Assessing arterial stiffness using characteristics of Korotkoff sounds
Shuqi Ren, Wei Zhao, Changcheng Yi, Xiaoyan Deng, Zengsheng Chen, Li Wang, Ling Xu, Yuheng Yang, Yubo Fan, Anqiang Sun

TL;DR
This study explores using Korotkoff sounds during blood pressure measurements to assess arterial stiffness, a marker of vascular aging, through machine learning techniques.
Contribution
The novel use of Korotkoff sound features and machine learning to infer arterial stiffness and age-related vascular differences is presented.
Findings
Features like center of mass and peak frequency from Korotkoff sounds showed significant differences between age groups.
Deep learning models achieved high classification accuracy (up to 93.7%) for age-related vascular differences.
Korotkoff sound features had a modest association with brachial-ankle pulse wave velocity (baPWV).
Abstract
Arterial stiffness is a recognized marker of vascular ageing and is associated with adverse cardiovascular outcomes. However, routine assessment of pulse wave velocity (PWV) remains limited in many clinical and home settings. This study investigated the feasibility of extracting arterial stiffness-related information from Korotkoff sounds recorded during cuff-based blood pressure measurement using feature analysis and machine learning. Korotkoff sounds were collected from 123 young (25.9 ± 2.2 years) participants and 112 older (67.5 ± 6.7 years) participants using a custom-developed device as a proof-of-concept for age-related vascular differences. In addition, 81 hospital participants with measured brachial-ankle PWV (baPWV) were enrolled and grouped according to baPWV to further evaluate clinical feasibility. Time- and frequency-domain features were extracted, and both traditional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
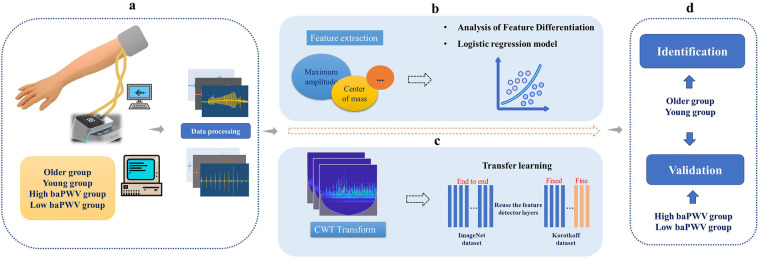 Figure 1
Figure 1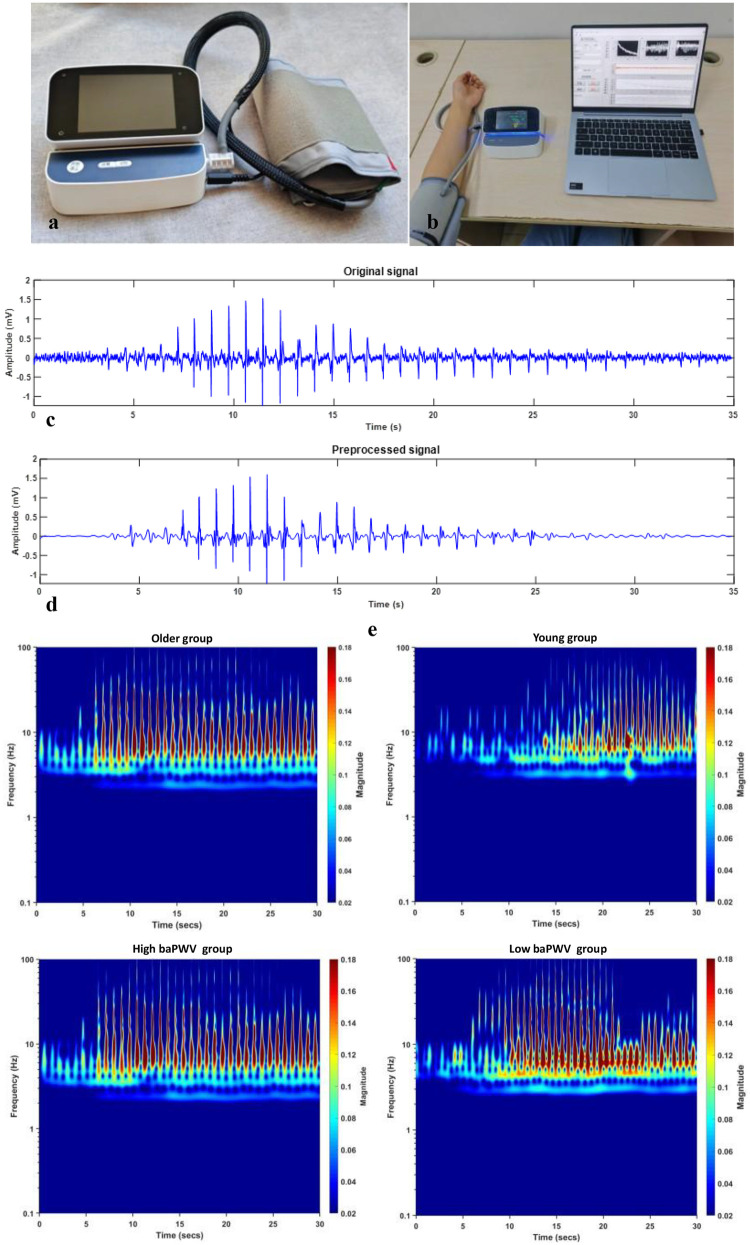 Figure 2
Figure 2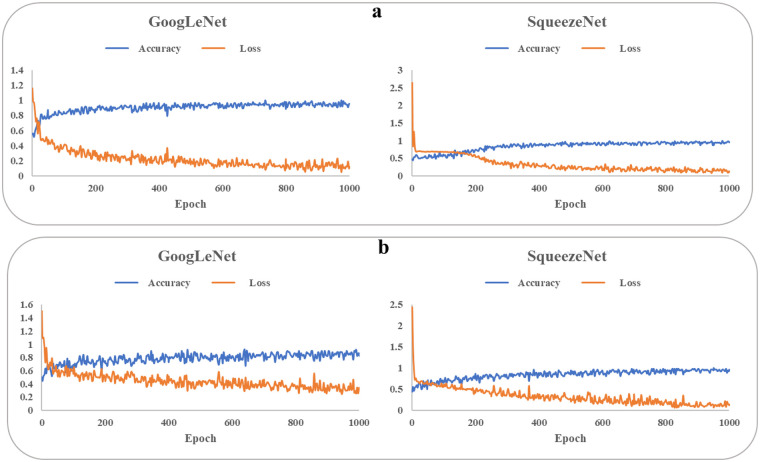 Figure 3
Figure 3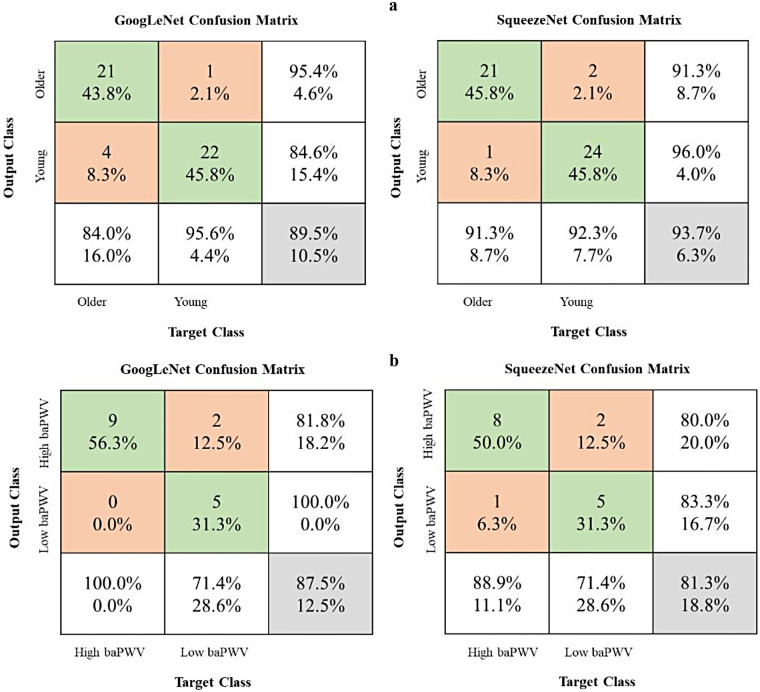 Figure 4
Figure 4| Variables | Older ( | Young ( |
|
|---|---|---|---|
| Age in years, M (SD) | 67.5 (6.7) | 25.9 (2.2) | <0.001 |
| Gender, | 0.112 | ||
| Male | 44 (39.4) | 57 (46.3) | |
| Female | 68 (60.7) | 66 (53.7) | |
| BMI, M(SD) | 23.4 (1.5) | 22.8 (1.1) | 0.115 |
| Blood pressure, M(SD) | |||
| SBP | 120 (11) | 118 (6) | 0.083 |
| DBP | 79 (6) | 77 (5) | 0.091 |
| Heart rate, M (SD) | 78.2 (11.4) | 76.0 (9.2) | 0.129 |
| Variables | High baPWV ( | Low baPWV ( |
|---|---|---|
| Age in years, M (SD) | 51.8 (14.2) | 36.7 (9.7) |
| Gender, | ||
| Male | 25 (55.6) | 11 (30.6) |
| Female | 20 (44.4) | 25 (69.4) |
| BMI, M(SD) | 26.0 (4.1) | 23.0 (3.4) |
| Blood pressure, M(SD) | ||
| SBP | 136 (13) | 118 (12) |
| DBP | 81 (9) | 69 (11) |
| Heart rate, M (SD) | 74.2 (10.6) | 72.0 (11.5) |
| Diabetes, | 8 (17.8) | 7 (19.4) |
| Smoking, | 8 (17.8) | 3 (8.3) |
| Past medical history, | 27 (60.0) | 7 (19.4) |
| Indicates | Young | Older |
| T | Cohen's d |
|---|---|---|---|---|---|
| Maximum amplitude | 1.095 (0.446) | 1.059 (0.555) | 0.679 | 0.414 | 0.072 |
| Kurtosis | 14.199 (5.364) | 17.094 (4.202) | 0.070 | −1.828 | −0.316 |
| Skewness | 0.231 (0.689) | −0.802 (1.371) | <0.001 | 5.632 | 0.973 |
| Peak factor | 6.941 (1.504) | 6.526 (2.421) | 0.228 | 1.211 | 0.209 |
| Pulse factor | 12.860 (3.511) | 12.978 (6.127) | 0.298 | 1.045 | 0.181 |
| Form factor | 1.726 (0.238) | 1.777 (0.305) | 0.279 | −1.087 | −0.188 |
| Center of mass | 0.971 (1.605) | −0.643 (1.574) | <0.001 | 5.785 | 0.999 |
| Peak frequency | 3.707 (1.478) | 2.653 (0.441) | <0.001 | 5.411 | 0.935 |
| Center of gravity frequency | 28.330 (5.798) | 32.417 (13.206) | 0.018 | −2.388 | −0.412 |
| Mean square frequency | 7.771 (1.596) | 9.514 (5.595) | 0.017 | −2.427 | −0.419 |
| Features | Coef. | SE | Wald |
| OR | 95% CI |
|---|---|---|---|---|---|---|
| Maximum amplitude | 1.399 | 0.648 | 4.663 | 0.031 | 4.050 | [1.138,14.412] |
| Kurtosis | 0.050 | 0.097 | 0.264 | 0.608 | 1.051 | [0.869,1.272] |
| Skewness | −1.543 | 0.521 | 8.768 | 0.003 | 0.214 | [0.077,0.594] |
| Peak factor | 1.051 | 0.632 | 2.768 | 0.096 | 2.861 | [0.829,9.873] |
| Pulse factor | −0.528 | 0.294 | 3.212 | 0.073 | 0.590 | [0.331,1.051] |
| Form factor | 0.333 | 1.578 | 0.044 | 0.833 | 1.395 | [0.063,30.735] |
| Center of mass | −0.879 | 0.237 | 13.768 | <0.001 | 0.415 | [0.261,0.660] |
| Peak frequency | −1.516 | 0.495 | 9.372 | 0.002 | 0.220 | [0.083,0.580] |
| Center of gravity frequency | −0.041 | 0.048 | 0.707 | 0.400 | 0.960 | [0.874,1.055] |
| Mean square frequency | 0.135 | 0.201 | 0.455 | 0.500 | 1.145 | [0.773,1.697] |
| Hosmer-Lemeshow test | χ² |
| ||||
| 6.601 | 0.580 | |||||
| Accuracy | 83.7% | |||||
| Indicates |
| r | 1- |
|---|---|---|---|
| Maximum amplitude | 0.049 | 0.218 | 0.228 |
| Kurtosis | 0.182 | 0.103 | 0.205 |
| Skewness | 0.031 | 0.181 | 0.233 |
| Peak factor | 0.745 | 0.037 | 0.056 |
| Pulse factor | 0.442 | −0.087 | 0.084 |
| Form factor | 0.048 | −0.240 | 0.326 |
| Center of mass | 0.005 | −0.310 | 0.506 |
| Peak frequency | 0.011 | −0.254 | 0.360 |
| Center of gravity frequency | 0.195 | 0.146 | 0.148 |
| Mean square frequency | 0.847 | −0.022 | 0.052 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Health and Disease Prevention · Non-Invasive Vital Sign Monitoring · Phonocardiography and Auscultation Techniques
Introduction
As the ageing population increases globally, the prevention of cardiovascular disease (CVD) faces more severe challenges (1). By 2030, about 20% of the population will be aged 65 years or older, and in this age group, CVD will be the leading cause of death, accounting for 40% of deaths (2). Arterial stiffening is a key manifestation of vascular ageing and is associated with higher cardiovascular morbidity and mortality (3–9). Accordingly, assessment of arterial stiffness has attracted growing interest as a means to characterize vascular health and potentially refine prevention strategies (10–12).
Pulse wave velocity (PWV) is widely used for non-invasive assessment of arterial stiffness (13–16). Importantly, carotid-femoral PWV (cfPWV), which reflects aortic (large elastic artery) stiffness, is regarded as the reference-standard measure for arterial stiffness assessment in clinical practice and research, and standardization of its measurement has been emphasized in expert consensus documents (17). However, cfPWV measurement often requires dedicated equipment and trained operators, which limits access in routine primary care and home settings. Recent hypertension guidelines underscore the need for pragmatic approaches that can be implemented broadly across care settings (18).
In contrast to dedicated PWV devices, Korotkoff sounds are already routinely generated during cuff-based blood pressure measurement. Although their precise genesis remains debated, both arterial wall mechanics (compliance-related vibration) (19, 20) and hemodynamic factors (flow patterns) (21–23) are believed to contribute, suggesting that Korotkoff sounds may contain information related to vascular properties. Evidence in recent years (24–26) has increasingly supported the concept that Korotkoff sounds encode physiologically meaningful signatures beyond systolic/diastolic pressure, motivating efforts to extract vascular information from these signals.
Korotkoff sounds are complex, non-stationary biosignals, posing analytical challenges similar to heart sounds and other physiological waveforms. Conventional approaches typically rely on engineered time- and frequency-domain features, whereas deep learning can learn high-dimensional representations directly from time–frequency maps. Transfer learning with convolutional neural networks (CNNs) has proven effective in biosignal classification when domain-specific labeled datasets are limited (27–30).
In this study, we investigated whether machine-learning analysis of Korotkoff sounds can capture stiffness-related information. We performed (i) a proof-of-concept analysis comparing young and older adults (age-defined groups expected to differ in vascular ageing), and (ii) an additional clinical feasibility analysis in a separate cohort with measured PWV, to examine whether Korotkoff sound–derived features and models relate to PWV. Because age itself (and estimated PWV derived from age and blood pressure) can be used for risk estimation, the present work focuses on feasibility rather than establishing incremental prognostic value beyond conventional variables (31).
Methods
The overall methodology of this study is outlined in Figure 1. In brief, Korotkoff sound signals were acquired from participants using a self-developed device. Participants were categorized for two complementary analyses: (i) an age-stratified proof-of-concept comparison between an older group and a young group (age used as a surrogate of vascular ageing rather than a direct stiffness diagnosis), and (ii) in a separate clinical feasibility cohort with measured brachial-ankle pulse wave velocity (baPWV), a comparison between high-baPWV and low-baPWV groups based on measured baPWV values. Furthermore, the correlation between baPWV and the acoustic features was investigated to explore clinical relevance of the proposed method.
Schematic diagram of the study methodology. baPWV, brachial-ankle pulse wave velocity. CWT, continuous wavelet transforms. (a) Data Acquisition and Preprocessing: Korotkoff sound signals were collected and preprocessed. Participants were stratified into older group vs. young group (age-stratified), and into high-baPWV group vs. low-baPWV group. (b) Traditional Feature Analysis: Time- and frequency-domain features were extracted from the signals and compared between the older group and young group to identify significant differences. A logistic regression model was subsequently developed for classification. (c) Deep Learning-Based Classification: Time-frequency images were generated via CWT, and convolutional neural networks were trained using a transfer learning approach. (d) Clinical Feasibility: The Korotkoff sound–based approach was further evaluated against measured baPWV data.
Hardware device
Signal acquisition was performed using a custom-developed Korotkoff sound acquisition device (Figure 2A), which comprised three primary components: a hardware unit, an inflatable cuff, and a sensor integrated into the cuff for Korotkoff sound detection. The hardware unit contained a pump for cuff inflation and deflation, an STM32H750 microprocessor with 24-bit AD sampling for data acquisition and system control, and a Bluetooth module for communication with a computer. To balance performance and cost, a CM-01B sensor was utilized for collecting Korotkoff sound signals (32), while an MPS20N0040D-S sensor was employed to acquire the cuff pressure signal. All Korotkoff sound signals were sampled at a frequency of 1,000 Hz.
baPWV, brachial-ankle pulse wave velocity. (a) The self-developed Korotkoff sound signal acquisition device. (b) The process of collecting signals. (c) The original Korotkoff sound signal. (d) The preprocessed Korotkoff sound signal. (e) The time-frequency RGB images after continuous wavelet transform (older group vs. young group, high-baPWV group vs. low-baPWV group).
In the clinical feasibility cohort, baPWV was measured as the comparator PWV index using an automatic waveform analyzer (BP-203 RPE III, Omron Health Medical, Dalian, China). baPWV was used as the comparator PWV measure because it is widely implemented in clinical workflows and population studies and can be obtained with high operational efficiency (33–36).
Data acquisition
Arterial structure and function change with age, resulting in progressive arterial stiffness (13). This well-established relationship, demonstrated by Gomez-Sanchez et al. in a Spanish adult cohort without overt CVD (10), provided the rationale for using age as a primary grouping variable in the proof-of-concept analysis. An a priori power analysis was conducted to ensure sufficient statistical power, defined as an 80% probability of detecting a true effect at a significance level (α) of 0.05. Based on a reference effect size from a similar study (26), the total required sample size was estimated to be 200. Therefore, we collected Korotkoff sound signals from 112 older adults (67.5 ± 6.7 years) and 123 young adults (25.9 ± 2.2 years), as the older and young groups, respectively. To evaluate clinical feasibility using a measured arterial stiffness index, Korotkoff sound and concurrent baPWV data were additionally collected from 81 hospital participants. Based on the median baPWV value of this cohort, participants were stratified into two groups (high baPWV vs. low baPWV) for PWV-defined classification and association analyses.
Participants for the primary comparison (older vs. young groups) were recruited from the community. Korotkoff sound recordings were obtained with the participant seated and the test arm supported such that the cuff on the mid-upper arm was positioned at heart level. The cuff was applied directly on the bare upper arm (participants removed thick clothing from the measurement arm) to minimize signal attenuation and artifacts. The sensor was positioned over the brachial artery pulse point. Following cuff inflation to achieve complete arterial occlusion, signals were acquired during a controlled deflation period. All participants provided written informed consent and completed a questionnaire covering demographics (age, sex, height, weight), medication use, medical history, and smoking status. Blood pressure and heart rate were obtained during the study visit using standardized measurements performed by trained staff and were recorded alongside the Korotkoff sound acquisition. The inclusion criteria for the young and older groups were: age 20–30 or 60–79 years, respectively; a body mass index (BMI) of 20–25 kg/m²; good general health without a history of major diseases; non-smoking status; and normal blood pressure and heart rate. Representative Korotkoff sound recordings from older and young subjects are provided in the Supplementary Material Audio.
The data for the high-baPWV and low-baPWV groups were collected at a hospital. All the participants provided informed consent and completed a detailed questionnaire (as described above). Subjects aged 20–79 years with no serious diseases (including cardiovascular diseases, malignant tumors, severe primary liver or kidney diseases, or chronic lung diseases) were included. Participant characteristics are summarized in Table 1 (age-stratified cohort) and Table 2 (baPWV-measured hospital cohort).
Signal processing and feature extraction
All data processing was performed using MATLAB (version 2019a). The acquired Korotkoff sound signals were first processed to eliminate baseline drift using filtering techniques. Subsequently, high-frequency noise was attenuated employing wavelet transform, which offers superior time-frequency localization for non-stationary signals. Figures 2c,d display representative original and preprocessed Korotkoff sound signals, respectively.
For the preprocessed signals, we introduced the concept of “center of mass” to integrate amplitude and temporal location information. A set of six time-domain features was extracted, including maximum amplitude, kurtosis, skewness, peak factor, pulse factor, and form factor. Additionally, three frequency-domain features were obtained: peak frequency, center of gravity frequency, and mean square frequency. Detailed mathematical descriptions of the preprocessing steps and feature extraction formulas are provided in the Supplementary Material.
Statistical analysis
All statistical analyses were performed using SPSS (version 27, IBM Corp.). Normality of continuous variables was assessed using the Kolmogorov–Smirnov test. For comparisons of acoustic features between groups, independent-samples t-tests were used to compare mean values. Homogeneity of variance was evaluated using Levene's test; when variances were unequal, Welch's t-test was applied. To account for multiple comparisons across the ten extracted features, statistical significance for the univariate feature comparisons was set at p < 0.005 (Bonferroni correction).
To address potential confounding factors in the correlation analyses between Korotkoff sound features and arterial stiffness (as measured by baPWV), multivariable linear regression analyses were conducted. Candidate covariates for adjustment were pre-specified based on prior literature and clinical plausibility, and their distributions and intercorrelations were also examined in the current dataset. Age, diabetes, obesity (BMI) and systolic blood pressure (SBP) were included as established determinants of baPWV (37–40). Separate regression models were built for each Korotkoff sound feature that demonstrated a significant univariate association with baPWV. In each model, baPWV served as the dependent variable, while the Korotkoff sound feature and covariates (age, diabetes, BMI, SBP) were entered as independent variables. Variance inflation factors (VIFs) were examined to assess multicollinearity (all VIF < 5).
Machine learning methods
Time-frequency images were obtained using a continuous wavelet transform (CWT). These representations were utilized as input for two CNN models, GoogLeNet and SqueezeNet, which were trained following a transfer learning paradigm to obtain stiffness-related information. A comprehensive description of the machine learning hyperparameters is available in the Supplementary Material.
Results
Participant characteristics
Time- and frequency-domain features
The statistical results for the ten extracted features are summarized in Table 3. No significant difference was observed in the maximum amplitude value between the older and young groups. This lack of difference may be attributed to the sensitivity of the maximum amplitude to factors such as sensor placement, variations in tissue layer thickness and density, and individual differences in blood flow. Although the sensor is aligned with the relative position of the brachial artery during signal acquisition, it is inevitably influenced by the properties of the lateral tissue of the brachial artery and differences in blood flow through the brachial artery. In contrast, the proposed center of mass feature demonstrated a statistically significant difference between the two groups. This finding suggests that while individual anatomical and physiological factors may influence absolute amplitude values, they exert a comparatively minor effect on the temporal location of the maximum amplitude, supporting the robustness of this feature.
In addition, skewness differed significantly between groups (Table 3), suggesting group-level differences in the Korotkoff sound envelope: the envelope distribution was left-skewed in older adults and right-skewed in young adults. Peak-frequency–related results suggested that spectral energy was concentrated at different frequency ranges between groups, with peak frequency showing a significant shift (Table 3). Center of gravity frequency and mean-square frequency showed nominal between-group differences (p < 0.05) but did not remain significant after Bonferroni correction.
All the features were entered into an exploratory logistic regression model. The model demonstrated a good fit per the Hosmer-Lemeshow test (p > 0.05) and achieved a classification accuracy of 83.7%. The specific information is shown in Table 4.
Although the conventional feature-based analysis demonstrated some ability to distinguish the age-defined groups/stiffness-related signatures, its classification accuracy remained limited. A principal challenge lies in the manual curation of the most discriminative features or identifying optimal multi-dimensional feature combinations to enhance the model's capability for assessing pathological signals. In contrast, deep learning networks possess a superior ability to automatically learn complex, high-dimensional feature hierarchies and approximate the optimal mapping function through iterative parameter optimization. To enable more automated and scalable screening of vascular stiffness-related signatures, we therefore developed and implemented deep learning models.
Verification
To evaluate clinical relevance, correlations between Korotkoff sound features and baPWV were analyzed (Table 5). Notably, several features (including center of mass, peak frequency, and skewness) showed modest correlations with measured baPWV, supporting the hypothesis that these acoustic characteristics are sensitive to vascular property differences. Nevertheless, the correlation coefficients were modest, indicating limited effect size; thus, these findings should be interpreted as preliminary evidence requiring replication in larger and independent cohorts.
To assess whether Korotkoff sound features provide information beyond established covariates, multivariable linear regression analyses were performed adjusting for age, diabetes status, BMI, and systolic blood pressure. After adjustment, skewness (β = 0.166, p = 0.030), center of mass (β = −0.310, p = 0.018), and peak frequency (β = −0.331, p = 0.029) remained significantly associated with baPWV. The negative coefficients indicate that higher values of center of mass and peak frequency are associated with lower baPWV (i.e., less stiffness), consistent with the between-group differences observed in the age-defined task. The relatively high adjusted R² values primarily reflect the contribution of established covariates (especially age and blood pressure), while the persistence of the acoustic features suggests a small independent association. Full model details are provided in the Supplementary Material Tables S3–S5.
CNN models
Figure 3 illustrates the progression of training accuracy and loss for the CNN models, indicating stable learning convergence. The corresponding classification performance is quantified using confusion matrices in Figure 4. Evaluation of the age-based group classification (older vs. young) revealed that both CNN architectures showed high performance in the age-defined task (Figure 4A). GoogLeNet correctly identified 84.0% of older-group cases (sensitivity) and 95.6% of young-group cases (specificity), with an overall accuracy of 89.3%. SqueezeNet exhibited a slightly higher sensitivity of 91.3% and a specificity of 92.3%, leading to an accuracy of 93.7% (see Supplementary Material Table 6).
Training accuracy and loss of googLeNet and squeezeNet. baPWV, brachial-ankle pulse wave velocity. (a) older and young groups. (b) High-baPWV and low-baPWV groups.
Model performance evaluation using confusion matrices. baPWV, brachial-ankle pulse wave velocity. The matrices present results for two binary classification tasks: (a) older group vs. young group and (b) high-baPWV group vs. low-baPWV group. Rows indicate the true labels, and columns indicate the predicted labels. The third row aggregates the total instances per true class and shows the Recall (Sensitivity) for each class. The third column aggregates the total instances per predicted class and shows the Precision for each class. The bottom-right cell shows the overall accuracy. Values in the main 2 × 2 cells represent counts and their percentage relative to the true class (row total).
In the independent baPWV-defined classification task (high baPWV vs. low baPWV; Figure 4B), both models showed moderate performance (Supplementary Table 7). While this suggests that the networks capture stiffness-related information not restricted to the age-defined labels, performance was lower than in the age-defined task and should be interpreted cautiously given the limited sample size and potential spectrum differences between cohorts.
Discussion
The assessment of arterial stiffness is closely linked to cardiovascular risk and is widely used to characterize vascular ageing and subclinical organ damage (17, 41, 42). However, the complexity, cost, and need for specialized operators limit widespread implementation of PWV, particularly in primary care workflows and in-home monitoring. This study therefore investigated the feasibility of extracting stiffness-related information from Korotkoff sounds recorded during routine cuff-based blood pressure measurement using engineered feature analysis and machine learning.
This study provides proof-of-concept evidence that Korotkoff sound analysis can differentiate between young and older individuals, groups expected to differ in vascular ageing and arterial stiffness based on the well-established association between age and PWV (43–45). Importantly, PWV was not directly measured in these two groups; therefore, these findings should be interpreted as discrimination of age-defined vascular characteristics rather than direct stiffness quantification or clinical risk stratification. In the separate hospital cohort with measured baPWV, selected features showed statistically significant associations with baPWV, providing supportive evidence for feasibility.
From a biological perspective, the link between vascular ageing and arterial stiffening is driven by integrated molecular and cellular processes across the vascular wall. A geroscience framework emphasizes that endothelial dysfunction (including impaired nitric oxide bioavailability), increased oxidative stress, chronic low-grade inflammation (“inflammaging”), mitochondrial dysfunction, impaired proteostasis, and the accumulation of senescent vascular cells with a senescence-associated secretory phenotype (SASP) contribute to progressive adverse vascular remodeling. In parallel, extracellular matrix changes, such as elastin fragmentation, increased collagen content and cross-linking, altered mechanotransduction, and, in some contexts, medial calcification, reduce arterial compliance and increase PWV. These processes provide a biologically plausible basis for why younger and older adults are expected to differ in vascular mechanical properties, even in the absence of overt cardiovascular disease, supporting the rationale for using age as a surrogate label in an initial feasibility comparison (46, 47).
Mechanistically, Korotkoff sounds are thought to arise from a combination of arterial wall vibration and hemodynamic phenomena during partial arterial compression, although the precise genesis remains an active area of research (19, 24). Recent experimental and modeling work has reinforced that both vessel wall mechanics and flow-related instabilities can contribute to sound generation and that the time–frequency characteristics are shaped by the coupled dynamics of pulsatile flow, arterial wall motion, cuff pressure, and vibration transmission through surrounding tissue (24). Increased arterial stiffness may alter the coupling between pulsatile flow, arterial wall vibration, and cuff-induced compression, which can plausibly shift the temporal asymmetry of the envelope and redistribute spectral energy. In this context, our observation that skewness and peak-frequency–related features differ between age-stratified groups is biologically plausible, because ageing-related arterial remodeling and reduced compliance can shift the dynamic response of the arterial wall to external compression and pulsatile flow (13, 48, 49).
Our findings are also consistent with prior efforts to derive vascular information from Korotkoff sounds. Earlier work reported age-related differences in Korotkoff sound characteristics as a proxy for vascular compliance (26), and recent studies have demonstrated that deep learning can extract clinically relevant information from Korotkoff sounds beyond conventional blood pressure estimation (25). Our approach emphasizes waveform- and time- frequency-derived acoustic descriptors combined with transfer-learning CNNs, offering an alternative pathway to extract stiffness-related signatures from routine cuff measurements.
Notably, the associations between individual Korotkoff sound features and baPWV were statistically significant but modest in magnitude. This is not unexpected because baPWV is influenced by multiple determinants including age, blood pressure, metabolic factors, and peripheral arterial properties, while Korotkoff sounds are additionally affected by cuff pressure dynamics, tissue characteristics, and sensor positioning. These differences in physiological territory and measurement determinants can attenuate correlations and reduce classification performance when labels are defined by baPWV rather than by age. In addition, the limited sample size of the baPWV cohort and potential spectrum differences between cohorts may constrain generalizability and performance. Therefore, the current results should be interpreted as feasibility evidence that Korotkoff sounds encode stiffness-related information, rather than as proof that these signals can replace standardized PWV measurement or provide substantial incremental risk stratification beyond age and blood pressure. Quantifying incremental value, head-to-head against estimated PWV derived from age and blood pressure, as well as multivariable clinical models, should be a central aim of future work (31).
To enable a more automated analysis, we applied transfer-learning CNNs (GoogLeNet and SqueezeNet) to classify Korotkoff sound time-frequency representations. Both architectures achieved high performance in distinguishing age-defined groups, outperforming traditional feature-based analysis. Considering potential implementation in mobile or portable devices (e.g., electronic sphygmomanometers), lightweight networks such as SqueezeNet may be advantageous in terms of computational efficiency. Because the primary labels were age-defined, these CNN results should be interpreted as proof-of-concept, and future studies should evaluate robustness across devices, measurement conditions, and populations.
Finally, while our findings support feasibility, establishing clinical utility will require additional validation steps. Larger cohorts spanning a wider range of vascular ageing should be studied with standardized PWV measurements, ideally cfPWV, to better characterize how Korotkoff sound–derived representations relate to arterial stiffness and whether they provide incremental value beyond conventional variables. Korotkoff sounds may also encode hemodynamic information beyond stiffness, but such applications remain speculative and will require dedicated study designs with appropriate labels and clinical endpoints (24).
Limitations
Several limitations of this study should be acknowledged. First, the primary comparison (older vs. young) used age as a surrogate for arterial stiffness rather than direct PWV measurement. Although this approach is supported by prior literature and complemented by the secondary analysis in a baPWV-measured cohort, standardized direct PWV measurements within the same individuals are needed to confirm the relationship. In addition, cfPWV (reference-standard aortic stiffness) was not measured; baPWV was used as a pragmatic comparator. Future studies should therefore incorporate direct cfPWV measurements for definitive validation (17). Second, the analyzed acoustic features were selected based on a priori knowledge; expanding feature diversity through a more comprehensive search may yield biomarkers that better capture stiffness-related information. Third, the generalizability and model performance may be constrained by the limited sample size and cohort differences, potentially limiting further gains in accuracy and robustness. Fourth, incremental value beyond age and blood pressure was not quantified; this is required before any risk-stratification claims can be made.
Clinical implications and future perspectives
Importantly, the current work should be interpreted as a feasibility and proof-of-concept study. The approach should be considered an adjunct rather than a substitute for established PWV assessment, and its incremental value beyond conventional variables remains to be determined. Future studies should: (i) validate performance against standardized direct PWV (preferably cfPWV) within the same individuals, (ii) evaluate test-retest reproducibility, (iii) quantify incremental value beyond conventional clinical variables, and (iv) examine associations with prospective cardiovascular outcomes to determine clinically meaningful thresholds and utility.
Conclusion
This study supports the feasibility of using machine-learning analysis of Korotkoff sounds to capture signals related to arterial stiffness and vascular ageing. The approach discriminated age-defined groups and demonstrated a statistically significant but modest association with baPWV in a baPWV-measured clinical cohort. Further validation against standardized direct PWV measurements (ideally cfPWV) and prospective outcome studies are needed before clinical risk-stratification or prognostic claims can be made.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Garcia-Rios A Ordovas JM. Chronodisruption and cardiovascular disease. Clin Investig Arterioscler. (2022) 34(Suppl 1):S 32–7. 10.1016/j.arteri.2021.12.00435125247 · doi ↗ · pubmed ↗
- 2North BJ Sinclair DA. The intersection between aging and cardiovascular disease. Circ Res. (2012) 110(8):1097–108. 10.1161/circresaha.111.24687622499900 PMC 3366686 · doi ↗ · pubmed ↗
- 3Wu S Jin C Li S Zheng X Zhang X Cui L Aging, arterial stiffness, and blood pressure association in Chinese adults. Hypertension. (2019) 73(4):893–9. 10.1161/HYPERTENSIONAHA.118.1239630776974 · doi ↗ · pubmed ↗
- 4Lee JG Joo SJ. Arterial stiffness and cardiovascular risk. Korean J Intern Med. (2019) 34(3):504–6. 10.3904/kjim.2019.11031048659 PMC 6506729 · doi ↗ · pubmed ↗
- 5Chirinos JA Segers P Hughes T Townsend R. Large-artery stiffness in health and disease. J Am Coll Cardiol. (2019) 74(9):1237–63. 10.1016/j.jacc.2019.07.01231466622 PMC 6719727 · doi ↗ · pubmed ↗
- 6Townsend RR Anderson AH Chirinos JA Feldman HI Grunwald JE Nessel L Association of pulse wave velocity with chronic kidney disease progression and mortality. Hypertension. (2018) 71(6):1101–7. 10.1161/hypertensionaha.117.1064829712736 PMC 6342478 · doi ↗ · pubmed ↗
- 7Banegas JR Townsend RR. Arterial stiffness and reference values. Rev Esp Cardiol (Engl Ed). (2020) 73(1):11–3. 10.1016/j.rec.2019.07.00431405793 · doi ↗ · pubmed ↗
- 8Laurent S Boutouyrie P Asmar R Gautier I Laloux B Guize L Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. (2001) 37(5):1236–41. 10.1161/01.hyp.37.5.123611358934 · doi ↗ · pubmed ↗