Caregiver-reported good practices and their associations with care-recipient condition in dementia care: a text-mining study
Hiroyuki Tanaka, Masahiro Tenjin, Haruka Atosako, Yuma Nagata, Daiki Ishimaru

TL;DR
This study identifies and validates good practices in dementia care reported by caregivers, using text mining and expert validation to create a training resource.
Contribution
A validated list of 72 good practice items in dementia care derived from caregiver reports and expert consensus.
Findings
Keywords like 'voice', 'explanation', and 'eye contact' were frequently associated with good practices in dementia care.
Co-occurring clusters revealed context-specific practices, such as 'explanation' and 'menu' for eating and 'confirmation' and 'temperature' for bathing/dressing.
72 out of 79 extracted good practice items met the content validity ratio threshold after expert evaluation.
Abstract
Dementia care requires specific “good practice” actions, which often involve tacit knowledge possessed by experienced caregivers. This study extracts and verifies caregiver-reported good practice actions that improve the condition of people with dementia and compiles them into a structured list. An online survey was conducted on Japanese care and medical professionals (nurses, care workers, therapists, and care managers). Participants answered questions on basic attributes, dementia attitude scales, dementia knowledge scales, and the Approaches to Dementia Questionnaire (ADQ) and provided free-text descriptions of good practice in six care situations: eating, mobility/transfer, hygiene, toileting, bathing/dressing, and communication Free-response comments were analyzed using KH Coder, as follows: (1) cooccurrence network analysis was performed to identify clusters of related terms, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
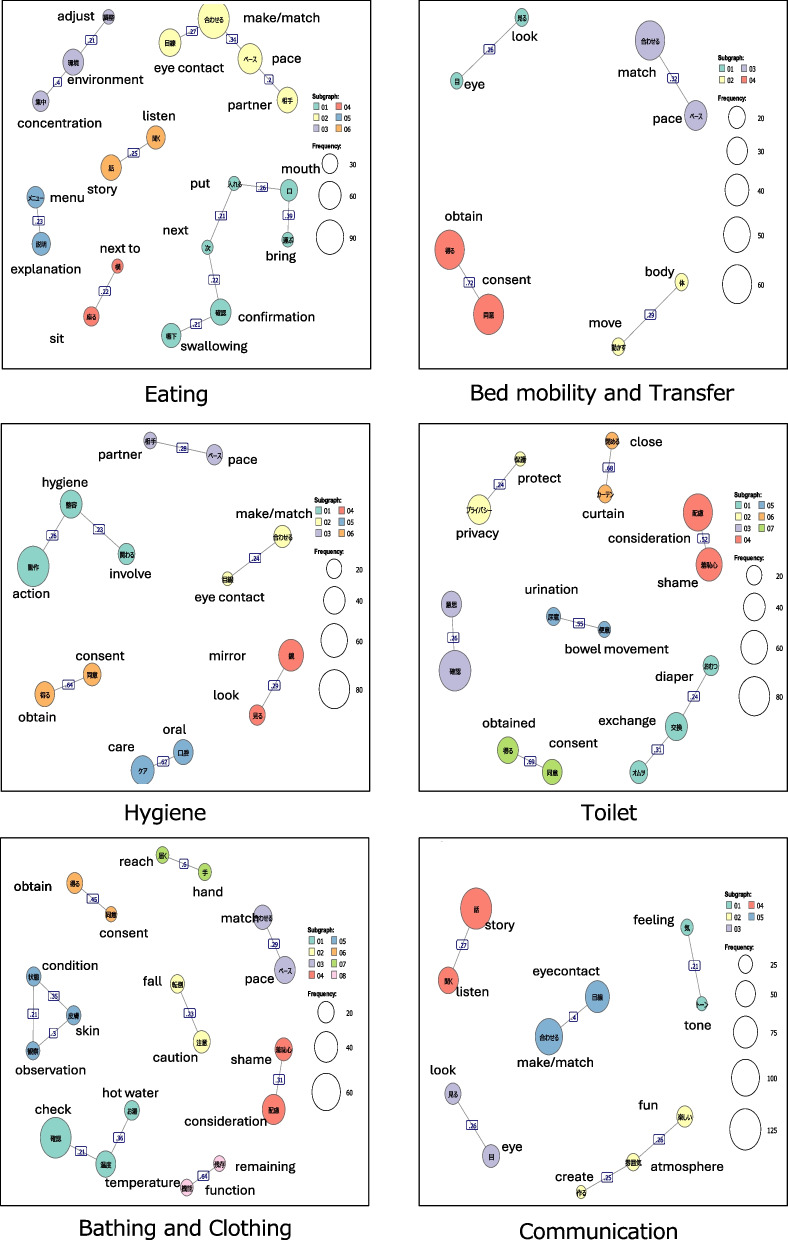 Figure 1
Figure 1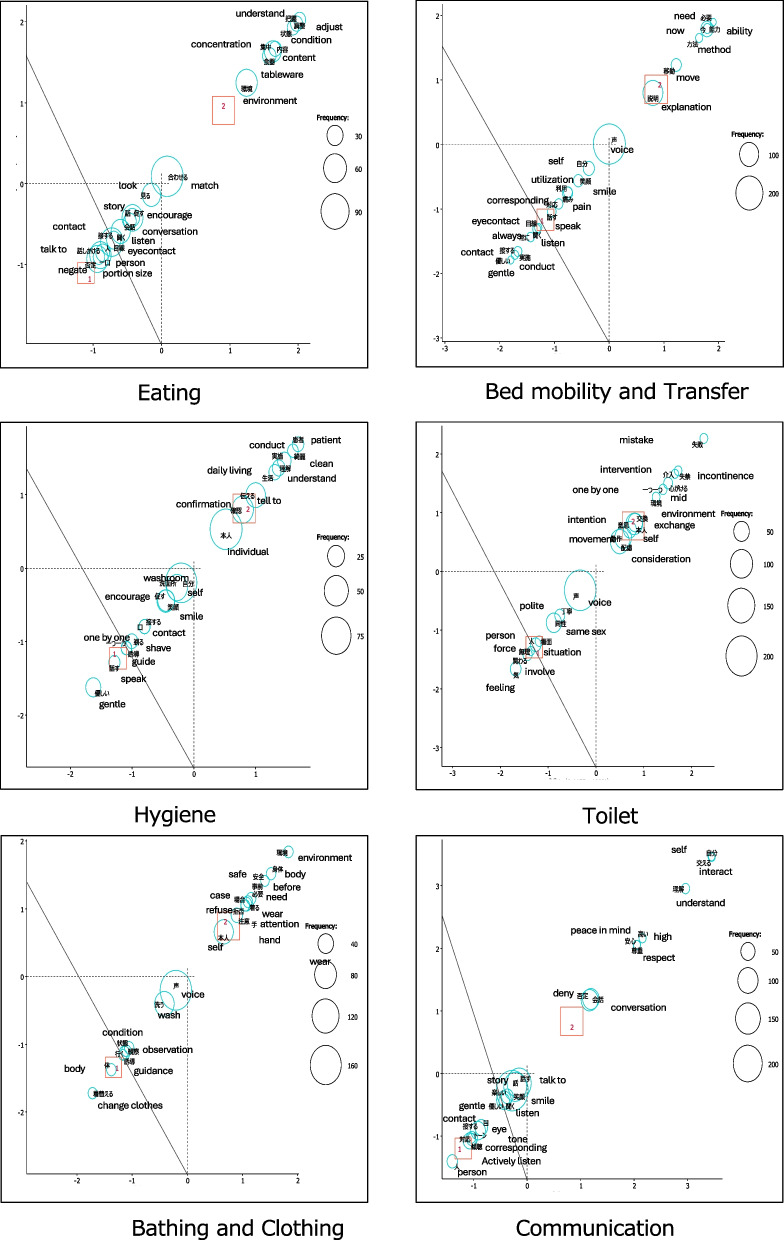 Figure 2
Figure 2- —JSPS KAKENHI Grant-in-Aid for Scientific Research
- —Research Foundation for Dementia Osaka
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDementia and Cognitive Impairment Research · Nutrition and Health in Aging · Education, Healthcare and Sociology Research
Background
Supporting the autonomy, dignity, and personhood of individuals living with dementia using “good practice” actions is essential and extends beyond symptom management [1]. The identification of good practice actions to care for and interact with people with dementia enhances frontline caregivers’ skills, preserves care recipients’ dignity, and improves the recipients’ quality of life (QoL) [2, 3]. In particular, providing support for essential basic activities of daily living (ADLs), such as eating and toileting, upholds care recipients’ dignity and self-efficacy, enhances their QoL, and reduces their confusion and anxiety [4]. These good practice actions must be clearly defined to ensure that care staff have the required practical guidance to maintain and improve care quality.
Moreover, research on Dementia Care Mapping underscores the importance of caregivers knowing how to interact with patients in everyday situations [5]. In their study, Gkioka et al. trained hospital staff in specific communication strategies for person‐centered care (PCC) and reported the subsequent occurrence of behavioral changes, highlighting the importance of structuring care actions and presenting them in a shareable format [6]. However, applying this theory in everyday practice remains challenging [7]. Although nonpharmacological interventions are required in medical and nursing care professions [8], they pose a serious issue. Despite accumulating significant practical knowledge through experience, experienced professionals cannot effectively pass the knowledge on to newer and less experienced professionals due to heavy workloads that limit mentoring time and high turnover rates that hinder tacit knowledge transfer [7, 9].
Studies have attempted to structure empirical knowledge from qualitative data using various theoretical frameworks, including PCC [7, 10]. However, these studies are based on data extracted from small samples and are highly unique; they did not provide lists of universal good practice actions, as well. Further, educational interventions have been shown to cause positive changes in staff attitudes and improve care-practice quality [11, 12]. Therefore, there is a growing need to formalize successful care experiences into specific, observable practices that can be systematically identified and evaluated. Previous studies have shown that dementia related knowledge and attitudes among caregivers are important factors influencing the quality of care. For example, a large hospital-based survey found that staff with higher dementia knowledge and more positive attitudes were more prepared to implement person-centered dementia care [13].
Accordingly, the present study aimed to identify caregiver-reported good practices in dementia care. The specific objectives were: (1) to extract and organize good practices from free-text responses provided by healthcare professionals, and (2) to validate these practices through expert consensus.
Methods
This was a cross-sectional, text-mining-based study conducted among Japanese healthcare professionals recruited through an online research panel.
Participants
The study’s participants were Japanese healthcare professionals, particularly registered nurses, care workers, physical therapists, occupational therapists, speech‐language therapists, and care managers. All the participants were recruited by the medical monitor panel maintained by Macromill, Inc. (Tokyo, Japan). Eligible participants had prior experience providing health care or caregiving services to individuals with dementia. The following demographic characteristics were obtained: age, gender, “frequency of contact with people with dementia over the past month (almost every day, several times a week, once a week, less than once a week, none),” “Knowledge and understanding of dementia care (Know, Somewhat know, Neither know nor don't know, Don't know much, Don't know),” “Gathering information and studying about dementia care over the past month (doing, somewhat doing, neither doing nor not doing, not doing much, not doing).”
Scale to measure the awareness of person-centered dementia care
The Approaches to dementia questionnaire
Attitudes toward dementia care were measured using the Japanese version of Approaches to Dementia Questionnaire (ADQ) [14]. The ADQ includes 19 statements and uses a 5-point Likert scale (“1 = strongly disagree” to “5 = strongly agree”) to capture respondents’ attitudes toward people with dementia. A total score (range = 19–95) and two sub-scores, “hope” (range = 8–40) and “person-centeredness” (range = 11–55), are derived. Higher ADQ scores indicate more positive attitudes toward people with dementia. Finally, the Japanese version of ADQ has acceptable reliability and validity [15]. The ADQ demonstrated high internal consistency (Cronbach’s alpha [α] = 0.84), strong test–retest reliability (r = 0.89), and construct validity supported by factor analysis identifying two dimensions—Hope and Person-Centeredness—and convergent validity through significant correlations with dementia knowledge and care style measures.
Description and definition of good practice
Good practice is operationally defined as the specific actions recognized and enacted by caregivers that were found successful in improving the condition of people with dementia or that enabled them to perform actions appropriate to their goals. In this study, good practice items were collected from participants in a free-response format. In particular, questions were formulated for each of the six areas of daily living, that is, eating, elimination, getting up and moving around, personal hygiene, changing clothes and bathing, and communication, and participants were asked to describe specific practical actions constituting good practice. Furthermore, the definition of “state image” used to prompt responses was created based on the Well/Ill Being (WIB) value assessment stages of dementia care mapping [5] and provided as an example in the questionnaire. Therefore, the definition of good practice includes the following elements:
- Direct care interventions or environmental adaptations that elicited smiles or positive actions from care recipients.
- Direct care interventions or environmental adaptations that alleviated undesirable states—dissatisfaction or restlessness—in care recipients.
- Direct care interventions or environmental adaptations that drew out the care recipient’s abilities, thereby facilitating smoother care.
- Direct care interventions or environmental adaptations that drew out the care recipient’s abilities and enabled their use in daily living, rehabilitation, and recreational activities.
Analysis
Exclusion criteria
The study’s exclusion criteria were as follows: participants’ responses on any one of the knowledge, attitude, or ADQ scales had 90% or more identical answers; data were missing in demographic items or on any of the scales; the participants failed to respond seriously or left items blank; they provided non-substantive comments or verbatim reproductions of the example text in free-response fields; they submitted duplicate surveys; or their responses contained obvious typographical errors or omissions.
Descriptive statistics
Descriptive statistics were calculated for basic attributes; each questionnaire item, and the dementia attitude scale, knowledge scale, and ADQ total score. For the evaluation scales, the mean and standard deviation (± SD) values were calculated.
Qualitative analysis of free descriptions
Free description data were analyzed using KH Coder (Version 3) (https://khcoder.net/en/), a software that quantitatively analyzes text data and enables users to obtain the overall picture of the data, extract characteristic words, and visualize the relationships among words [16]. This software is widely used in international papers [17], and the authors have experience using it for data analysis [18].
Quantitative content analysis is a method in which open-ended data are quantified into numeric values by identifying specific keywords and patterns, and then analyzed using statistical techniques. The purpose is to clarify trends and relationships in the data using objective numerical evidence [16, 17]. We used this approach as an objective and reproducible method to avoid the effect of researchers’ subjective perceptions on results.
Identification of frequent keywords for good practice
The collected free-text data were converted to the Microsoft Excel format and analyzed using KH Coder to extract vocabulary, such as nouns, verbs, and adjectives, through morphological analysis. The top 50 most frequently occurring words were calculated for each of the six care scenarios and indicated as important keywords for good practice. However, words such as “eating,” which completely matched the situation, were removed from the list of extracted words to avoid hindering the analysis.
Structural characteristics of good practice items
Cooccurrence network and correspondence analyses were performed to list items. These methods involved a multivariate analysis on frequently used words in qualitative data and produced a cooccurrence network to ensure the connections among words in a cluster, which enabled us to search for the concepts and clusters included in the data [17, 18]. The Jaccard coefficient was used as an indicator of the association between words. This coefficient assumes a value between 0 and 1, and any value exceeding 0.2 indicates a strong association.
Correspondence analysis is a technique that visualizes relationships between extracted terms and other variables in a scatterplot. ADQ measures awareness and understanding of person-centered dementia care. Since dividing participants into high- and low-ADQ groups enables the extraction of words more strongly associated with effective good practices, in this study, participants were divided into high- and low-ADQ groups by a median split of their total ADQ scores, and correspondence analysis was conducted on the 20 most frequent terms to identify each group’s characteristics. In the resulting scatterplot, terms positioned close to the origin indicate the words common to both groups, whereas the terms located farther represent the words that were characteristic of one group or the other.
We used these analytical methods to visualize semantic connections based on the cooccurrence of words and identified the structural characteristics of good practice for each situation.
In the cooccurrence network diagram and correspondence analysis diagram, larger circles in the figures indicate higher frequency of occurrence.
Development of the good practice item list
We created a list of items by confirming the collected raw data to ensure that at least one item in each category had a Jaccard coefficient of 0.2 or higher in the cooccurrence network, constituting a good practice at the action level. Further, in the correspondence analysis, we extracted characteristic words from the high- and low-score groups; our focus was on the words that were characteristic of the high-ADQ score group. While confirming the raw data, we created a list of items for each word, referring to the words in the high-score group, to enable their use as good practice at the action level.
In other words, we reviewed the words with high scores in the correspondence analysis for each cooccurrence network category. Subsequently, we checked all the raw data of the extracted words written by participants and, based on the vocabulary and phrases that they considered practically useful, we created a list of good practice items for each situation. This process enabled us to expand the simple frequency analysis of words and analysis of structural characteristics to identify the specific actions underlying participants’ descriptions of “successful care experiences” and “tacit knowledge of dementia care.”
Validity verification of good practice items
The Delphi method was used to examine the validity of the good practice items extracted from the aforementioned free descriptions. The subjects were nurses and occupational therapists with master's or doctoral degrees who were involved in dementia care and were conducting research on dementia. Occupational therapists in Japan are recognized as specialists in both dementia care and activities of daily living (ADL); they were intentionally prioritized to evaluate the practical applicability of the good practice items. Delphi panelists were not drawn from the original participants. They were recruited separately through a snowball sampling approach.
They completed a questionnaire survey. For each good practice item, respondents had to select one of the following three options: “appropriate,” “neither appropriate nor inappropriate,” or “inappropriate.” Subsequently, the “content validity ratio” (CVR) was calculated for each item using the following formula [19]:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mathrm{CVR}=\left(\mathrm{Ne}-\mathrm{N}/2\right)/\left(\mathrm{N}/2\right)$$\end{document}where Ne is the number of evaluators who rated the item appropriate, and N is the total number of evaluators. The items with CVR values equal to or more than 0.75 were considered valid.
Ethical considerations
This study was conducted with the prior informed consent of participants, who were notified that participation was voluntary and data would be destroyed upon analysis completion. Ethical approval for the study was obtained from the Ethics Review Committee of the Graduate School of Rehabilitation Sciences, Osaka Metropolitan University, Japan (approval number: 2021–210) and conducted in accordance with the Helsinki Declaration and its later amendments. Clinical trial number: not applicable.
Results
Participant characteristics
Among the 897 survey respondents, 173 were excluded from the analysis based on the exclusion criteria. Accordingly, the analysis considered 724 valid cases. The sample comprised 225 men and 499 women, aged 20–68 years. The valid cases included 179 nurses, 188 care workers, 129 physical therapists, 135 occupational therapists, 50 speech language pathologists, and 43 care managers. The respondents’ mean professional experience was 12.8 years (SD = 8.3). Regarding facility type, 273, 65, 288, 65, and 33 participants worked in hospitals, clinics, care facilities, community-based settings, and other facilities, respectively. According to international classification standards, hospitals in this survey largely correspond to secondary and tertiary care, clinics represent primary care, and care facilities and community-based services represent long-term and community-based care, respectively. For contact frequency with people with dementia, 629 (86.9%) reported interacting almost daily or several times a week. Finally, regarding self-perceived dementia care knowledge, 524 (72.4%) reported that they “know” or “somewhat know” about dementia care. Tables 1 and 2 presents more participant characteristics.Table 1. Sociodemographic characteristics of participantsValueAge (years), mean ± SD41.3 ± 10.4Sex, n (%)Male 225 (31.1), Female 499 (68.9)Work experience (years), mean ± SD12.8 ± 8.3Table 2Professional characteristics of participantsN%OccupationPhysical therapists12917.8Occupational therapists13518.6Speech therapists506.9Care managers435.9Nurses17924.7Care workers18826.0Workplace facilityHospitals (secondary/tertiary care)27337.7Workplace facility: Clinics (primary care)659.0Nursing care facilities28839.8Community-based offices659.0Other334.6Frequency of contact for the past monthAlmost every day48767.3Several times a week14219.6Once a week142.2Less than once a week315.0No contact508.0Knowledge of dementia careKnow14219.7Somewhat know38247.2Neither know nor don’t know13421.5Don’t know much518.1Don’t know152.4Gathering information about dementia over the past monthDoing12319.7Somewhat doing29547.2Neither doing nor not doing17327.7Not doing much9415.1: Not doing396.3ADQ (Approach to Dementia Questionnaire), range 19–95, mean ± SD68.37.9Values are presented as n (%) unless otherwise indicatedPT, physical therapist; OT, occupational therapist; ST, speech therapist; CM, care manager; Nurs., nurse; CW, care worker; ADQ, Approach to Dementia Questionnaire
Scale measuring awareness of person-centered dementia care
The participants’ mean total score on the Japanese version of the ADQ was 68.30 ± 7.88.
Listing good practice items
Frequently used words
Based on the free-text data collected from 724 healthcare and nursing professionals, the top 50 frequently used words were assessed for each of the six care scenarios by KH coders. Table 3 depicts the results.Table 3. Top 50 frequently used words in each care situationEatingBed mobility and transferHygieneToiletingBathing and dressingCommunicationExtracted wordsNumber of occurrencesExtracted wordsNumber of occurrencesExtracted wordsNumber of occurrencesExtracted wordsNumber of occurrencesExtracted wordsNumber of occurrencesExtracted wordsNumber of occurrencesAssistance252Voice284Perform283Perform209Perform200Smile248Eating182Perform241Voice194Voice205Voice166Talk140Matching117Assist184Assistance104Assistance164Assistance165Voice127Voice115Action145Person90Toilet143Self87Conversation126Pace71Explain108Action87Confirm87Can78Match98Smile71Communicate79Self85Consider72Confirm72Eye contact76Performing66Individual69Explanation55Explain61Explain68Negative70Individual62Consent65Mirror54Individual58Wash64Other person69Eye contact58Adjust61Can53Shyness58Person61Conversation67Confirm53Obtain61Before49Movement57Action51Talking65Environment53Confirm55Care46Guide49Change clothes48Person59Negative53Always48Confirm40Same sex48Consider39Interact52Talk52Now42Washroom38Privacy46Part39Listen52Partner50Partner42Oral34Change42Communicate34Words50Conversation50Words36Self34Communicate42Pace32Topic49Communicate49Pace35Obtain34Go39Self32Listening attentively39Swallowing45Self35Communicate33Obtain38Temperature30Do39Listen42Before32Consent28Always38Mind30Eyes39Explain40Possible31Always28Intention35Situation28Be mindful34Talk40Understand30Smile27Consent33Clothes27Fun33Look38Pain29Go26Self32Match26Look33Respond36Move28Match26Case30Involve25Respond30Menu35Smile27Encourage25Diaper28Always24Person26Mouth35One by one24Involve24Possible28Assist23Kind26Concentration33Go24Now23Time26Shyness23Interest23Food33Instruct22Especially23Person24Caution22Atmosphere22Words30Talk22Pace22Before24Case20Family21Self30Action21Look22Mind23Response20Mind20Attention30Timing20Show21Respond23Same sex20Use20Sitting29Hand20Brushing teeth20Say22Privacy19Expression20Use29careful20Gentle20Diaper21Go19Say18Posture26Encourage20Situation19Polite20Before19Like18Time26Move20Watch18Involve18Obtain19Past17Hold25Understand20Talk18Adjust18Especially18Big17Encourage25Unnecessary20When17Curtain17Hot water17Understand17Patient24Use20Person17Urination17Wash17Awareness16Case24Talk20Time16Utilization17Watch over16Interact16Possible23Respond19Implement16Talk17Condition16Polite16Interact23Anxiety19Wash16Pants16Body16Communicate16Spoon22Guide19Necessary16Be mindful16Skin16Tone15Form22Mind17Part16Especially16Bath15Utilization15Mistake22Implement17Partner15Necessary16Intervene15Empathy14Person22Fall17Together14Refuse15Perform15Target14Intake22Ability17Use14Smile15Partner15Understand14Involved21Listen17Usage14Close15Encourage15Interact13Situation21Strength17Understand14One by one14Dressing/undressing15High13Tableware21Wheelchair16Words13Words14Falls15Create13Serving21Move15Life13Situation14Necessary15Eye contact13Swallowing21Get up15Understand13Bowel movement14Patient14Peace of mind12Careful20Always15Utilization13Gentle14Environment14Bring out12Front20Movement15Observation14Feelings12Eyes20Washable14Time12Wear14Always12Careful14Respect12Listen14Weather12Utilization14Being sure12
In the eating situation, frequently used words such as “match,” “voice,” “pace,” and “smile” were extracted. Similarly, in the “mobility and transfer” situation, “voice,” “action,” “explanation,” and “consent” were extracted as frequently occurring terms, whereas, in the “personal care” situation, “voice,” “the individual,” “action,” “self,” and “explanation” were extracted. In the “elimination” situation, “voice,” “confirmation,” “consideration,” “explanation,” and “shame” were extracted as frequently occurring terms. Further, in bathing and dressing situations, frequently occurring words such as “voice,” “self,” “can,” “confirmation,” and “explanation” were extracted. Finally, in communication situations, frequently occurring words such as “smile,” “voice,” “match,” “eye contact,” and “denial” were extracted.
Results and the interpretation of cooccurrence networks
The visualization of the cooccurrence network structure revealed multiple common words (“smile,” “eye contact,” “wait,” “obtain consent,” etc.) in all situations. For each category with a Jaccard coefficient of 0.2 or higher in the cooccurrence network, we created a list of items that could be practiced by caregivers at the action level and selected one or two items to confirm the raw data (Fig 1).Fig. 1. Cooccurrence network diagram for each care situation. The larger circles in the figure indicate that the words appear frequently
Eating situation
In the eating situation, the cooccurrence network was divided into six clusters, including “explanation” and “menu.” Phrases such as “explaining the contents of the meal (menu)” were interpreted and extracted from raw data and categorized as good practice items; these are listed in Table 3.
Bed mobility and transfer situation
In this situation, the cooccurrence network was divided into four clusters, including “pace” and “match.” Phrases such as “match the pace” were interpreted as good practice items; they are listed in Table 3.
Hygiene situation
In the hygiene situation, the cooccurrence network was divided into six clusters, including “eye contact” and “made (eye contact).” Phrases such as “made eye contact” were interpreted as good practice items (Table 3).
Toileting situation
In the toileting situation, the cooccurrence network was divided into seven clusters, including “intention” and “confirmation.” Phrases such as “confirming the intention to use the toilet” were interpreted as good practice items (Table 3).
Bathing and dressing situation
In this situation, the cooccurrence network was divided into eight clusters, including “confirming,” “temperature,” and “hot water.” Phrases such as “checking the temperature of the hot water” were interpreted as good practice items (Table 3).
Communication situation
In the communication situation, the cooccurrence network was divided into five clusters, including “enjoyable,” “atmosphere,” and “create.” Phrases such as “creating an enjoyable atmosphere” were interpreted as good practice items (Table 3).
Correspondence analysis results and their interpretation
As part of correspondence analysis, data were divided into two groups—high- and low-ADQ score groups—and characteristic words were extracted from the high‐score group. After confirming the words identified in the high-score group against the original raw data, we created a list of items that can be implemented by caregivers as good practice actions (fig 2).Fig. 2. Correspondence analysis diagram for each care situation. Participants were divided into two groups based on the median Approaches to Dementia Questionnaire score (group 1: low scores; group 2: high scores), and the top 20 most frequent words were extracted. Subsequently, a correspondence analysis scatterplot was generated to identify the good practice (GP) items characteristic of the high-ADQ score group. The larger circles in the figure indicate that the words appear frequently. The X-axis (Dimension 1) and Y-axis (Dimension 2) indicate relative “distance,” with words in the positive direction being characteristic of the High-ADQ group and those in the negative direction being characteristic of the Low-ADQ group
Eating situation
For the high-ADQ score group, words such as “preference,” “understanding,” “concentration,” and “environment” were extracted. Based on these words, good practice items such as “understanding food preferences” and “creating an environment conducive to concentration” were identified (Table 3).
Bed mobility and transfer situation
Words such as “explanation” and “ability” were extracted. Based on these words, good practice items such as “explained each assistive action” and “utilized remaining abilities” were identified.
Hygiene situation
Words such as “communicate” and “understand” were extracted. Based on these words, good practice items such as “communicated that they were clean” and “communicated the purpose of hygiene and obtained consent” were identified.
Toileting situation
Words such as “one by one” and “intention” were extracted. Based on these words, good practice items such as “explained each assistance action” and “confirmed the intention to defecate” were identified.
Bathing and dressing situation
Words such as “refusal” and “safety” were extracted. Based on these words, good practice items such as “did not force the patient if they refused” and “set up a safe environment (handrails, seat arrangement, etc.)” were identified.
Communication situation
Words such as “understanding,” “exchanging,” and “denying” were extracted. Based on these words, good practice items such as “used gestures (body language) while talking” and “did not deny the content of the conversation.” In summary, this analysis extracted a total of 79 good practice items, with items such as “making eye contact” included in communication situations (Table 4).Table 4CVR values for each care situationEatingBed mobility and transferHygieneToiletingBathing and clothingCommunicationItem noItemCVRItemCVRItemCVRItemCVRItemCVRItemCVR1Confirmed swallowing before bringing the next item to the mouth0.875Matched pace (matched the other person's movements)0.875Made eye contact0.625Closed curtains and doors to ensure privacy0.875Checked water temperature0.875Created a fun-filled atmosphere12Made eye contact0.75Communicated the transfer’s purpose and obtained consent1Matched the pace (adjusted to the person's movements)0.875Guided the individual to the toilet0.875Adjusted the pace (to match the movements of the person being assisted)0.75Listened attentively13Matched the pace (adjusted to the person's movements)0.875Made eye contact0.875Shaving, brushing teeth, and taking care of hygiene were performed in front of the sink or using a mirror provided0.875Confirmed the individual's intention to use the toilet0.875Closed curtains and doors to ensure privacy0.875Made eye contact14Created an environment conducive to concentration0.875Listened attentively0.875Explained the purpose of hygiene and obtained consent0.875Explained the purpose of using the toilet and obtained consent0.625Observed the skin’s condition0.875Asked about topics of interest, hobbies, and life experiences15Sat down next to the person0.625Approached the person with a smile1If the person resisted, did not force them, gave them time, or took extra time0.875Interacted with a smile0.75Explained the purpose of bathing and changing clothes and obtained consent0.875Communicated in short, easy-to-understand words16Sat down facing the person0Checked for pain (facial expressions)1Approached the person with a smile0.875Encouraged cooperation where possible (utilized remaining abilities)0.875Explained each step of the assistance process0.875Interacted with a smile17Explained the meal menu0.75Cooperated with the other person as much as possible (utilized remaining abilities)1Asked for cooperation where possible (utilized remaining abilities)0.875Adjusted pace to match the individual's movements0.875Established a safe environment (handrails, seating arrangements, etc.)0.875Talked about family (life experiences)0.758Understood the person's food preferences0.875Used gestures to help the other person understand the transfer movements1Explained each assistive action0.75Conducted the procedure in an environment conducive to the individual's needs (e.g., handrail placement)0.875Interacted with a smile0.875Used gestures (body language) while talking19Did not negate the content of the conversation0.875Confirmed the position of the other person's arms and legs1Praised them for looking clean0.875Took care to dress and undress gently0.875Received assistance from someone of the same gender0.875Called the person by name110Interacted with a smile0.875Performed the transfer in a way that minimized strain0.75Used tools familiar to the individual in their daily life (e.g., razor, comb)0.875Reassured the individual not to worry about incontinence0.25Encouraged cooperation for the tasks the person could perform (utilizing remaining abilities)0.875Greeted the person111Used the same utensils the person used at home0.75Explained each assistance action0.75Used gestures to help the individual understand hygiene actions0.875If there was refusal, did not force the individual (did not perform the procedure against their will)0.875Started with individuals without paralysis (or with mild paralysis) for undressing (when dressing, started with those with paralysis) (not applicable for dementia patients)−0.875Did not negate the content of the conversation112Used utensils that were easy to hold and eat with0.875Responded with a same-sex caregiver0.875Avoided forcing assistance if refused (did not perform procedures against the individual's will)0.875Nodded; spoke loudly, slowly, and clearly113Adjusted the form of the meal0.875Explained each assistive action step by step0.75Spoke in a way that made my facial expressions clear to the other person114Adjusted the person's posture to a comfortable one for eating0.875Spoke face to face0.62515Assisted the individual to see the food0.87516Engaged in conversation related to the meal (other than explaining the menu)0.87517Adjusted the portion size0.87518Communicated that the meal was delicious0.75CVR Content validity ratio
Validity verification results for good practice items using the Delphi method
Sixteen experts (15 occupational therapists and 1 nurse) participated in the validity assessment of each good practice item. Subsequently, 72 of 79 items met the CVR criterion of 0.75 or higher, and at least 13 participants evaluated them as valid. The remaining seven items did not meet the CVR criterion (Table 4).
The items that did not meet CVR criteria included specific opinions such as “The seating position during eating varies depending on the situation; so, it cannot be generalized,” which were considered practical and relevant to the clinical setting. Items that did not meet the CVR threshold were reviewed by the authors against the Delphi panelists’ stated reasons for exclusion and were removed from the final good practice list. No new items were added during this process.
Discussion
In this study, 72 items of practical knowledge were extracted as good practice from 724 medical and care professionals involved in dementia care in six care situations. These findings have important implications in establishing a foundation for educational interventions aimed at improving dementia care quality. In existing dementia care education programs such as Humanitude, techniques like “seeing” and “touching” are emphasized as essential components of care [20]. Previous research has highlighted the importance of addressing residents by name and using positive language in communication training for nursing staff [21]. These approaches are important and overlap with several of the good practice items identified in our study. However, most existing programs focus on general communication techniques with people with dementia, whereas the present study uniquely organizes good practices by specific ADL situations, thereby providing a structured framework that can be more directly translated into everyday care practices and training modules. This situational organization may enhance applicability in clinical training because it allows staff to practice context-specific behaviors that are immediately relevant to daily caregiving tasks.
Our good practice items can be organized by ADL situation to develop training modules. These modules can form the basis of hands-on workshops and simulation exercises that allow health professionals to practice these actions and receive targeted feedback. By embedding these items into competency checklists, institutions can measure proficiency, identify gaps, and tailor future training. Future studies should assess whether such focused training reduces the behavioral and psychological symptoms of dementia, decreases staff burnout, and improves self-efficacy.
Characteristics of participants in this study
The participants had frequent contact with people with dementia as part of their daily work and scored high on measures of PCC awareness. In this study, the mean ADQ score was 68.3 (SD = 7.9). A cross-sectional study in 15 Dutch nursing homes reported ADQ scores among healthcare professionals ranging from 65.7 to 74.2 [22]. Our participants achieved comparable scores. These participants’ characteristics support the reliability of the survey’s free-response data, as they reflect the practical knowledge of experienced, specialized professionals working in the clinical practice.
Practical knowledge in dementia care
Dementia care settings are characterized by busy daily routines and high staff turnover, which makes it difficult for experienced staff to pass on their practical knowledge to newer staff [23]. This study indicates that structuring tacit knowledge through cooccurrence network analysis and linking it to PCC through correspondence analysis has several implications. It reveals the meaningful connections underlying high-quality practice and clarifies how the dementia care process can be translated into concrete, actionable steps. In addition, presenting these practices as a structured list makes them easier to transfer to newly recruited staff, thereby facilitating continuity of good dementia care even in settings with frequent turnover.
When listing good practice items, the items extracted in this study, smile, eye contact, and “obtaining consent,” are commonly used in any situation, and these words may be the core elements of each daily living situation, such as eating, toileting, and bathing. This may indicate that the PCC philosophy is a crucial part of the practical knowledge of healthcare and nursing staff. In particular, the fact that a list of specific actions related to the consideration for individuality and respect for autonomy, such as “understanding meal preferences” and “not forcing refusal,” was extracted from the high-ADQ score group suggests that the PCC philosophy comprises not only theoretical knowledge but also actions.
Research on PCC clarifies that the generalizability of specific care behaviors is a challenge [24]. In this study, we used text mining, a quantitative method, to extract practical knowledge, or the experiences that were considered successful by medical and nursing care professionals, and identified specific actions based on PCC principles. This approach plays an important role in linking abstract concepts to concrete practices and is consistent with earlier studies on ADL support that lead to “peace of mind” and “maintaining autonomy” [3]. It is well established that agitation often occurs during bathing or excretion [25]. The good practice list of each ADL situation can provide guidance for future educational interventions as practical nonpharmacological care for behavioral and psychological symptoms of dementia [8].
Validity of good practice items and list refinement using the Delphi method
Expert evaluation using the Delphi method confirmed the high practicality and reliability of the extracted good practice items. The impractical items that did not meet CVR criteria were removed from the list. Therefore, this good practice list is consistent with expert opinion and has been established as a highly refined list. In addition, we clarified the basis for applying the CVR threshold. The cutoff was set at ≥ 0.75 in accordance with Lawshe’s method [19]. Notably, a recent study used a lower cutoff (≥ 0.56) with 12 experts in developing a dementia-related scale [26], whereas our study adopted the stricter criterion of ≥ 0.75 with a larger expert panel (n = 16). This comparison further supports the robustness and validity of the finalized good practice item list.
Limitations of and future challenges posed by this study
This study has several limitations. First, since free-response data are based on respondents’ subjective opinions, they may not cover all good practice aspects. Additionally, the validity assessment using the Delphi method was conducted by a limited number of experts and did not incorporate the opinions of family caregivers and persons with dementia. Moreover, most Delphi participants were occupational therapists, which underrepresented the perspectives of other healthcare professionals, such as nurses and physiotherapists. Occupational therapists are specialists in dementia care and ADL and, therefore, highly qualified to evaluate practical aspects of good practice items. These aspects may affect the generalizability of the findings. Hence, future research must incorporate intervention studies to verify the effectiveness of good practice item lists as educational programs.
Future developments and practical applications
Educational interventions effectively change staff attitudes and increase self-efficacy, thereby improving the quality of care practices [12]. The good practice item list obtained in this study is expected to serve as effective specific content for such educational interventions. In particular, the items can be organized by ADL situations—such as eating, toileting, and bathing—to create structured training modules. This organization can be practiced through simulation exercises. This approach is consistent with prior work that highlights respect, structured processes, and supportive environments as common themes across ADL domains [27]. Moreover, intervention studies, including communication-focused training that emphasizes brief instructions and positive language, have improved staff–resident interactions and reduced caregiver distress, supporting the applicability of our good practice items as structured training content [21].
For example, it provides practical guidance on specific content for “speaking to patients” in various situations and postures when making eye contact. Moreover, care training is reported to cause behavioral changes in healthcare professionals [28], and the good practice list can serve as specific content for similar educational interventions.
Conclusions
This text-mining study of caregiver-reported “good practices” identified practice elements that were associated with more favorable care-recipient conditions in dementia care. These findings highlight the importance of systematically identifying effective care practices and incorporating them into staff training and individualized care planning.