SGLT2 Inhibitor Use and Cardiorenal Outcomes in Type 2 Diabetes With Liver Cirrhosis
Mu-Chi Chung, Tung-Min Yu, Laing-You Wu, Ming-Ju Wu, Jeng-Jer Shieh, Chi-Jung Chung

TL;DR
This study finds that SGLT2 inhibitors may protect the kidneys, heart, and liver in patients with type 2 diabetes and liver cirrhosis.
Contribution
The study provides new evidence that SGLT2 inhibitors offer cardiorenal and hepatic benefits in patients with T2D and cirrhosis.
Findings
SGLT2 inhibitors were associated with reduced risks of end-stage kidney disease and acute kidney injury.
Use of SGLT2 inhibitors was linked to lower risks of cardiovascular events and all-cause mortality.
SGLT2 inhibitors showed reduced risk of hepatic decompensation events in patients with cirrhosis.
Abstract
This cohort study analyzes associations of sodium-glucose cotransporter–2 (SGLT2) vs dipeptidyl peptidase–4 inhibitor use with kidney outcomes, cardiovascular events, and hepatic decompensation in patients with concurrent type 2 diabetes (T2D) and liver cirrhosis. Is the use of sodium-glucose cotransporter–2 inhibitors (SGLT2is) associated with improved cardiorenal and hepatic outcomes in patients with type 2 diabetes (T2D) and liver cirrhosis? In this cohort study of 24 259 patients with T2D and cirrhosis, SGLT2is were associated with decreased risk of end-stage kidney disease, acute kidney injury, major adverse cardiovascular events, and all-cause mortality during a median follow-up of 2.3 years. SGLT2is were also associated with reduced risk of hepatic decompensation events, with consistent results across sensitivity and subgroup analyses. These findings suggest that SGLT2is may…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
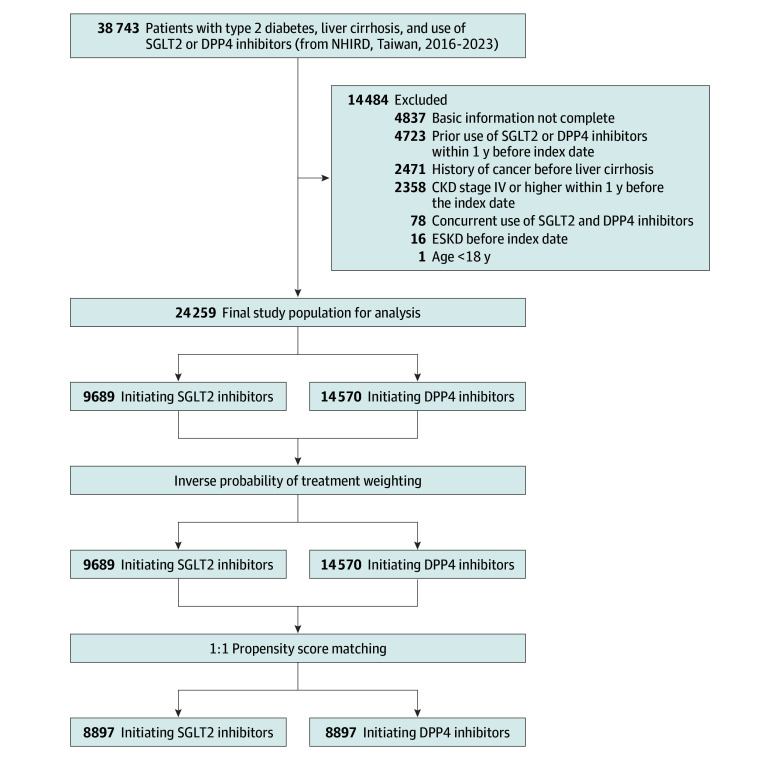 Figure 1
Figure 1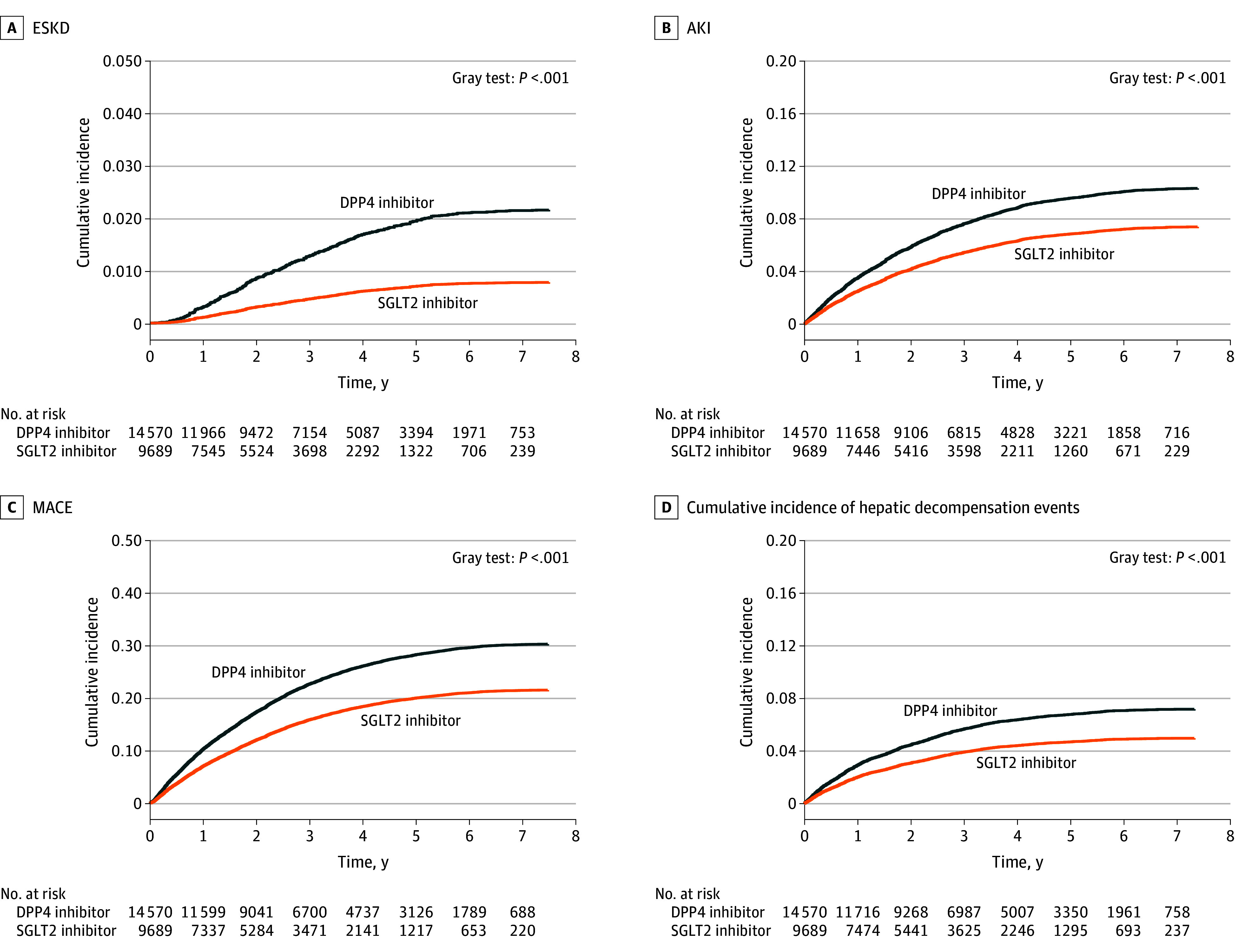 Figure 2
Figure 2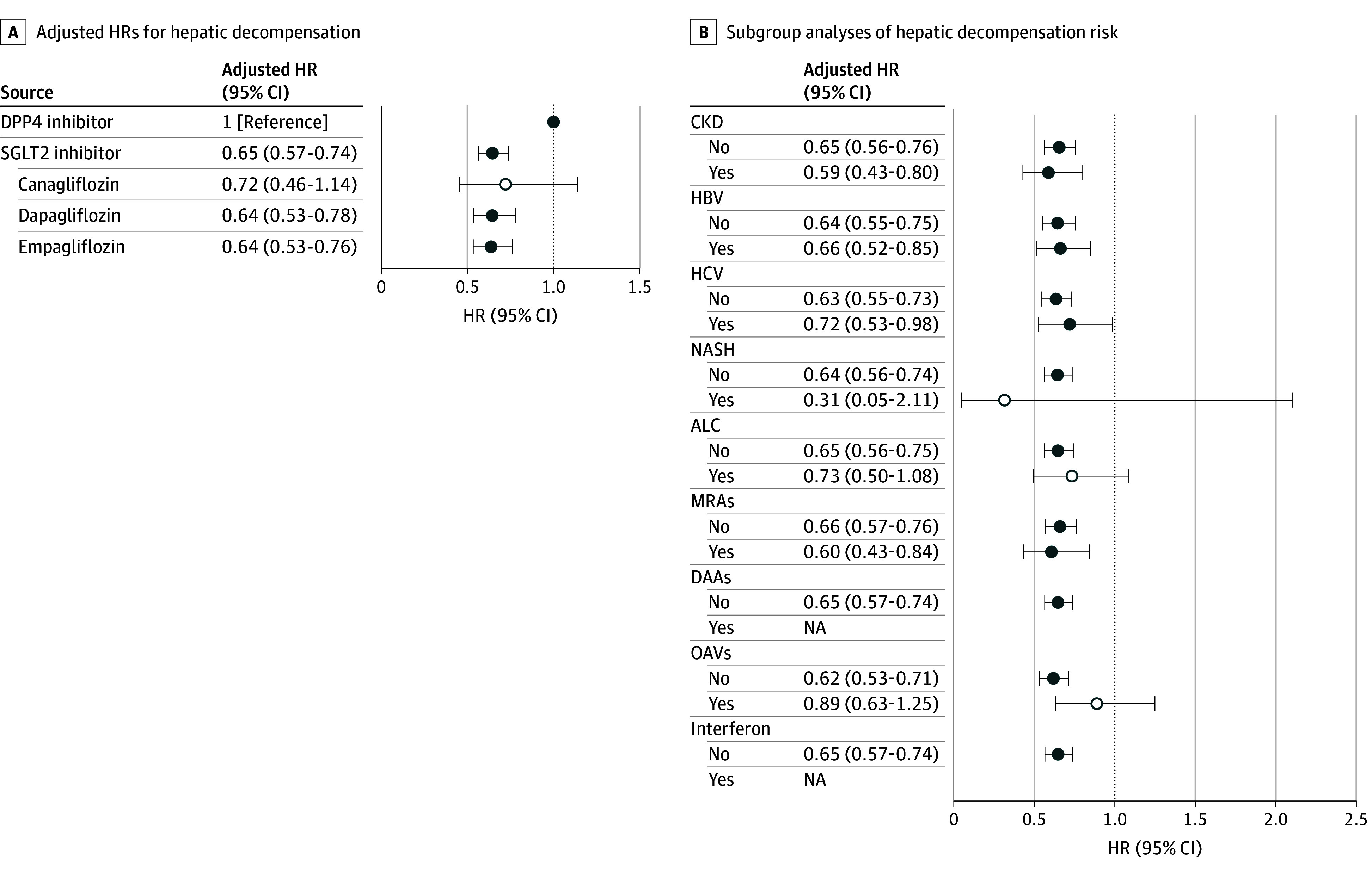 Figure 3
Figure 3| Characteristic | Patients, No. (%) | SMD | |||
|---|---|---|---|---|---|
| Overall (N = 24 259) | DPP4 inhibitors (n = 14 570) | SGLT2 inhibitors (n = 9689) | Unweighted | Weighted | |
| Diabetes duration, mean (SD), y | 9.99 (6.37) | 9.86 (6.34) | 10.18 (6.42) | 0.05 | 0.00 |
| Index year of receiving SGLT2 or DPP4 inhibitors | |||||
| 2016 | 1825 (7.52) | 1506 (10.34) | 319 (3.29) | 0.28 | 0.02 |
| 2017 | 2607 (10.75) | 2019 (13.86) | 588 (6.07) | 0.26 | 0.01 |
| 2018 | 2688 (11.08) | 1965 (13.49) | 723 (7.46) | 0.20 | −0.01 |
| 2019 | 3059 (12.61) | 1966 (13.49) | 1093 (11.28) | 0.07 | −0.01 |
| 2020 | 3568 (14.71) | 2085 (14.31) | 1483 (15.31) | −0.03 | 0.00 |
| 2021 | 3751 (15.46) | 1972 (13.53) | 1779 (18.36) | −0.13 | 0.00 |
| 2022 | 3537 (14.58) | 1664 (11.42) | 1873 (19.33) | −0.22 | 0.00 |
| 2023 | 3224 (13.29) | 1393 (9.56) | 1831 (18.90) | −0.27 | 0.00 |
| Age, y | |||||
| Mean (SD) | 64.68 (11.95) | 66.29 (12.18) | 62.25 (11.16) | −0.35 | −0.02 |
| 18-24 | 7 (0.03) | 3 (0.02) | 4 (0.04) | −0.01 | 0.00 |
| 25-34 | 111 (0.46) | 58 (0.40) | 53 (0.55) | −0.02 | 0.00 |
| 35-44 | 1060 (4.37) | 513 (3.52) | 547 (5.65) | −0.10 | 0.00 |
| 45-54 | 3731 (15.38) | 1975 (13.56) | 1756 (18.12) | −0.13 | 0.00 |
| 55-64 | 6976 (28.76) | 3836 (26.33) | 3140 (32.41) | −0.13 | 0.00 |
| 65-74 | 7224 (29.78) | 4325 (29.68) | 2899 (29.92) | −0.01 | −0.01 |
| 75-84 | 3981 (16.41) | 2886 (19.81) | 1095 (11.30) | 0.24 | 0.01 |
| ≥85 | 1169 (4.82) | 974 (6.68) | 195 (2.01) | 0.23 | 0.03 |
| Sex | |||||
| Female | 8229 (33.92) | 5520 (37.89) | 2709 (27.96) | 0.21 | 0.00 |
| Male | 16 030 (66.08) | 9050 (62.11) | 6980 (72.04) | ||
| Comorbidity | |||||
| Hypertension | 15 053 (62.05) | 9045 (62.08) | 6008 (62.01) | 0.00 | 0.00 |
| Hyperlipidemia | 12 049 (49.67) | 6614 (45.39) | 5435 (56.09) | −0.22 | 0.00 |
| Cerebral vascular disease | 2276 (9.38) | 1593 (10.93) | 683 (7.05) | 0.14 | −0.01 |
| Coronary artery disease | 4101 (16.91) | 2241 (15.38) | 1860 (19.20) | −0.10 | 0.00 |
| Chronic kidney disease | 4811 (19.83) | 2982 (20.47) | 1829 (18.88) | 0.04 | 0.02 |
| Hepatitis B virus | 5007 (20.64) | 2924 (20.07) | 2083 (21.50) | −0.04 | 0.00 |
| Hepatitis C virus | 3664 (15.10) | 2447 (16.79) | 1217 (12.56) | 0.12 | 0.02 |
| Acute myocardial infarction | 392 (1.62) | 175 (1.20) | 217 (2.24) | −0.08 | −0.01 |
| Stroke | 1786 (7.36) | 1275 (8.75) | 511 (5.27) | 0.14 | −0.01 |
| Heart failure | 1595 (6.57) | 878 (6.03) | 717 (7.40) | −0.05 | 0.01 |
| Nonalcoholic steatohepatitis | 281 (1.16) | 142 (0.97) | 139 (1.43) | −0.04 | 0.00 |
| Alcoholic liver cirrhosis | 1636 (6.74) | 1087 (7.46) | 549 (5.67) | 0.07 | 0.00 |
| Hypoglycemia | 451 (1.86) | 352 (2.42) | 99 (1.02) | 0.11 | 0.00 |
| Medication (diabetes) | |||||
| GLP-1 RAs | 138 (0.57) | 43 (0.30) | 95 (0.98) | −0.09 | 0.01 |
| Insulin | 2661 (10.97) | 1349 (9.26) | 1312 (13.54) | −0.14 | −0.01 |
| Metformin | 7367 (30.37) | 4435 (30.44) | 2932 (30.26) | 0.00 | −0.02 |
| Medication (other) | |||||
| Mineralocorticoid receptor antagonists | 1504 (6.20) | 1030 (7.07) | 474 (4.89) | 0.09 | 0.00 |
| Other diuretics | 2834 (11.68) | 1887 (12.95) | 947 (9.77) | 0.10 | 0.00 |
| Statins | 6648 (27.40) | 3442 (23.62) | 3206 (33.09) | −0.21 | −0.01 |
| Antiplatelet agents | 3672 (15.14) | 2037 (13.98) | 1635 (16.87) | −0.08 | 0.00 |
| ACEIs and ARBs | 8676 (35.76) | 4931 (33.84) | 3745 (38.65) | −0.10 | 0.00 |
| Direct-acting antivirals | 31 (0.13) | 24 (0.16) | 7 (0.07) | 0.03 | 0.00 |
| Oral antiviral agents | 2365 (9.75) | 1335 (9.16) | 1030 (10.63) | −0.05 | 0.00 |
| Interferon | 6 (0.02) | 6 (0.04) | 0 | NA | NA |
| Carvedilol | 744 (3.07) | 437 (3.00) | 307 (3.17) | −0.01 | −0.01 |
| Other nonselective β-blockers | 1738 (7.16) | 1116 (7.66) | 622 (6.42) | 0.05 | 0.00 |
| Exposure | Events, No. | Person-years | Incidence rate | Crude HR (95% CI) | Model 1, HR (95% CI) | Model 2, HR (95% CI) | |||
|---|---|---|---|---|---|---|---|---|---|
| End-stage kidney disease | |||||||||
| DPP4i (n = 14 570) | 339 | 46 949.41 | 7.22 | 1 [Reference] | NA | 1 [Reference] | NA | 1 [Reference] | NA |
| SGLT2i | |||||||||
| Any (n = 9689) | 60 | 26 096.79 | 2.30 | 0.33 (0.24-0.45) | <.001 | 0.33 (0.24-0.45) | <.001 | 0.34 (0.25-0.47) | <.001 |
| Canagliflozin (n = 735) | 4 | 1781.19 | 2.25 | 0.29 (0.11-0.79) | .02 | 0.28 (0.10-0.75) | .01 | 0.28 (0.10-0.75) | .01 |
| Dapagliflozin (n = 4907) | 26 | 12 983.44 | 2.00 | 0.31 (0.19-0.49) | <.001 | 0.31 (0.19-0.50) | <.001 | 0.33 (0.21-0.53) | <.001 |
| Empagliflozin (n = 4047) | 30 | 11 332.16 | 2.65 | 0.36 (0.24-0.54) | <.001 | 0.35 (0.23-0.53) | <.001 | 0.37 (0.24-0.56) | <.001 |
| Acute kidney injury | |||||||||
| DPP4i (n = 14 570) | 1708 | 45 291.06 | 37.71 | 1 [Reference] | NA | 1 [Reference] | NA | 1 [Reference] | NA |
| SGLT2i | |||||||||
| Any (n = 9689) | 568 | 25 573.71 | 22.21 | 0.65 (0.58-0.73) | <.001 | 0.66 (0.59-0.73) | <.001 | 0.66 (0.59-0.74) | <.001 |
| Canagliflozin (n = 735) | 37 | 1763.15 | 20.99 | 0.65 (0.45-0.94) | .02 | 0.63 (0.44-0.91) | .014 | 0.63 (0.44-0.91) | .01 |
| Dapagliflozin (n = 4907) | 268 | 12 736.44 | 21.04 | 0.60 (0.52-0.70) | <.001 | 0.61 (0.52-0.70) | <.001 | 0.62 (0.54-0.73) | <.001 |
| Empagliflozin (n = 4047) | 263 | 11 074.11 | 23.75 | 0.72 (0.61-0.84) | <.001 | 0.72 (0.61-0.84) | <.001 | 0.69 (0.59-0.82) | <.001 |
| MACE | |||||||||
| DPP4i (n = 14 570) | 5132 | 44 740.75 | 114.71 | 1 [Reference] | NA | 1 [Reference] | NA | 1 [Reference] | NA |
| SGLT2i | |||||||||
| Any (n = 9689) | 1640 | 25 061.92 | 65.44 | 0.66 (0.61-0.70) | <.001 | 0.67 (0.63-0.72) | <.001 | 0.67 (0.62-0.71) | <.001 |
| Canagliflozin (n = 735) | 116 | 1728.80 | 67.10 | 0.71 (0.58-0.88) | .002 | 0.70 (0.56-0.86) | .001 | 0.71 (0.58-0.88) | .001 |
| Dapagliflozin (n = 4907) | 811 | 12 458.70 | 65.10 | 0.66 (0.60-0.72) | <.001 | 0.68 (0.62-0.74) | <.001 | 0.69 (0.63-0.76) | <.001 |
| Empagliflozin (n = 4047) | 713 | 10 874.41 | 65.57 | 0.65 (0.59-0.71) | <.001 | 0.66 (0.60-0.72) | <.001 | 0.63 (0.58-0.69) | <.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Liver Disease Diagnosis and Treatment · Hormonal Regulation and Hypertension
Introduction
Type 2 diabetes (T2D) and liver cirrhosis frequently coexist and share a bidirectional association. Approximately 31% of patients with cirrhosis have T2D,^1^ and those with diabetes are approximately twice as likely to develop cirrhosis.^2^ When T2D and liver cirrhosis are present, patients face substantially worse outcomes, including increased risks of kidney complications,^3^ hepatic decompensation, and mortality.^2^
Despite the well-established cardiorenal benefits of sodium-glucose cotransporter–2 inhibitors (SGLT2is) in patients with T2D, their role in individuals with liver cirrhosis remains poorly understood. Most randomized clinical trials have excluded patients with advanced liver disease, leaving limited evidence on the safety and efficacy of SGLT2is in this high-risk population.^4^ In fact, few large-scale studies with long-term follow-up have specifically examined the effects of any antidiabetic therapy in patients with coexisting T2D and cirrhosis, making the broader association of diabetes medications with cirrhotic outcomes largely unknown.^2^
T2D is a key factor underlying nonalcoholic fatty liver disease (NAFLD), promoting hepatic steatosis, inflammation, and fibrosis.^5^ Emerging evidence suggests that SGLT2is may confer hepatic benefits, including reductions in NAFLD incidence, cirrhosis progression, and composite liver-related outcomes, outperforming other glucose-lowering agents.^6^ A recent US nationwide cohort study^7^ found that SGLT2i use was also associated with lower risks of both hepatic and extra-hepatic complications—such as cardiovascular disease (CVD) and chronic kidney disease (CKD)—in patients with diabetes and metabolic dysfunction–associated steatotic liver disease; however, that study excluded individuals with viral hepatitis and did not specifically evaluate those with liver cirrhosis.
To address this knowledge gap, we evaluated the associations of SGLT2is with cirrhosis of all causes. Given the historically high prevalence of viral hepatitis in Taiwan,^8,9^ understanding their role in viral-related cirrhosis is of particular importance. We conducted a nationwide cohort study using Taiwan’s National Health Insurance Research Database (NHIRD) to compare the kidney, cardiovascular, and hepatic outcomes between SGLT2i and dipeptidyl peptidase–4 inhibitor (DPP4i) users with T2D and cirrhosis.
Methods
Data Source
This cohort study utilized the Taiwan NHIRD, established in 1995, which contains comprehensive medical records for approximately 23 million citizens. The NHI program has mandatory enrollment and captures outpatient visits, hospitalizations, procedures, and prescription records. Taiwan’s National Health Research Institute authorizes database access for scientific investigations without requiring individual patient consent. The study received approval from China Medical University Hospital’s research ethics committee and adhered to their established guidelines and regulations (CRREC-109-018). Our methodological approach followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cohort studies.
Study Population and Design
We conducted a nationwide retrospective cohort analysis using deidentified data from Taiwan’s National Health Research Institutes. For privacy protection and to facilitate longitudinal tracking, personal identifiers were converted to unique encrypted codes. The study included adult patients with both T2D and liver cirrhosis diagnosed according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and *International Statistical Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) *(detailed coding available in the eTable 1 in Supplement 1).
T2D was defined as at least 3 outpatient consultations or 1 hospital admission within 12 months, a definition previously validated using the NHIRD.^10^ We identified liver cirrhosis cases using a validated approach requiring either 2 sequential outpatient diagnoses or a single inpatient diagnosis—a method used in multiple studies.^11,12^ This diagnostic algorithm has demonstrated a positive predictive value of 82.6% when 2 diagnostic codes are present,^13^ and similar algorithms have demonstrated positive predictive values up to 98% in Taiwan.^14^ In our study, 89.2% of patients also underwent abdominal ultrasonography before the diagnosis, providing further support for case validity.
We identified 38 743 patients who initiated SGLT2is or DPP4is between May 1, 2016 (when SGLT2is were first approved in Taiwan), and December 31, 2023. The index date was defined as the first prescription date after both T2D and cirrhosis had been established. Follow-up commenced immediately at the index date (t = 0) to eliminate immortal time bias, ensuring an uninterrupted exposure timeline for both groups (eFigure 1 in Supplement 1).
Exclusion criteria were age younger than 18 years, prior cancer, end-stage kidney disease (ESKD) or CKD stage IV or V before the index date, concurrent use of both medication classes, or any SGLT2i or DPP4i use within the preceding 12 months. Patients with cancer were excluded to focus on kidney and cardiovascular outcomes. The participant selection process is illustrated in Figure 1.
Participant Enrollment in Patients With Type 2 Diabetes and Liver CirrhosisCKD indicates chronic kidney disease; DPP4, dipeptidyl peptidase–4; ESKD, end-stage kidney disease; NHIRD, National Health Insurance Research Database; SGLT2, sodium-glucose cotransporter–2
Medication Exposure Assessment
This study examined 2 classes of antidiabetic medications: SGLT2is and DPP4is. SGLT2is included dapagliflozin, empagliflozin, and canagliflozin, while the DPP4is included alogliptin, linagliptin, sitagliptin, saxagliptin, and vildagliptin. We adopted an intention-to-treat approach to analyze data, evaluating outcomes on the basis of initial medication assignment regardless of subsequent treatment changes. To ensure clean exposure groups, we implemented a 365-day washout period (t = −365 to t = 0), excluding patients who had used either medication within 12 months before the index date.
Outcome Measurements
The primary outcomes comprised ESKD, acute kidney injury (AKI), and major adverse cardiovascular events (MACE). ESKD cases were identified through the Taiwan Catastrophic Illness Registry, a system established for reimbursement purposes that ensures diagnostic accuracy. For AKI identification, we employed validated ICD-9-CM and ICD-10-CM codes with previously established diagnostic performance (positive predictive value, 98.5%; negative predictive value, 74.0%) in the NHIRD.^15^ MACE was defined as a composite end point encompassing acute myocardial infarction (AMI), stroke, heart failure (HF), and all-cause mortality. Secondary outcomes included individual components of MACE (hospitalization for AMI, stroke, and HF) and indicators of hepatic decompensation (hospitalization for hepatic encephalopathy, ascites, peritonitis, or esophageal variceal bleeding). Definitions for AMI, stroke, and HF have been previously validated in the NHIRD.^16,17^ Peritonitis (including spontaneous bacterial peritonitis and cirrhosis-related peritonitis) was identified using ICD-9-CM codes 567.2, 567.8, and 567.9 and ICD-10-CM code K65.2. In addition, to maximize diagnostic specificity, all primary outcomes were identified using inpatient diagnosis codes. Because inpatient-only definitions may preferentially capture more severe events, we additionally prespecified a sensitivity analysis incorporating outpatient diagnoses for AMI, stroke, and HF.
Covariate Definition
Comorbidity profiles were assessed according to diagnostic codes documented within 1 year preceding the index date. The evaluated comorbidities included hypertension, hyperlipidemia, CVD, coronary artery disease, CKD, HF, viral hepatitis (both hepatitis B and C infections), nonalcoholic steatohepatitis, alcoholic cirrhosis, and hypoglycemia. Baseline cerebrovascular disease encompassed prior ischemic or hemorrhagic stroke, transient ischemic attack, and other chronic cerebrovascular disorders (ICD-9-CM codes 430-437 and ICD-10-CM codes I60-I63 and I66-I68), whereas the stroke MACE component referred to new-onset acute ischemic or hemorrhagic stroke during follow-up (ICD-9-CM codes 430-437, I61-I63, and I65-I66).
Medication use was assessed during the same 1-year baseline period. In addition to SGLT2is and DPP4is, we captured the use of glucagon-like peptide–1 receptor agonists, insulin, metformin, mineralocorticoid receptor antagonists, diuretics, statins, antiplatelet agents, renin-angiotensin system inhibitors (angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers), carvedilol, and other nonselective β-blockers. For patients with viral hepatitis, we additionally captured the use of direct-acting antivirals, oral antiviral agents, and interferon-based therapies during the same period.
Statistical Analysis
Descriptive statistics were reported as means (SDs) for continuous variables and frequencies (percentages) for categorical variables. To minimize confounding from baseline comorbidities and concomitant medication use, inverse probability of treatment weighting (IPTW) was employed. Propensity scores were estimated using multivariate logistic regression that included age, sex, index year, comorbidities, and medications use. Patients prescribed an SGLT2i received weights of 1 divided by the propensity score, and those prescribed a DPP4i received weights of 1 divided by (1 − propensity score). This method allocated greater analytical importance to individuals with lower probability of receiving their actual treatment. Stabilized weights were used to limit the impact of extreme values, as recommended in prior methodological work.^18^ The standardized mean difference, with a threshold of 0.10, was employed to evaluate the balance of covariates between groups.^19,20^
Patient follow-up commenced on the index date and continued until the occurrence of ESKD, AKI, MACE, hepatic decompensation, mortality, or the study termination (December 31, 2023), whichever came first. To account for competing mortality risks, we employed cause-specific hazard functions in all Cox regression analyses. Cumulative incidence functions accounting for the competing risk of death were estimated using the Aalen-Johansen estimator with IPTW. The Gray test was used to compare cumulative incidence between groups. Upon testing the proportional hazards assumption via Schoenfeld residual analysis and identifying violations, we implemented time-varying coefficient models in our weighted Cox proportional hazards regression. This approach allowed us to calculate both unadjusted and multivariable-adjusted hazard ratios (HRs) with corresponding 95% CIs for the association of SGLT2is with the risk of ESKD, AKI, MACE, and hepatic complications. To evaluate variations in treatment effects, we conducted additional stratified analyses examining the association of specific SGLT2i agents (dapagliflozin, empagliflozin, and canagliflozin) with our primary outcomes. We also performed subgroup analyses using adjusted Cox models to assess potential effect size modification by baseline comorbidities and concomitant medications.
Additionally, we conducted sensitivity analyses using propensity score trimming at various thresholds, 1:1 propensity score matching with a caliper width of 0.2 SDs,^21^ incorporation of outpatient diagnoses for AMI, stroke, and HF and stratified analyses by baseline CKD stage (defined by ICD-9-CM and ICD-10-CM codes) to assess the robustness of our findings. All statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc) and Python version 3.11.7 (Python Software Foundation), with 2-sided P < .05 considered statistically significant.
Results
Baseline Characteristics
A total of 24 259 patients with both T2D and liver cirrhosis (mean [SD] age, 64.68 [11.95] years; 8229 female [33.92%]) were identified, including 9689 patients (39.94%) receiving SGLT2is and 14 570 patients (60.06%) receiving DPP4is. Before weighting, SGLT2i users were younger (mean [SD] age, 62.25 [11.16] vs 66.29 [12.18] years) and included fewer females (2709 patients [27.96%] vs 5520 patients [37.89%]) compared with DPP4i users (Table 1). Among all participants, 5007 (20.64) had hepatitis B virus infection, 3664 (15.10%) had hepatitis C virus infection, and 1636 (6.74%) had alcohol-related liver disease. Hyperlipidemia was more prevalent in SGLT2i than DPP4i users (5435 patients [56.09%] vs 6614 patients [45.39%]), whereas cerebrovascular disease, hepatitis C infection, stroke, and hypoglycemia were more common in the DPP4i group. Insulin (1312 patients [13.54%] vs 1249 patients [9.26%]) and statin use (3206 participants [33.09%] vs 3442 participants [23.62%]) were more common among SGLT2i than DPP4i users. SGLT2i users had longer diabetes duration than DPP4i users (mean [SD], 10.18 [3.29] vs 9.86 [6.34] years). After IPTW, all baseline characteristics were well-balanced between the 2 groups, with standardized mean differences less than 0.10.
SGLT2i Use and Clinical Outcomes
During a median (IQR) follow-up of approximately 2.3 (1.0-4.0) years, the cumulative incidence curves demonstrated a consistently lower probability of ESKD, AKI, and MACE in SGLT2i users compared with DPP4i users (Gray test P < .001) (Figure 2). In the weighted population, SGLT2i use was associated with significantly reduced risk of ESKD (adjusted HR, 0.34; 95% CI, 0.25-0.47; P < .001), AKI (adjusted HR, 0.66; 95% CI, 0.59-0.74; P < .001), and MACE (adjusted HR, 0.67; 95% CI, 0.62-0.71; P < .001) compared with DPP4i use after adjusting for diabetes duration, age, sex, comorbidities, and concomitant medications (Table 2). These associations remained stable under various propensity score trimming analyses (eTable 2 in Supplement 1).
Cumulative Incidence Curves Comparing Outcomes for Sodium-Glucose Cotransporter–2 (SGLT2) vs Dipeptidyl Peptidase–4 (DPP4) Inhibitors in Patients With Type 2 Diabetes With Liver CirrhosisA, Cumulative incidence of end-stage kidney disease (ESKD). B, Risk of acute kidney injury (AKI). C, Probability of major adverse cardiovascular events (MACE) in the inverse probability treatment-weighted population. D, Cumulative incidence of hepatic decompensation.
Subgroup analyses showed broadly consistent findings across categories defined by age, sex, comorbidities, and medication use (eTable 3 in Supplement 1). Some smaller subgroups, such as those with prior AMI or hypoglycemia, had wider 95% CIs, but effect size estimates remained directionally similar.
For hepatic decompensation, SGLT2i therapy was associated with a lower incidence compared with DPP4i therapy (Gray test P < .001) (Figure 3A), even adjusting for other risk factors (HR, 0.65; 95% CI, 0.57-0.74; P < .001) (Figure 3B). In the subgroup analysis, the beneficial association of SGLT2is was consistent across most key subgroups (Figure 3C), including patients with and without CKD or hepatitis B infection. Although estimates also favored SGLT2is in smaller subgroups, such as those with hepatitis C virus or nonalcoholic steatohepatitis, 95% CIs were wider and did not reach statistical significance.
Forest Plots for Hazard of Hepatic Decompensation Risk Comparing Sodium-Glucose Cotransporter–2 (SGLT2) vs Dipeptidyl Peptidase–4 (DPP4) Inhibitors in Patients With Type 2 Diabetes With Liver CirrhosisA, Adjusted hazard ratios (HRs) for hepatic decompensation by SGLT2 inhibitor type. B, Subgroup analyses of associations of treatment with hepatic decompensation risk stratified by comorbidities and concomitant medications. Solid circles denote estimates that are statistically significant (P < .05), where the 95% CIs do not cross the null value (HR = 1.00). Open circles denote estimates that did not reach statistical significance (P ≥ .05). ALC indicates alcoholic cirrhosis; CKD, chronic kidney disease; DAAs, direct-acting antivirals; HBV, hepatitis B virus; HCV, hepatitis C virus; MRAs, mineralocorticoid receptor antagonists; NA, not applicable; NASH, nonalcoholic steatohepatitis; OAVs, oral antiviral agents.
For MACE components, SGLT2i users exhibited significantly lower risks of AMI (adjusted HR, 0.60; 95% CI, 0.45-0.80; P < .001), stroke (adjusted HR, 0.72; 95% CI, 0.61-0.85; P < .001), and all-cause mortality (adjusted HR, 0.58; 95% CI, 0.53-0.63; P < .001), whereas there was no significant association with HF (eFigure 2 in Supplement 1). Additionally, SGLT2i use was associated with reduced risk of hepatic decompensation events, particularly ascites (adjusted HR, 0.65; 95% CI, 0.55-0.76; P < .001), peritonitis (adjusted HR, 0.62; 95% CI, 0.45-0.86; P < .001), and esophageal variceal bleeding (adjusted HR, 0.67; 95% CI, 0.45-0.99; P = .04).
Sensitivity Analysis
We included 17 794 patients (8897 in each group) in the propensity score–matched cohort. Baseline characteristics were well-balanced between groups (all standardized mean differences <0.10) (eTable 4 in Supplement 1). In the matched cohort, SGLT2i use remained associated with significantly reduced risks of ESKD (adjusted HR, 0.30; 95% CI, 0.15-0.60; P < .001), AKI (adjusted HR, 0.66; 95% CI, 0.56-0.78; P < .001), MACE (adjusted HR, 0.63; 95% CI, 0.58-0.69; P < .001), and hepatic decompensation (adjusted HR, 0.63; 95% CI, 0.51-0.78; P < .001) (eTable 5 in Supplement 1), findings consistent with our primary IPTW analysis.
In addition, sensitivity analyses incorporating outpatient diagnoses of AMI, stroke, and HF showed similar findings (eTable 6 in Supplement 1). In stratified analyses by CKD stage, the protective associations of SGLT2is with ESKD, AKI, MACE, and hepatic decompensation remained evident regardless of baseline kidney function (eTable 7 in Supplement 1).
Discussion
This cohort study provides new evidence supporting the use of SGLT2is in patients with T2D and liver cirrhosis, demonstrating significant associations with reductions in the risks of ESKD, AKI, and MACE, as well as hepatic decompensation events. Importantly, these protective associations were consistent across the full spectrum of cirrhosis causes, including viral hepatitis, alcoholic liver disease, and nonalcoholic steatohepatitis, and remained robust after multivariable adjustment. These findings extend the established cardiorenal benefits of SGLT2is to a population previously underrepresented in clinical trials.
In our cohort, baseline characteristics indicated that about one-fifth of patients had hepatitis B virus infection, 15% had hepatitis C virus infection, and 7% had alcohol-related liver disease, suggesting viral hepatitis as the predominant underlying condition in this cirrhotic population. Because all patients had T2D, NAFLD was likely a major cause among the remaining cases. Given the shared metabolic pathways, we also referred to some NAFLD studies to extend our understanding of SGLT2i effects in patients with cirrhosis with metabolic risk factors.
CVD is the leading cause of death in patients with NAFLD,^22^ and NAFLD was associated with a 90% increased CVD risk in patients with T2D,^23^ due to poor glycemic control, insulin resistance, inflammation, and oxidative stress,^22^ all of which are improved by SGLT2is.^24^ Cirrhosis may further exacerbate cardiovascular dysfunction through hyperdynamic circulation, systemic inflammation, and neurohormonal dysregulation, resembling decompensated HF.^4^ SGLT2is have shown benefits in HF with both preserved and reduced ejection fraction,^25^ likely through natriuresis, hemodynamic relief, and anti-inflammatory effects, which may also explain the reduced MACE risk in patients with cirrhosis using SGLT2is.^4^ Our findings suggest that SGLT2is retain their cardioprotective effects in patients with T2D and liver cirrhosis.
NAFLD also increases the risk of CKD, through inflammation, and metabolic pathways,^26^ and greater NAFLD severity correlates with higher kidney risk.^27^ In parallel, AKI is a frequent and severe complication in cirrhosis,^28^ with kidney failure significantly increasing mortality by 7-fold.^29^ The risk of dialysis is highest in patients with both T2D and cirrhosis,^3^ underscoring the importance of preventing both CKD and AKI in this population.
SGLT2is have demonstrated protective kidney effects in CKD progression and reduced AKI risk in both clinical trials^30^ and cohort studies.^31^ In our study, these kidney benefits were preserved in patients with T2D and cirrhosis. One possible mechanism is the natriuretic effect of SGLT2is, which may reduce ascites formation and limit the need for traditional diuretics, particularly mineralocorticoid receptor antagonists and loop diuretics, which are often associated with hepatorenal syndrome. SGLT2i use has been shown to safely reduce ascites recurrence without compromising kidney function,^4^ and is associated with lower ascites-related mortality compared with DPP4is.^32^ These findings suggest SGLT2is may mitigate kidney complications in this high-risk population by reducing diuretic-associated kidney injury.
We also observed a reduction in hepatic decompensation events. While the reduction in peritonitis risk is a novel observation, it is supported by a prior meta-analysis showing decreased rates of gastroenteritis with SGLT2i use.^33^ Moreover, SGLT2is have been associated with reduced esophageal variceal bleeding risk compared with DPP4is^34^ and thiazolidinedione,^35^ supporting the hepatic benefits observed in our cohort.
Viral hepatitis has been associated with worse cardiovascular^36^ and kidney outcomes,^37^ potentially through mechanisms such as atherogenesis, proinflammatory cytokines, and oxidative stress.^38^ Steatosis in chronic hepatitis B virus infection may further contribute to lipid peroxidation and systemic inflammation,^39^ suggesting a potential therapeutic role for SGLT2is in this setting. A recent study reported reduced hepatocellular carcinoma risk in patients with T2D and hepatitis B treated with SGLT2is.^40^ Although data remain limited, our results suggest that the cardiorenal benefits of SGLT2is appear to extend to viral hepatitis-related cirrhosis as well.
Strengths and Limitations
Strengths of this study include the use of a large, nationwide cohort, validated diagnostic algorithms, and comprehensive adjustment for comorbidities and medication use. IPTW enhanced covariate balance while retaining statistical power. Our study addresses potential lead-time bias through several design features. First, we adjusted for both diabetes duration and index year in our propensity score model to account for temporal changes in prescribing practices. Second, after IPTW, SGLT2i users had longer diabetes duration than DPP4i users (10.18 vs 9.86 years), confirming that treatment was not initiated earlier in the disease course.
Some limitations should be acknowledged. The lack of laboratory data precluded assessment of cirrhosis severity, and lifestyle factors such as alcohol consumption were unavailable. Although alcoholic cirrhosis was included as a diagnostic category, residual confounding cannot be fully excluded. Furthermore, despite the use of IPTW to balance baseline characteristics between SGLT2i and DPP4i users, confounding by indication may still persist.
Conclusions
In this cohort study, we found that SGLT2is were associated with significantly lower risk of ESKD, AKI, MACE, and hepatic decompensation among patients with T2D and cirrhosis. By interrupting key metabolic and hemodynamic pathways underlying T2D and liver disease, SGLT2is may offer meaningful clinical benefits for this high-risk population. Prospective studies are warranted to confirm these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee WG, Wells CI, Mc Call JL, Murphy R, Plank LD. Prevalence of diabetes in liver cirrhosis: a systematic review and meta-analysis. Diabetes Metab Res Rev. 2019;35(6):e 3157. doi:10.1002/dmrr.315730901133 · doi ↗ · pubmed ↗
- 2Elkrief L, Rautou PE, Sarin S, Valla D, Paradis V, Moreau R. Diabetes mellitus in patients with cirrhosis: clinical implications and management. Liver Int. 2016;36(7):936-948. doi:10.1111/liv.1311526972930 · doi ↗ · pubmed ↗
- 3Sheen YJ, Kung PT, Sheu WH, Kuo WY, Tsai WC. Impact of liver cirrhosis on incidence of dialysis among patients with type 2 diabetes. Diabetes Ther. 2020;11(11):2611-2628. doi:10.1007/s 13300-020-00919-632901421 PMC 7547941 · doi ↗ · pubmed ↗
- 4Siafarikas C, Kapelios CJ, Papatheodoridi M, Vlachogiannakos J, Tentolouris N, Papatheodoridis G. Sodium-glucose linked transporter 2 inhibitors in liver cirrhosis: beyond their antidiabetic use. Liver Int. 2024;44(4):884-893. doi:10.1111/liv.1585138293770 · doi ↗ · pubmed ↗
- 5Hickman IJ, Macdonald GA. Impact of diabetes on the severity of liver disease. Am J Med. 2007;120(10):829-834. doi:10.1016/j.amjmed.2007.03.02517904449 · doi ↗ · pubmed ↗
- 6Khanmohammadi S, Habibzadeh A, Kamrul-Hasan ABM, Schuermans A, Kuchay MS. Glucose-lowering drugs and liver-related outcomes among individuals with type 2 diabetes: a systematic review of longitudinal population-based studies. Diabet Med. 2024;41(11):e 15437. doi:10.1111/dme.1543739340770 · doi ↗ · pubmed ↗
- 7Mao X, Zhang X, Kam L, . Synergistic association of sodium-glucose cotransporter-2 inhibitor and metformin on liver and non-liver complications in patients with type 2 diabetes mellitus and metabolic dysfunction-associated steatotic liver disease. Gut. 2024;73(12):2054-2061. doi:10.1136/gutjnl-2024-33248139122360 · doi ↗ · pubmed ↗
- 8Yu ML, Chen PJ, Dai CY, . 2020 Taiwan consensus statement on the management of hepatitis C: part (I) general population. J Formos Med Assoc. 2020;119(6):1019-1040. doi:10.1016/j.jfma.2020.04.00332359879 · doi ↗ · pubmed ↗