Association of migraine with subsequent risk of depression or anxiety by small-area deprivation: national cohort study with sibling analysis
Emily White Johansson, Mattias Linde, Anna Ohlis, Mathias Mattsson, Ahmed Nabil Shaaban, Sofie Gustafsson, Johan Holm, Christina Dalman, Emilie E. Agardh

TL;DR
People with migraine are almost twice as likely to develop depression or anxiety, and this risk isn't significantly affected by the deprivation level of their neighborhood.
Contribution
This study provides a large-scale national analysis of migraine's association with depression or anxiety, using sibling comparisons to account for genetic and environmental factors.
Findings
Migraine is associated with a 1.78-fold increased risk of depression or anxiety in a matched cohort.
The risk remains elevated (1.63-fold) even after adjusting for shared genetics and childhood environments in sibling analyses.
Small-area deprivation does not significantly modify the risk of depression or anxiety among migraine patients.
Abstract
Growing evidence indicates that migraine could increase the risk of depression or anxiety in affected persons. Residential deprivation, with its links to stressful environments and access to quality services, could exacerbate the risk of developing depression or anxiety among migraine patients, but evidence remains limited. We aimed to examine the subsequent risk of depression or anxiety in persons with migraine and to determine if this association varies by small-area deprivation. A nationwide register-based cohort study was conducted of persons aged 10–50 years registered in Sweden from 2015 to 2023 who did not have recorded depression or anxiety in the previous ten years (n = 4,065,375). We generated matched (n = 1,455,352) and sibling (n = 179,888) samples for analyses. The exposure (migraine) and outcome (depression or anxiety) were defined as the first diagnosis, or the first…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
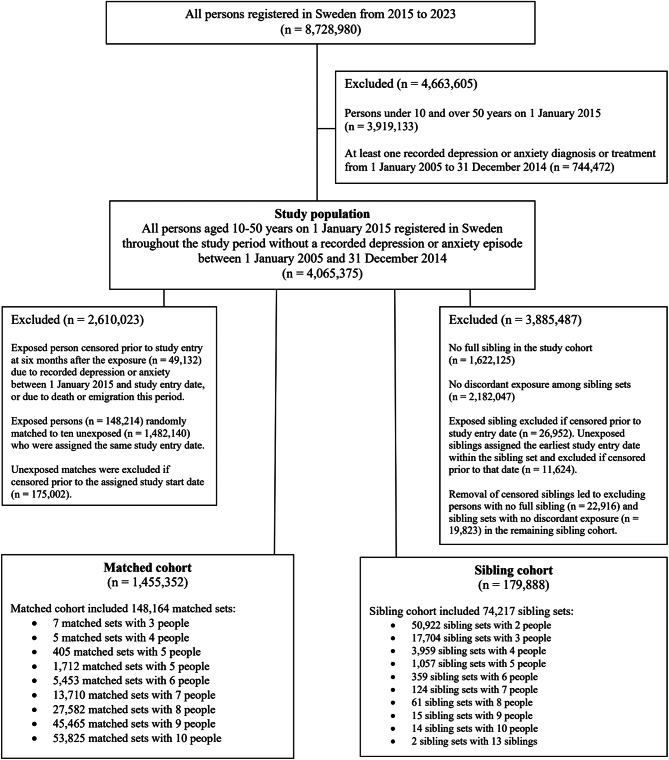 Figure 1
Figure 1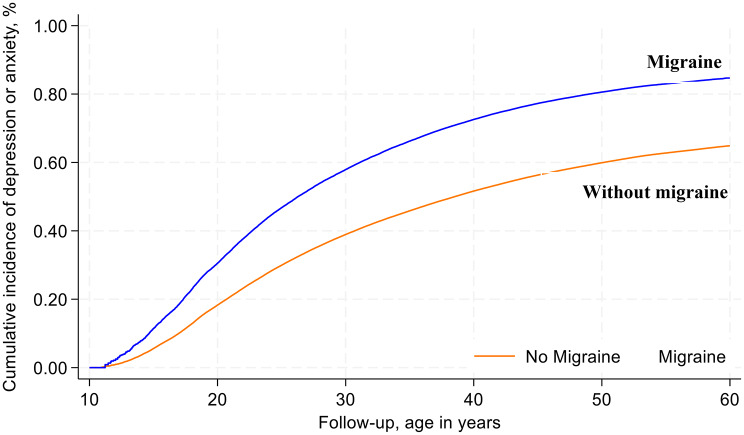 Figure 2
Figure 2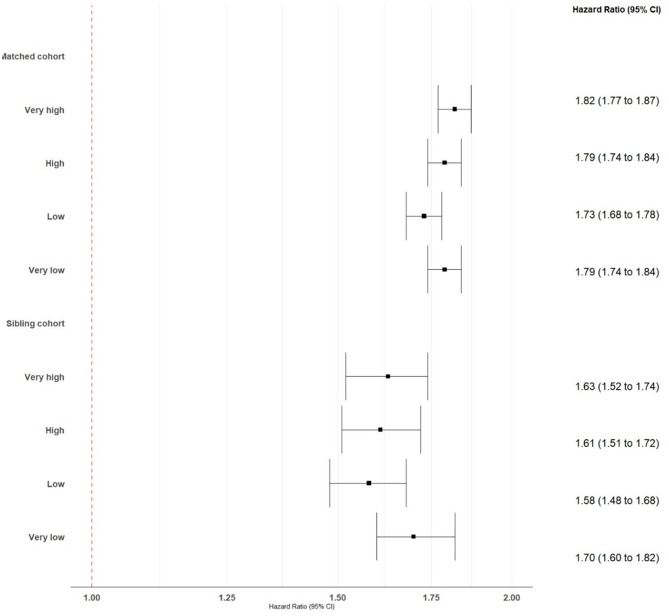 Figure 3
Figure 3- —Karolinska Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigraine and Headache Studies · Traumatic Brain Injury Research · Electromagnetic Fields and Biological Effects
Introduction
Migraine is the second leading cause of disability worldwide and affects more than one billion people annually [1]. In Sweden, it has been estimated that at least one in eight individuals experience migraine with women and people in lower socioeconomic groups disproportionately affected [2–4]. Migraine not only affects a person’s health and functioning, but may also lead to disruptions in social relationships, leisure time, school activities, ability to work, and income [5–7]. Furthermore, migraine is often co-morbid with depression or anxiety, further worsening health and wellbeing, working life, and relationships [8–15]. Similar to migraine, depression and anxiety are two major public health problems that often onset in adolescence or early adulthood and are more common in people with lower education or income levels [9, 16, 17].
A growing body of evidence shows the relationship between migraine, depression, and anxiety could be bidirectional with the conditions potentially exacerbating one another [8, 12, 15, 18]. Migraine may increase the risk of depression and anxiety, suggesting that severe pain could potentially lower a person’s quality of life leading to depressive symptoms [8, 12, 13]. There is also potential that the association between migraine and development of depression or anxiety is exacerbated by other known risk factors [9, 13, 16, 19–22], such as genetics or environmental conditions, but evidence remains limited.
Residential deprivation has long been established as an important driver of poor health outcomes including depression and anxiety [19, 23–27]. Residential deprivation refers to neighborhoods that are socioeconomically disadvantaged across multiple domains such as housing, employment, services, safety, or other resources [19, 23–27], which is referred to in this paper as small-area deprivation. Such deprivations are linked to stress levels, crime and violence, access to quality services, social cohesion, among other mechanisms that are known to influence depression or anxiety risk [23–25]. Yet evidence is lacking on whether small-area deprivation plays a modifying role in the potential bidirectional relationships between migraine, depression, and anxiety.
To help fill this evidence gap, this study aims to examine if people with migraine have increased subsequent risk of depression or anxiety and if the association differs according to small-area deprivation.
Methods
We conducted a national register-based cohort study with matched and sibling samples to examine the association between migraine and depression or anxiety among persons aged 10–50 years registered in Sweden between 2015 and 2023. The role of small-area deprivation was studied as a potential modifier in the risk of depression or anxiety among persons with migraine.
Data sources
Using a Swedish personal identification number uniquely assigned to each resident, the study linked multiple healthcare registers at the national and regional levels, including: (1) the Total Population Register for population and household statistics; (2) the National Prescribed Drug Register for prescription medications dispensed through Swedish pharmacies; (3) the National Multigenerational Register: and (5) the National Swedish Longitudinal Database for Health Insurance and Labor Market Studies for socioeconomic information for adult residents in Sweden. (6) the National Patient Register for data on the management of patients seen through inpatient and specialized outpatient care in Swedish hospitals; and (3) the Primary Healthcare Registers for data on the management of patients at regional primary healthcare centers. All registers had national coverage for the study period except the primary care registers that were available for 17 of 21 regions in the years 2015–2017, representing 89% of the Swedish population. The study received approval from the Ethical Review Authority in Sweden (2018/1339-31/5, 2018/2292-32, 2019–02185, 2021 − 00657, 2022-03111-02, 2023-07509-02, 2024-02816-02).
Study population
We identified all persons registered in Sweden throughout the study period from 2015 to 2023 who had a personal identification number assigned at birth or immigration, and a primary address assigned to one of 5,984 small geographical divisions established by Statistics Sweden (DeSO) (Fig. 1) (n = 8,728,980) [28, 29]. We restricted the study cohort to people aged 10–50 years (n = 3,919,133) since migraine onset typically occurs within this age range and there is broad homogeneity in the pathophysiology and management of the three conditions within this age range [8]. We further excluded 744,472 people diagnosed with or treated for depression or anxiety between 1 January 2005 and 31 December 2014, or ten years prior to the study start on 1 January 2015 (Table S1-S2). This was done to further establish a temporal relationship between exposure and outcome in our analysis. The final study population included 4,065,375 individuals.
Fig. 1. Flow diagram of inclusion criteria for the study population and sampled cohorts
Matched and sibling cohorts
From the study population, we generated separate matched and sibling samples for analysis purposes. The age- and sex- matched cohort was generated by identifying the 197,346 exposed person in the study population and excluding those who were censored prior to entering follow-up at six months after their first recorded migraine (n = 49,132). Persons were censored prior to study entry if they had recorded depression or anxiety between 1 January 2015 and their study entry date, or who died or emigrated during this time. A total of 148,214 exposed persons were randomly matched to ten unexposed based on sex and five-year age groups (n = 1,482,140). All persons in each matched set were assigned the same study entry date, which was six months after the first recorded migraine date for the exposed person in the matched set. We excluded any unexposed matches who were censored prior to the follow-up start date for the reasons previously described (n = 175,002). The final sample for the matched cohort was 1,455,352 persons including 148,164 matched sets.
The sibling cohort was separately generated by identifying full siblings in the study population who had the same mother and father in the Swedish Multigeneration Register. We excluded people with no full sibling (n = 1,622,125) and sibling sets with no discordant exposures (n = 2,182,047). As per the matched cohort procedure, we excluded exposed siblings who were censored prior to entering follow-up at six months after their first recorded migraine exposure (n = 26,952). Unexposed siblings were assigned the earliest exposure date within the sibling set and excluded if censored prior to this study entry date (n = 11,624). The removal of censored siblings led to excluding persons in the remaining cohort with no full sibling (n = 22,916) and sibling sets with no discordant exposure (n = 19,823). The final sample for the sibling cohort was 179,888 persons including 74,217 sibling sets.
Migraine measurement
Migraine was defined as the first diagnosis date in primary, specialist outpatient or inpatient care, and if no diagnosis was recorded during the study period, the first prescription date for a dispensed drug. Table S3 lists the diagnosis and prescription codes that measured the exposure based on the Swedish adaptation of the International Statistical Classification of Diseases and Related Health Problems, 10th version (ICD-10-SE) and the Anatomical Therapeutic Chemical (ATC) classification system, respectively. Migraine diagnoses were derived from any inpatient admission or specialist outpatient visit recorded in the National Patient Register during the study period, and any primary care visit in 17 of 21 regions from 2015 to 2017 when data were available. If the date of diagnosis (day and month) was missing, we imputed the date using the earliest prescription date in the year of the visit. If there was no prescription that year, the midpoint date in the year of the visit was used for the diagnosis date. Study participants without recorded migraine as previously described comprised the comparison group.
Depression or anxiety measurement
Depression or anxiety was defined as the first diagnosis date in primary, specialist outpatient or inpatient care, and if no diagnosis was recorded in the study period, the first prescription date for a dispensed drug. Table S2 lists the ICD-10-SE and ATC codes that measured the outcome in administrative registers. Depression or anxiety diagnoses were derived from any inpatient admission or specialist outpatient visit during the study period, and any primary care visit in 17 of 21 regions from 2015 to 2017 when data were available. If the diagnosis date was missing (day and month), we imputed the date using the earliest prescription date in the year of the visit. If there was no prescription in that year, the midpoint date in the year of the visit was used for the diagnosis date.
Small-area deprivation level
We used the Index for Multiple Deprivation in Sweden (IMDIS) to estimate small-area deprivation level for each of the 5,984 DeSO areas in the year 2015 [30]. IMDIS has been previously described elsewhere [30]. Briefly, IMDIS is a composite index of deprivation that aims to measure four domains using 15 indicators: (1) income and capital (2) education (3) employment (4) housing. An IMDIS valued based on this composite measure was assigned to each DeSO, which was then ranked from least to most deprived and categorized into quartiles using the 25th, 50th, and 75th percentiles (very low, low, high, and very high deprivation levels). Each person was assigned the deprivation level of the DeSO for their primary address in the Total Population Register in the year of their study entry. We assumed the deprivation level assigned to each DeSO in the year 2015 remain unchanged across the study period that could lead to exposure misclassification if residential area characteristics changed over time. Previous research has shown that nearly 80% of Stockholm neighborhoods had stable socioeconomic profiles from 1990 to 2015 [31]. While this research does not cover all of Sweden or the most recent period from 2015 onwards, it does suggest that the vast majority of the nearly 6,000 small geographic areas in our analysis could likely be classified into the same deprivation quartile during the study period.
Other covariates
Other regression covariates included age in the year of study entry (continuous), sex (male or female), area of residence in the year of study entry (urban, peri-urban, rural), and birthplace (Sweden, Nordic outside Sweden, European Union (EU28) outside Nordic, Europe outside EU28 and Nordic, or another birthplace) derived from the Total Population Register. Area of residence was defined by Statistics Sweden and derived from the DeSO assigned to each study participant.
Statistical analyses
For matched and sibling cohort analyses, we separately calculated unadjusted rates of depression or anxiety per 1,000 person-years for participants with or without migraine. Person-years at risk were computed from the start of follow-up until date of outcome, death, emigration, or study end on 31 December 2023, whichever occurred first. Cumulative incidence rates for depression or anxiety among participants with or without migraine were plotted using the Kaplan-Meier method and compared using the log rank test.
Stratified cox proportional hazards models with robust error variance and separate strata for each sibling or matched set were used to compute hazard ratios (HR) with 95% confidence intervals (CI) for the association between migraine and the outcome, using no migraine as the reference category. We tested the proportional hazards assumption by inspecting the log minus log survival plot in matched and sibling cohorts (Figures S1-S2). Final models were adjusted for small-area deprivation level, age, sex, area of residence, and birthplace. We used a Wald Test to determine if there was an interaction between migraine and small-area deprivation level in the adjusted models of the matched and sibling cohorts. The level of statistical significance was set to 0.05. We analyzed data using Stata 18 (StataCorp, College Station, TX).
Sensitivity analyses
We conducted two sensitivity analyses for this study. In the first sensitivity analysis the definition of the outcome was restricted to diagnoses only, and prescribed depression or anxiety drugs (without a diagnosis) were omitted from the definition since some antidepressants may be used to treat other conditions, such as chronic pain. In the second sensitivity analysis, the outcome was defined without primary healthcare data since these data were not available throughout the study period or for all regions.
Results
Among the 4,065,375 participants, 4.9% had recorded migraine between 2015 and 2023 (Table 1). There was limited variation in this proportion across small-area deprivation levels. The median age of participants with migraine was 30 years (IQR: 21–41) and three times as many women had migraine than men in the study population. The matched sample had a similar exposure distribution to the study population across all covariates except those used for matching. The sibling sample, in comparison to the study population, had a higher proportion of men, native-born Swedes, rural and peri-urban residents, and residents in less deprived areas.
Table 1. Characteristics of the study population and sampled cohorts by migraine statusStudy populationMatched cohortSibling cohortMigraineNo MigraineMigraineNo MigraineMigraineNo Migraine N % N % N % N % N % N %Total197 346100.03 868 029100.0148 214100.01 307 138100.076 239100.0103 649100.0Age,** median (IQR)**30(21–41)30(20–41)34(25–44)34(24–44)32(23–42)31(23–42) Sex Male52 84726.82 116 77854.743 27829.2401 23730.722 24329.260 00957.9Female144 49973.21 751 25145.3104 93670.8905 90169.353 99670.843 64042.1 Small-area deprivation Very low deprivation50 95025.81 004 12926.039 22526.5338 60125.921 52628.226 77925.8Low deprivation50 41925.6984 06825.437 86725.6331 78025.420 68927.127 16726.2High deprivation48 79924.7962 37224.936 06824.3324 11024.818 79224.726 30125.4Very high deprivation47 17823.9917 46023.735 05423.7312 64723.915 23220.023 40222.6 Area of residence Urban153 93878.02 965 18676.7115 33577.81 010 35777.357 92275.277 97676.0Peri-urban16 5508.4329 6948.512 4678.4108 3868.36 8348.99 2259.0Rural26 85813.6573 14914.820 41213.8188 39514.411 48315.916 44815.1 Birthplace Sweden159 91381.33 144 71581.3119 92980.91 048 92780.371 06693.294 22890.9Nordic outside Sweden2 3091.143 2781.11 7921.215 5421.23540.54890.5EU28 outside Nordic5 7633.4130 0013.44 3092.945 5543.54870.67100.7Europe outside EU286 1132.8109 6972.84 5153.138 3112.91 1781.62 0662.0Other birthplace23 24811.4440 33811.417 66911.9158 80412.23 1544.16 1565.9
Matched analysis
During 7,214,949 person-years of follow-up, a total of 169,733 individuals had a depression or anxiety episode (median time at risk: 5.4 years) (Table 2). Among participants with the outcome, 26,521 had migraine corresponding to an incidence rate of 39.2 episodes per 1,000 person-years (95% CI: 38.7–39.6) compared to 21.9 per 1,000 person-years (95% CI: 21.8–22.0) for people without migraine. Cumulative incidence curves on the matched cohort showed consistently higher probability of developing depression or anxiety among people with migraine versus those without migraine across the study duration (Fig. 2). Overall, migraine was associated with a 1.78 (95% CI: 1.75–1.81) higher rate of depression or anxiety compared to no migraine in adjusted models across the study period (Table 2).
Fig. 2. Kaplan-Meier cumulative incidence rates of depression or anxiety through 31 December 2023 among the matched cohort
Sibling analysis
The sibling analysis included 862,613 person-years of follow-up with a total of 23,612 full siblings experiencing depression or anxiety across the follow-up period (Table 2). Among siblings with depression or anxiety, 13,250 siblings had migraine corresponding to an incidence rate of 37.7 episodes per 1,000 person-years (95% CI: 37.0-38.3) compared to 20.3 per 1,000 person-years (95% CI: 19.9–20.7) for siblings without migraine. In the sibling analysis, migraine was associated with a 1.63 (95% CI: 1.58–1.68) higher rate of depression or anxiety compared to no migraine in adjusted models across the study period.
Table 2. Association between migraine and depression or anxiety through end-2023 in the matched and sibling cohortsPersons entering follow-upDepression or anxiety episodesPerson-years at riskRate of depression or anxiety episodesHazard ratios (95% CI) N
N
N per 1,000 person-yearsCrudep-valueAdjustedp-value Matched sample
1 455 352
169 733
7 214 949 Person with migraine148 21426 521677 41839.2 (38.7–39.6)1.78 (1.76–1.81)< 0.0011.78 (1.75–1.81)< 0.001Person with no migraine1 307 138143 2126 537 53121.9 (21.8–22.0)1.001.00 Sibling sample
179 888
23 612
862 613 Sibling with migraine76 23913 250351 73237.7 (37.0–38.3)1.89 (1.83–1.94)< 0.0011.63 (1.58–1.68)< 0.001Sibling with no migraine103 64910 362510 88120.3 (19.9–20.7)1.001.00Note: Hazard ratios were estimated using stratified Cox regression models with strata for each matched or sibling set and robust error variance. Adjusted hazard ratios accounted for age, sex, small-area deprivation, area of residence, and birthplace. For the matched cohort, persons with migraine were matched to ten unexposed by sex and five-year age-bands. For the sibling cohort, siblings with migraine were matched to unexposed siblings
Interaction between small-area deprivation and migraine on risk of depression or anxiety
There was no overall evidence of an interaction between migraine and small-area deprivation level on the subsequent risk of depression or anxiety in the matched (p = 0.123) or sibling (p = 0.422) cohorts. In the matched cohort, the interaction term between low and very high deprivation levels was not significant (p = 0.089) although the CIs across these deprivation levels had limited overlap (Fig. 3).
Fig. 3. Associations between migraine and depression or anxiety through end-2023 in the matched and sibling cohorts of persons aged 10–50 years registered in Sweden in 2015–2023, by small-area deprivation
Sensitivity analysis
In the sensitivity analysis that used a stricter definition without drug exposure for depression and anxiety (Table S4), there were 7,565,649 person-years of follow-up in the matched cohort and a total of 83,418 people diagnosed with the outcome. After adjustment, the HR for depression or anxiety associated with migraine was 1.73 (95% CI: 1.70–1.76) across the study duration. In the sensitivity analysis that did not include primary healthcare data, an adjusted HR for depression or anxiety associated with migraine of 1.96 (95% CI: 1.93–1.99) was found in the matched cohort (Table S5).
Discussion
Principle findings
In this national register-based cohort study with matched and sibling analyses, we found that people who were depression- or anxiety-free for the ten years prior to their migraine diagnosis had a higher subsequent risk of these conditions compared to people without migraine. This association was lower but remained significant in the sibling analysis that further adjusted for shared genetics and childhood family environments. We found no evidence for the modifying role of small-area deprivation in the development of depression or anxiety among migraine patients in our cohort. This important research area merits further investigation, particularly in settings with larger socioeconomic disparities across residential areas.
Comparisons with other studies
The comorbidity of depression, anxiety and migraine symptoms is well-documented [8, 9, 11–13, 15, 32], although the reason for this overlap is less well understood [8, 13]. A growing body of evidence suggests a bidirectional relationship between the three conditions with one or more conditions inducing the other(s) [18, 33]. Recent research has shown that people with migraine had increased risks of affective or anxiety disorders [8, 33, 34].
Our study expanded on previous research by analyzing matched and sibling samples drawn from a national cohort to examine the associated subsequent risk of depression or anxiety among migraine patients with no recent history of these conditions. We found a nearly two-fold higher rate of depression or anxiety among people with migraine in the matched cohort. When accounting for shared childhood family environment and genetic factors, which are known risk factors for all three conditions, the association remained but was slightly weaker in the sibling analysis.
Building on this evidence, our study is the first to our knowledge to examine if living in a highly deprived area exacerbates the subsequent risk of depression or anxiety in migraine patients. Residential deprivation itself has been shown to increase the risk of depression or anxiety in previous research from Sweden and elsewhere [24, 26], yet there has been limited evidence of its potential modifying role in any bidirectional relationship. It is plausible that a bidirectional relationship between migraine with depression or anxiety could be influenced by residential deprivation given its known links to stress, crime and violence, access the quality services, social cohesion, among other environmental factors [35–38]. Yet, we found no overall role of small-area deprivation in modifying the relationship between migraine and the subsequent risk of depression or anxiety in our cohort. Our analysis tested multiplicative interactions on the hazard ratio scale, and this does not exclude absolute risk differences between deprivation quartiles. It is also possible that our matched and sibling cohorts did not have sufficient power to detect effect differences across deprivation levels, or that persons excluded from the study population with prior depression or anxiety were correlated with greater residential deprivation further obscuring these results. In addition, a separate cross-sectional analysis of this study population showed higher migraine prevalence in residents of the least-deprived areas [39], potentially due to having more health system contacts for migraine diagnosis and treatment. In contrast, previous research suggests an opposite relationship for small-area deprivation and depression or anxiety prevalence [22, 24]. Taken together, these results suggest a more complicated role for small-area deprivation in the development of these conditions and potentially in terms of modifying any potential bidirectional relationship. Further research is needed to better elucidate to what extent, if any, social and environmental conditions may modify how these conditions relate to one another.
Strengths and limitations of this study
This study leveraged multiple national and regional registers to enable research on a whole population basis providing greater statistical power for analyzing matched and sibling cohorts, stratifying by small-area deprivation level, minimizing risk of selection bias, and allowing for a longer and more complete follow-up period. There are also some study limitations. First, the study relied on administrative registers to ascertain exposure and outcome status in the population that may undercount and misclassify cases due to well-recognized gaps in care-seeking and appropriate management of these conditions. Misclassification of migraine, depression and anxiety from register data, including under-ascertainment, may disproportionately affect men and milder cases. In addition, regional primary care registers were only available for 17 of 21 regions (89% national population) and for the years 2015 to 2017. This will likely underestimate the prevalence of all three conditions in the current study and could potentially impact associations found if the three conditions are differentially diagnosed in primary versus specialist or inpatient care where measurement is at the national level, or if drugs are prescribed in ways that are systematically different across the conditions. A large proportion of cases were ascertained from prescription registers alone. We included only migraine drugs that did not have multiple indications, and the registers do not include over- the-counter drugs used to treat migraine. In contrast, antidepressants could be prescribed for other conditions, e.g., chronic pain, and we aimed to account for this issue in sensitivity analysis using diagnosed cases only. Second, observational studies are prone to residual confounding that makes causal inferences difficult. Migraine may not directly cause depression or anxiety, and the associations found in our study may be due to unmeasured risk factors associated with both the exposure and outcome. For example, people with migraines may have more contact with the healthcare system than undiagnosed people and could thus be more likely to get diagnosed with other conditions such as depression or anxiety. The sibling analysis could partially adjust for healthcare seeking behaviors learned in a shared childhood family environment, but residual confounding likely remains. Fourth, while sibling analyses may reduce confounding bias from shared genetic and other unmeasured factors in the childhood family environment, sibling comparisons are prone to carryover effects and may also lead to different associations from the matched comparison due to poor generalizability and varying distributions of other confounders in the sibling versus matched samples. Sibling samples may also undercount immigrant families with siblings who may not be resident in Sweden or sought healthcare here. Fifth, contextual factors such as small-area deprivation have measurement challenges including defining the area or developing indicators, and composite deprivation measures could obscure differences in areas even within the same level. Sixth, our study excluded people with depression or anxiety in the previous ten years, which may introduce selection or collider bias and change the demographic composition of our study cohort compared to the general Swedish population. This bias could attenuate both the overall association between migraine and the outcome as well as the interaction by small-area deprivation if depression or anxiety is correlated with living in more deprived areas. It is also possible that persons may be misclassified as having no prior mental health conditions if they did not seek care or were treated outside Sweden in the past ten years. Finally, small-area deprivation level for each DeSO was measured in 2015 and the quartile grouping was assumed to remain unchanged throughout the study period.
Conclusions
People with migraine have a higher subsequent risk of depression or anxiety than those without migraine, and this association remained but was lower in sibling analyses after adjusting for shared genetic factors and childhood family environments. We found no evidence of a modifying role for small-area deprivation in the subsequent risk of depression or anxiety among migraine patients, although further investigation is merited.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Viudez-Martínez A, Torregrosa AB, Navarrete F et al (2024) Understanding the biological relationship between migraine and depression. Biomolecules 30(2). 10.3390/biom 1402016310.3390/biom 14020163 PMC 1088662838397400 · doi ↗ · pubmed ↗
- 2Buse DC, Reed ML, Fanning KM et al (2020) Comorbid and co-occurring conditions in migraine and associated risk of increasing headache pain intensity and headache frequency: results of the Migraine in America Symptoms and Treatment (MAST) study. J Headache Pain 21(1):23. 10.1186/s 10194-020-1084-y 10.1186/s 10194-020-1084-y PMC 705310832122324 · doi ↗ · pubmed ↗
- 3Li B, Allebeck P, Burstöm B et al (2023) Educational level and the risk of mental disorders, substance use disorders and self-harm in different age-groups: a cohort study covering 1,6 million subjects in the Stockholm region. Int J Methods Psychiatr Res 32(4):e 1964. 10.1002/mpr.196410.1002/mpr.1964 PMC 1069881536802082 · doi ↗ · pubmed ↗
- 4Kosidou K, Dalman C, Lundberg M et al (2011) Socioeconomic status and risk of psychological distress and depression in the Stockholm Public Health Cohort: a population-based study. J Affect Disord 134(1–3):160-7. 10.1016/j.jad.2011.05.02410.1016/j.jad.2011.05.02421665286 · doi ↗ · pubmed ↗
- 5van der Velde L, Shabaan AN, Mattsson M et al (2025) An index of multiple deprivation in Sweden: measuring area-level socio-economic inequalities. Eur J Public Health 29. 10.1093/eurpub/ckaf 13810.1093/eurpub/ckaf 138PMC 1270747940882978 · doi ↗ · pubmed ↗
- 6Antonaci F, Nappi G, Galli F et al (2011) Migraine and psychiatric comorbidity: a review of clinical findings. J Headache Pain 12(2):115 – 25. 10.1007/s 10194-010-0282-410.1007/s 10194-010-0282-4PMC 307248221210177 · doi ↗ · pubmed ↗
- 7Johansson EW, Shaaban AN, Linde M, et al (2026) Geographical patterns and determinants of migraine in persons aged ten years or older living in Sweden from 2015 to 2023: a nationwide cross-sectional study. J Headache Pain 27:50. 10.1186/s 10194-026-02287-110.1186/s 10194-026-02287-1PMC 1291855441714942 · doi ↗ · pubmed ↗