES (one muscle) + PhysiotherapyPhysiotherapyBaron [27]2022RCT149interindividualNMESUsual careBerney [28]2021RCT162interindividualNMES + CyclingUsual careCampos [29]2022RCT74interindividualNMESUsual careCerqueira [30]2018RCT59interindividualNMESUsual careDall’Acqua [31]2017RCT25interindividualNMESSham NMES + usual careDirks [32]2015RCT6intraindividualNMESUsual careDos Santos [33]2020RCT51interindividualNMES + PhysiotherapyPhysiotherapyNMESUsual careFalavigna [34]2013RCT11intraindividualNMESUsual careFigueiredo [35]2023OBS49interindividualNMES + CyclingNMES + CyclingFigueiredo [36]2024OBS20intraindividualNMES + CyclingNoneFischer [37]2016RCT54interindividualNMESSham NMESFossat [38]2018RCT312interindividualNMES + CyclingUsual careGerovasili [39]2009RCT49interindividualNMESUsual careGruther [40]2010RCT17interindividualNMESSham NMESGuerra-Vega [41]2025RCT52interindividualNMES (low frequency)NMES (moderate frequency)Usual careHirose [42]2013RCT15interindividualNMESUsual careKaratzanos [43]2012RCT52interindividualNMESUsual careKho [44]2015RCT34interindividualNMESSham NMESKourek [45]2024OBS16intraindividualNMESNoneKoutsioumpa [46]2018RCT80interindividualNMESUsual careLeite [47]2018Pilot RCT50interindividualNMESUsual careLiu [48]2023RCT80interindividualNMESUsual careMahran [49]2023RCT118interindividualNMESSham NMESMedrinal [50]2017RCT19intraindividualNMES + CyclingNMESCyclingUsual careMeesen [51]2010Pilot RCT19interindividualNMESUsual careNakamura [52]2019RCT37interindividualNMESUsual careNakanishi [53]2020RCT36interindividualNMESUsual careOthman [54]2023RCT120interindividualNMES + PhysiotherapyNMES alonePhysiotherapyUsual carePoulsen [55]2011RCT8intraindividualNMESUsual careRodriguez [56]2012RCT14intraindividualNMESUsual careRoutsi [57]2010RCT140interindividualNMESUsual careSegers [58]2021RCT47intraindividualNMESUsual careSilva [59]2017OBS11intraindividualNMESNoneSilva [60]2019RCT60interindividualNMESPhysiotherapyStefanou [61]2016RCT32intraindividualNMESNMESVerceles [62]2023RCT39interindividualNMES + High Protein NutritionUsual careVieira [63]2023RCT40interindividualNMESUsual careWaldauf [64]2021RCT150interindividualNMES + CyclingUsual careWollersheim [65]2019RCT50interindividualNMES ± whole body vibrationUsual careWoo [66]2018Pilot RCT10intraindividualNMES + CyclingCyclingZulbaran-Rojas [67]2022RCT16interindividualNMESUsual care*NMES *Neuromuscular Electrical Stimulation; OBS Observational study; RCT randomized controlled trial
Randomization was performed at the interindividual level in 33 studies, while ten studies implemented intraindividual randomization, for example, by applying different interventions to the right and left leg. In terms of study design, 37 studies employed a two-arm structure, three studies had a three-arm design, and three studies featured a four-arm design.
The most frequently investigated comparison was NMES in combination with standard care ("usual care") versus standard care alone. Three studies additionally compared both NMES plus standard care and NMES alone against standard care. In four studies, NMES was combined with passive or active cycling interventions; three studies specifically examined the additive effect of a combined NMES-cycling therapy. Further multimodal approaches included combinations of NMES with high-protein nutritional support, low- and moderate-frequency NMES, and whole-body vibration.
To control for potential placebo effects, five studies employed a sham NMES condition as a control. A detailed overview of the patient characteristics across studies is provided in Table A2 and A3 in the appendix.
Characteristics of NMES protocols
Analysis of the NMES protocols revealed a predominant focus on stimulation of the lower extremity. The quadriceps femoris muscle, including its components vastus lateralis, vastus medialis, and rectus femoris, was most frequently targeted (n = 39 (78%)). Other regularly stimulated muscles included the tibialis anterior (n = 11 (22%)), gastrocnemius (n = 9 (18%)), peroneus longus (n = 6 (12%)), and gluteus maximus (4 (8%)) (Table 3 and Fig. 2). In select cases, stimulation also targeted trunk muscles, such as the rectus abdominis (n = 3 (6%)), or upper limb muscles (n = 9 (18%)), most commonly the biceps brachii, triceps brachii, and pectoralis major (Fig. 2.).Table 3.NMES protocol parametersAuthorYearStimulated muscleWaveformPulse duration (µs)Pulse frequency (Hz)min. intensity (mA)max. intensity (mA)mean intensity (mean)On (s)Off (s)Minutes per dayStart after admission (days)Number of stimulations / dayNumber of sessions / patientAbu-Khaber [24]2013Quadricepsbiphasic, symmetric20050100****150na15na60na1naAkar [25]2017Deltoid / Quadricepsbiphasic, symmetrical, squarena502025na6nanana520Bao [26]2022Gastrocnemius / Tibialis anteriorbiphasic, asymmetrical, balanced rectangular300****30nanananana40****2–311–12naBaron [27]2022Gluteus maximussymmetric biphasic rectangular500****100nana45.8 (8.4)5**2525****263 (2–5)Berney [28]2021Rectus femoris / Hamstrings / Gluteus maximus / Gastrocnemiusnananananananana60nana5 (3–9)Campos [29]2022Quadriceps / Tibialis anteriorBiphasic and symmetrical rectangular400****80na120na51060**** < 25naCerqueira [30]2018Gastrocnemius / Quadricepsna4005017.5^a^** / 22.8**^b^79.1^a^** / 71.2**^b^49.5^a^** / 54.9**^b^3960****0510 (5–10)Dall’Acqua [31]2017Pectoralis Majorna300****50nana53 (15)3**1030na7naDall’Acqua [31]2017Rectus Abdominisna300****50nana68 (18)3**1030na7naDirks [32]2015Quadriceps / Rectus femoris / Vastus lateralisbiphasic, symmetric, rectangular wave pulse400****100nana29.9–32.33.51060****2.53–10naDos Santos [33]2020Rectus femoris / Vastus lateralis / Vastus medialisbiphasic symmetric400****45nanana126110****27.111.7Dos Santos [33]2020Quadricepsbiphasic symmetric400****45nanana126110****25.8 (3.1)10.3 (4.8)Falavigna [34]2013Quadriceps / Tibialis anteriorbiphasic, symmetric4005022^c^* / 18*^d^60^c^* / 48*^d^39.4^c^* / 30.4*^d^9920na10.2 (9)naFigueiredo [35]2023Quadriceps / Tibialis anterior / Hamstringsbiphasic, rectangular500–1,00050–10050****250nananananananaFigueiredo [36]2024Quadriceps / Tibialis anterior / Hamstringsbiphasic, rectangular500–1,00050–10050****250nanana11.3nananaFischer [37]2016Quadricepsbiphasic, rectangular40066*210040.5**(2–100)3.5**4.56014 (2–13)naFossat [38]2018Quadricepsnana30–75nanana**4–510–1454nananaGerovasili [39]2009Quadriceps / Peroneus longusbiphasic, symmetric**40045**1955**38 (10)126552nanaGruther [40]2010Quadricepsbiphasic, symmetric**35050nanana**82430^** g**^** / 60**^** h**^** < 7nanaGuerra-Vega [41]2025Quadricepsbiphasic40010018.677.547.45**104012naHirose [42]2013Quadriceps / Tibialis anterior / Biceps femoris / Triceps suraenanana**3040na**1010**3077–14naKaratzanos [43]2012Vastus lateralis / Vastus medialismedialis, and peroneus longusna**40045nanana**12655nana8 (6)Kho [44]2015Quadricepsbiphasic, asymmetrical, balanced rectangularwaveform,**40050nanana**510534.6 (1.8)nanaKho [44]2015Tibialis anterior / Gastrocnemiusbiphasic, asymmetrical, balanced rectangularwaveform,**25050nanana**55534.6 (1.8)nanaKourek [45]2024Vastus lateralis / Vastus medialis / Peroneus longus / Gastrocnemiusbiphasic, symmetric**400753086535**2145nananaKoutsioumpa [46]2018Quadricepsna**50050nanananana60nananaLeite [47]2018Vastus lateralis / Vastus medialis / Rectus femorisnana50nanana**83045nananaLiu [48]2023Pectoralis major / Rectus abdominis / Quadricepsna**30050nanana**31030na1naMahran [49]2023Rectus abdominis / Diaphragmnana30nanana**120**20255Medrinal [50]2017Quadricepsbiphasic, rectangular**30035nanananana10nananaMeesen [51]2010Rectus femoris / Vastus medialisbiphasic symmetric rectangular**250–33060–100na120na**7–1014–20**3011naNakamura [52]2019All lower extremitiesna**25020nanana**52**2021naNakanishi [53]2020Biceps brachii / Rectus femorissquare (positive) exponential decay (negative)**65020nana30^e^** / 41**^f^**0.40.630na5naOthman [54]2023Vastus medialis / Vastus lateralis / Rectus femorisbiphasic, asymmetrical, balanced rectangular**40050nanana**510**60215Poulsen [55]2011Quadriceps / Vastus medialisbiphasic**300352348314**660na77Poulsen [55]2011Quadriceps / Vastus lateralisbiphasic**300353754424**660na77Poulsen [55]2011Vastus medialis / Vastus lateralisbiphasic**30035nanana**46**603 (1–4)nanaRodriguez [56]2012Quadriceps / Vastus medialis / Biceps brachiibiphasic30010020 V200 V*na2460213 (7–30)naRoutsi [57]2010Vastus lateralis / Vastus medialis / Peroneus longusbiphasic40045nanana1265524–481naSegers [58]2021Vastus medialis / Rectus femoris / Vastus lateralisna35045na120758.512602–47naSilva [59]2017Gluteus maximus / Gastrocnemius / Hamstrings / Tibialis anterior / Quadricepsbipolar rectangular1,000100na6952–575515na3naSilva [60]2019Quadriceps / Hamstrings / Tibialis anterior / Gastrocnemiusna400100**nana65 (62–67)*52525na1naStefanou [61]2016Vastus lateralis / Vastus medialis / Peroneus longusbiphasic, symmetric, trapezoid**40075nanana**62140na7.6 (0.8)1Stefanou [61]2016Vastus lateralis / Vastus medialis / Peroneus longusbiphasic, symmetric, trapezoid**40045nanana**51240na7.6 (0.8)1Verceles [62]2023Quadriceps / Dorsiflexor muscles of lower extremitiesbiphasic**30030nanana**1010**60*** > 240.8 (0.3)10.1 (4.5)Vieira [63]2023Rectus femorisbiphasic, symmetric, rectangular40050nanana61255 < 2455Waldauf [64]2021Quadricepsna25040060**nanana31.1 (10.1)**2–36.56.5Wollersheim [65]2019Tibialis anterior / Triceps surae / Vastus lateralis / Biceps brachii / Triceps brachii / Wrist extensors / Wrist flexorsna350504070na6 or 1010 or 1520 < 3nanaWoo [66]2018Quadriceps / Rectus femorisbiphasic symmetric square25035nanana101220nananaZulbaran-Rojas [67]2022Gastrocnemius / Achilles tendonasymmetrical damped sinusoidal biphasic400–1,40020–12150 V250 Vnanana**60****1.8 (1.9)**114^a^Gastrocnemius; ^b^Quadriceps; ^c^Protocol begin; ^d^Protocol end; ^e^Biceps brachii; ^f^Rectus femoris; ^g^First week; ^h^After first week; Bold Data extracted directly from the methodology Italic Data extracted from the results Bold italic Definition of the unit used deviates from the standard measure; na not availableFig. 2Absolute and relative frequencies of stimulation protocols stratified by the respective muscle groups targeted
Most studies (n = 26 (52%)) employed biphasic electrical stimulation, with symmetric rectangular or trapezoidal waveforms (n = 6 (12%)) being the most common. Three studies specifically described a biphasic-asymmetric, balanced rectangular waveform (n = 3 (6%)); trapezoidal or exponentially decaying waveforms were reported in two studies (n = 2 (4%)).
Of the 50 NMES protocols identified, 44 (88%) explicitly reported the pulse duration in microseconds (µs), ranging from 250 to 1,400 µs. The stimulation frequency (Hz) was specified in 48 (96%) protocols, with values ranging from 20 to 121 Hz (Fig. 3).Fig. 3. Comprehensive overview of the spectrum of stimulation parameter settings applied
Stimulation intensity (mA) was documented in 26 (52%) protocols, with reported values between 2 and 250 mA. Two studies reported intensity in volts (V), further complicating cross-study comparability.
The duration of stimulation and rest phases (on-/off-times) varied considerably: on-times ranged from 0.4 to 12 s, while off-times ranged from 0.6 to 30 s. Daily stimulation duration was reported in 47 (94%) protocols and ranged from 10 to 110 min per day. The number of stimulation sessions per day and per patient ranged from one to fourteen sessions.
Risk of bias
The majority of included studies demonstrated a moderate to high risk of bias, with only three RCTs classified as having a low risk of bias (Table A4 and A5 in Appendix).
Discussion
The present systematic review highlights a considerable heterogeneity in the NMES protocols employed across the included studies. Particularly striking is the wide range of stimulation parameters used including pulse duration (µs), frequency (Hz), intensity (mA), and on/off times, which substantially limits the comparability of results and hinders robust conclusions regarding the efficacy of specific protocols.
Several RCTs investigated the application of NMES in critically ill patients and reported beneficial effects on the preservation of muscle mass [16]. In many cases, the intervention groups demonstrated reduced muscular atrophy compared to their respective control groups. Some studies also observed a significant reduction in hospital length of stay. However, a consistent, evidence-based benefit regarding muscle strength or functional outcomes (e.g., mobility, rehabilitation duration) has not yet been clearly demonstrated [8, 15].
While various meta-analyses indicate potential positive effects of NMES on clinical endpoints, other studies found no significant advantage compared to EM strategies without NMES, especially regarding ICU length of stay [8, 14, 15]. A major reason for these inconsistencies could be due to the pronounced methodological heterogeneity among the primary studies. Not only did the NMES interventions differ—ranging from isolated application to combination with other measures such as in-bed cycling or physiotherapy—but the type of control group also varied widely (e.g., standard care vs. sham NMES).
Substantial differences have been reported in the technical implementation of NMES. Stimulation intensity, for example, has not only varied considerably in magnitude but has also been expressed in different units (mA vs. V), which complicates comparisons across studies. In addition, several investigations provided insufficient methodological detail, or descriptions had to be inferred from the results, limiting interpretability and reproducibility. This heterogeneity likely represents a major reason for the divergent findings observed in NMES trials, as variations in stimulation protocols appear to directly influence surrogate outcomes such as muscle strength or endurance [29, 41, 68]. To address this issue, a standardized NMES reporting sheet has been proposed to ensure transparent documentation of stimulation parameters and responder rates, thereby enabling systematic comparisons across patient cohorts and trials. Importantly, the induction of visible muscle contractions has been identified as a prerequisite for clinical efficacy. In one analysis, a stimulation intensity of 50.1 mA was sufficient to reliably elicit a contraction in responders, with a sensitivity of 100% and a specificity of 84.6% [68]. However, the magnitude of the evoked muscle force represents the primary determinant of NMES-induced strength adaptations, with stronger contractions being associated with greater training effects [69]. Accordingly, a merely visible contraction likely reflects a lower contraction quality. Based on the classification proposed by Segers et al., visible contractions correspond to a Type 3 response, whereas higher-quality Type 5 contractions, defined as strong, palpable, and clearly visible activation of the full muscle bulk, may represent a more appropriate stimulation target [60, 70]. Thus, relying solely on visible contractions as a dosing criterion may result in suboptimal stimulation intensity and contribute to heterogeneous clinical effects across NMES studies. Nevertheless, many published studies applied substantially lower intensities, raising concerns about whether effective muscle activation was consistently achieved. Taken together, these findings underscore the need for harmonized reporting standards and protocol consistency. Only by ensuring adequate stimulation thresholds and transparent documentation will it be possible to generate comparable data, and ultimately clarify the true clinical value of NMES in critically ill patients.
These findings are reflected in current clinical guidelines, which, due to a lack of robust evidence, do not provide specific parameters for recommendation [11, 12]. The stimulation approaches employed in the included studies were so heterogeneous that evidence-based standardization is currently not feasible. This heterogeneity also substantially limits the interpretability of pooled effect estimates in meta-analyses, as meaningful comparison or synthesis across protocols becomes inherently challenging.
In sport science and studies in healthy populations, NMES is applied with more consistent and purpose-specific protocols. For muscle hypertrophy and strength, high-frequency (50–100 Hz), high-intensity stimulation at maximally tolerable levels, and pulse durations between 200 and 1,000 μs are typically used, with sessions performed 3 times per week over several weeks [71, 72]. Endurance-focused protocols typically apply lower stimulation frequencies (10–30 Hz) and intensities combined with longer duty cycles, which are intended to promote fatigue resistance rather than selective fiber-type recruitment. Importantly, NMES-induced muscle activation does not follow the physiological size principle; instead, muscle fibers are recruited in a non-selective and asynchronous manner once depolarization occurs, with simultaneous activation of type I and type II fibers. Thus, differences between endurance- and strength-oriented NMES protocols likely reflect distinct metabolic and fatigue-related adaptations rather than preferential recruitment of specific muscle fiber types [73, 74].
Based on our findings and the literature in healthy individuals, it seems meaningful to explore NMES protocols using longer pulse durations and moderate- to high-frequency stimulation, with intensities individually titrated to elicit effective muscle contractions in ICU patients [75, 76]. Importantly, the term “wide-pulse” refers to pulse duration (µs) and should be interpreted in relation to individual neuromuscular excitability rather than as a fixed threshold, as critically ill patients, particularly those with ICU-acquired polyneuromyopathy, may require substantially prolonged pulse durations to achieve muscle depolarization [59, 77, 78]. As highlighted in Fig. 3, the parameter ranges reported in ICU studies span from very low to very high values (pulse duration 250–1,400 μs; frequency 20–121 Hz; intensity 2–250 mA; duty cycles 0.4–30 s), underscoring the urgent need for systematic testing of parameter combinations tailored to this population. Translational studies are therefore required to define safe and effective stimulation settings for critically ill patients, which may help bridge the gap between experimental protocols in sport science and the heterogeneous approaches currently applied in the ICU [16, 68, 70, 79]. Importantly, the choice of outcome measures must be aligned with the underlying stimulation strategy. For example, lower-frequency protocols (e.g., 20–30 Hz), which have demonstrated positive effects in ICU populations, may be more appropriately evaluated using functional or endurance-related outcomes, whereas higher-frequency stimulation is better assessed using objective, strength-related measures that quantify muscle force or contractile capacity, potentially also depending on the underlying pathophysiology (e.g., CIP vs. CIM) [60, 80].
Despite different application methods, NMES is generally considered a safe intervention in critically ill patients. Several studies that specifically evaluated feasibility and safety have reported a low incidence of adverse events and good tolerability of NMES in the ICU setting. Compared to other mobilization techniques, such as conventional physiotherapy or in-bed cycling, NMES appears to be associated with a favorable safety profile [38, 59, 81]. In view of its positive effects and favorable safety profile, NMES appears to be a reasonable option for supporting the early rehabilitation of critically ill patients [11, 12]. This is particularly relevant for patients who are unable to participate in active mobilization due to deep sedation. NMES externally induces muscle contractions in patients who are unable to induce muscle contractions themselves, thereby offering a potential preventive strategy against physical sequelae acquired during the critical illness [32, 53].
Limitations
Importantly, this review intentionally focused on the description of applied NMES protocols rather than on the mechanistic rationale or primary endpoints of individual studies, in order to capture the full spectrum of stimulation strategies currently used in ICU practice. The main limitation of this review is the incomplete and inconsistent reporting of NMES parameters across the included studies, which reduces the level of detail available for analysis. Additionally, significant heterogeneity in study designs, patient populations, and control conditions greatly limits comparability and hinders a formal meta-analysis. Finally, many of the included trials were small or pilot studies, which limits the external validity and generalizability of the findings.
Conclusion
The findings of this systematic review highlight the lack of standardized NMES protocols for early rehabilitation in critically ill patients. The wide variation in stimulation parameters and their reporting currently hinders the development of a standardized, evidence-based treatment protocol. We suggest a practical framework for future testing in trials, following published reporting standards. Facilitating comparability across studies with standardized protocols and reporting will further strengthen evidence-based recommendations for NMES use. Based on the available evidence, NMES appears to be a feasible and generally safe adjunct to early rehabilitation in selected critically ill patients, particularly when active mobilization is not possible. However, its routine application in the ICU should currently be guided by individual patient characteristics, careful protocol selection, and realistic expectations regarding clinical benefit until more robust, standardized evidence becomes available.
Supplementary Information
Additional file 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Daum N, Drewniok N, Bald A, Homann L, Scheffenbichler F, Schaller SJ, Grunow J. Neuromuscular electrical stimulation for early rehabilitation in critically ill patients: a systematic review protocol of applied protocols. In: OSF Preprints. 2023.10.1186/s 13054-026-05873-6PMC 1293072241668181 · doi ↗ · pubmed ↗
- 2Rayyan. Intelligent systematic review. [https://www.rayyan.ai/].