Patient‐ and Clinician‐Reported Outcomes and Outcome Measures Evaluating Timing of Implant Placement in the Edentulous Maxilla: A Systematic Review of Clinical Studies
Giuseppe A. Romito, Isabella Neme Ribeiro dos Reis, Mohamed A. Hassan, Cristina Cunha Villar, Helena Francisco, Claudio Mendes Pannutti

TL;DR
This paper reviews clinical studies to identify patient and clinician-reported outcomes used in evaluating implant placement timing in the edentulous maxilla.
Contribution
The study systematically reviews PROs and ClinROs in implant timing studies, highlighting the need for standardized outcome measures.
Findings
PROs included oral health-related quality of life, pain intensity, and satisfaction with prosthesis.
ClinROs like implant survival and prosthetic complications were reported in a minority of studies.
Outcomes varied widely, with limited comparability due to inconsistent assessment methods.
Abstract
To address what patient‐reported outcomes (PROs) and clinician‐reported outcomes (ClinROs) have been reported, and what measures (PROMs and CROMs) have been used to assess them in clinical studies on the timing of implant placement in the edentulous maxilla? Systematic searches were conducted in five databases to identify longitudinal prospective clinical studies. PROMs, CROMs, and methods were extracted. Risk of bias was assessed based on study design, and outcomes were analyzed descriptively. Thirteen studies were included: 1 randomized controlled trial and 12 case series. Delayed placement was reported in 9 studies, immediate in 2, and both in 2. Regarding PROs, 16 outcomes were identified, including oral health‐related quality of life (reported in 53.85%), pain intensity (38.46%), satisfaction with the prosthesis (23.08%), postoperative drug use (15.38%), and outcomes related to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
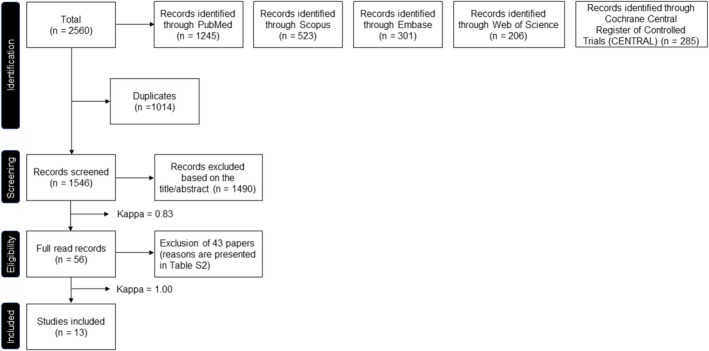 FIGURE 1
FIGURE 1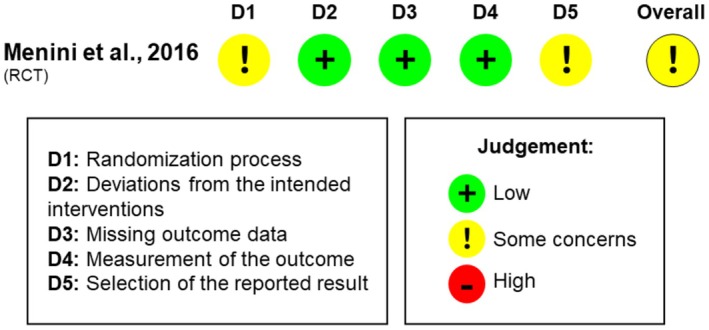 FIGURE 2
FIGURE 2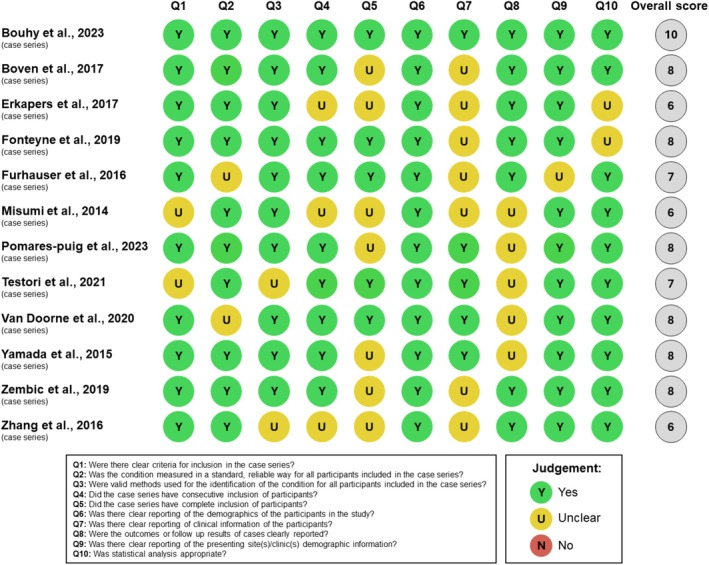 FIGURE 3
FIGURE 3| Study | Country | Study setting (university or private practice) | Study design | Number of arms | Funding | Number of patients (included/baseline/last follow‐up) | Sex (female/male) | Mean age (years) | Study's maximum follow‐up | Primary outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Bouhy et al. ( | Belgium | University | Case series | One | Yes | 30/29/27 | 13/17 | 66.4 ± 7.7 years (range: 48–82 years) | 5 years after implant placement | Prosthodontic survival rate |
| Boven et al. ( | Netherlands | University | Case series | One | Yes | 50/50/45 | 26/24 | 58.75 ± 9.03 years (range: 42–74 years) | 5 years after implant placement | NR |
| Erkapers et al. ( | United States and Sweden | University | Case series | One | Yes | 51/51/45 | 27/24 | 65.8 (range: 47–83 years) | 3 years after implant placement | OHIP‐49 scores |
| Fonteyne et al. ( | Belgium | University and private practice | Case series | One | No | 32/30/25 | 13/17 | 62.2 ± 9.0 years | 6 months after implant placement (on the day the final prosthesis was installed) | NR |
| Fürhauser et al. ( | Austria | University | Case series | One | No | 50 | 27/23 | 59.75 years | 1 week after implant placement | NR |
| Menini et al. ( | Italy | University | RCT | Two (Split‐mouth RCT) | No | 11 | 8/3 | 63.4 years (range: 51–75 years) | 48 h after implant placement | Swelling and pain control |
| Misumi et al. ( | Japan | University | Case series | One | No | 10 | 3/7 | 62 years (range: 53–76 years) | 3 months after the definitive prosthesis placement | OHIP‐14 scores |
| Pomares‐Puig et al. ( | Spain | Private practice | Case series | One | No | 10 | 3/7 | 56.6 ± 11.02 years | 7 days after implant placement | Accuracy of implant placement |
| Testori et al. ( | Italy | Private practice | Case series | One | No | 10 | 6/4 | 71.10 ± 11.02 years (range: 59–87 years) | 1 year | NR |
| Van Doorne et al. ( | Belgium | University | Case series | One | Yes | 31/31/29 | 14/17 | 62.30 ± 9.28 years | 2 years | NR |
| Yamada et al. ( | Japan | Private practice | Case series | One | Yes | 50/48/48 | 22/26 | 56.0 ± 8.3 years (range: 34–74 years) | 1 year | NR |
| Zembic et al. ( | Netherlands | University | Case series | One | Yes | 21/21/16 | 6/15 | 63 years (range: 52–81 years) | 4 years | NR |
| Zhang et al. ( | China | University | Case series | One | Yes | 12/11 | 8/4 | 56.3 years (range: 40–73 years) | 10 years | NR |
| Study | Timing of implant placement | Timing of loading | Bone grafting | Implants placed only in maxilla or maxilla and mandible | Number of implants (baseline/last follow‐up) | Number of implants per patient | Implant type | Type of prosthesis (fixed or removable) |
|---|---|---|---|---|---|---|---|---|
| Bouhy et al. ( | Delayed | Delayed loading | No | Maxilla | 116/108 | 4 | Standard implants | Removable (overdenture) |
| Boven et al. ( | Delayed | Delayed loading | In some cases, a sinus lifting procedure was performed using autogenous bone prior to implant placement, and implants were placed after the healing period | Maxilla | 300/295 | 6 | Standard implants | Removable (overdenture) |
| Erkapers et al. ( | Delayed | Delayed loading | No | Maxilla | 306/263 | 6 | Standard implants | Fixed (screw‐retained) |
| Fonteyne et al. ( | Delayed | Delayed loading | No | Maxilla | NR | 5–6 | Mini‐dental implants | Removable (overdenture) |
| Fürhauser et al. ( | Immediate (implants were placed immediately following extractions, during the same surgical procedure) | Immediate loading | No | Maxilla and mandible | 200 | 4 | Standard implants | Fixed (screw‐retained) |
| Menini et al. ( | Some immediate (implants were placed immediately following extractions, during the same surgical procedure) and some delayed | Immediate loading | No | Maxilla and mandible | 44 | 4 | Standard implants | Fixed (the method of retention was not reported) |
| Misumi et al. ( | Delayed | Immediate loading | No | Maxilla or maxilla and mandible | 65 | 4–6 | Standard implants | Fixed (screw‐retained) |
| Pomares‐puig et al. ( | Some immediate (implants were placed immediately following extractions, during the same surgical procedure) and some delayed | Immediate loading | In some cases, using a mixture of autogenous bone, xenograft and a collagen membrane | Maxilla and mandible | 48 | 4–8 | Standard implants | Fixed (screw‐retained) |
| Testori et al. ( | Immediate (implants were placed immediately following extractions, during the same surgical procedure) | Immediate loading | In some cases, using xenograft and/or collagen membrane or L‐PRF | Maxilla and mandible | 46/45 | 4–7 | Standard implants | Fixed (screw‐retained) |
| Van Doorne et al. ( | Delayed | Delayed loading | No | Maxilla | 185/166 | 5–6 | Mini‐dental implants | Removable (overdenture) |
| Yamada et al. ( | Delayed | Immediate loading | No | Maxilla | 290/278 | 4–6 | Standard implants | Fixed (screw‐retained) |
| Zembic et al. ( | Delayed | Delayed loading | In some cases. In case of minor bone defects, guided bone regeneration procedures not compromising primary implant stability were applied. The materials used were not reported | Maxilla | 42/32 | 2 | Standard implants | Removable (overdenture) |
| Zhang et al. ( | Delayed | Early loading | No | Maxilla | 91/83 | 6–8 | Standard implants | Fixed (segmented, cement‐retained) |
| Study | Timing of implant placement | Patient‐reported outcome measures (PROMs) | Evaluated question (key aspects/domains) | Methods | Interpretation | Analysis metric | Method of aggregation | Time point | Pre‐/Post‐intervention analysis (PROs/PROMs) |
|---|---|---|---|---|---|---|---|---|---|
| Bouhy et al. ( | Delayed |
Oral Health Impact Profile 20 (OHIP‐20) Patient satisfaction questionnaire—An adaptation of the McGill Denture Satisfaction |
Oral health‐related quality of life (domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap) Patient satisfaction with the prosthesis |
|
| Point estimates at each time point |
| Baseline (before implant placement), 1, 3, and 5 years after implant placement |
|
| Boven et al. ( | Delayed |
Functional complaints about the prosthesis Patients' eating ability Patient overall satisfaction with the treatment |
Functional complaints about the prosthesis ( Patients' eating ability (how well the patient could eat soft, tough, and hard food) Patient overall satisfaction with the treatment |
|
| Point estimates at each time point |
| Baseline (before implant placement), and 5 years after implant placement |
|
| Erkapers et al. ( | Delayed |
Oral Health Impact Profile (OHIP‐49) |
Oral health‐related quality of life (domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap) |
|
| Point estimates at each time point |
| Baseline (before implant placement), 12 weeks, 6 months, 1, 2 and 3 years after implant placement |
|
| Fonteyne et al. ( | Delayed |
Oral Health Impact Profile (OHIP‐14) Speech measured by one OHIP‐14 question Overall satisfaction with oral health Satisfaction with speech |
Phonetic evaluation (articulation and oromyofunctional behavior) Oral health‐related quality of life (domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap) Overall satisfaction with oral health Satisfaction with speech |
|
| Point estimates at each time point |
| Beseline (before implant placement), provisional loading, final connection (6 months after implant placement) |
|
| Fürhauser et al. ( | Immediate |
Postoperative pain intensity Postoperative swelling Impairment in everyday life and work after surgery |
Postoperative pain intensity Postoperative swelling Impairment in everyday life and work after surgery (days until resuming everyday life and work, perception of temporary prosthesis as a foreign body, impairment regarding food intake after surgery, impairment due to prosthetic complications, impairment regarding speech after surgery, and willingness to undergo the procedure again) |
|
| Point estimates at each time point |
|
|
|
| Menini et al. ( | Some immediate and some delayed |
Pain Psychosocial impact (comfort) of using the device RecoveryRx Postoperative drug use. |
Pain Psychosocial impact (comfort) of using the RecoveryRx device, a non‐invasive, disposable patch for managing postoperative swelling and pain with a 27.12 MHz electromagnetic field, was evaluated based on invasiveness, hygiene maneuvers, alimentation, and rest Postoperative drug use (type of non‐steroidal anti‐inflammatory drug (NSAIDs) and doses taken) |
|
| Point estimates at each time point |
|
|
|
| Misumi et al. ( | Delayed |
Oral Health Impact Profile (OHIP‐J14) |
Oral health‐related quality of life (domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap) |
|
The total range is 0–56. A score of 56/56 is indicative for maximal negative appreciation and 0/56 indicates that there are no issues at all | Point estimates at each time point |
| Baseline (before implant placement), 1 week after immediate restoration placement, 1 week after secondary provisional restoration placement, and 3 months after final restoration placement |
|
| Pomares‐puig et al. ( | Some immediate and some delayed |
Patient well‐being during the surgical procedure Intraoperative pain Satisfaction during the surgery Oral Health Impact Profile (OHIP‐14) Intake of analgesic and anti‐inflammatory medication Postoperative pain |
Patient well‐being during the surgical procedure (questions were related to the duration of the surgery, discomfort, ease of keeping the mouth open, willingness to repeat the procedure, recommendation of the procedure to others, and perceived accuracy and results of the guided technique) Oral health‐related quality of life (domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap) Intraoperative pain Satisfaction during the surgical procedure Intake of analgesics and anti‐inflammatory medication and postoperative pain |
|
| Point estimates at each time point |
|
|
|
| Testori et al. ( | Immediate |
Postsurgery quality of life Postprosthetic quality of life |
The postsurgical quality of life questionnaire evaluated pain management (pain and need for painkillers), physical symptoms (swelling, bruising, bleeding), daily functioning (sleep, chewing, speaking), and general well‐being (nausea, taste alterations) The postprosthetic quality of life questionnaire evaluated the overall esthetic result, color, shape, and size of the prosthesis (new teeth), appearance of the gingival tissue, chewing ability, speech, home‐care hygiene performance, and how closely the result met the patient's expectations |
|
| Point estimates at each time point |
|
|
|
| Van Doorne et al. ( | Delayed |
Pain Patient satisfaction |
Pain Patient satisfaction during the treatment, assessing inconveniences experienced during the process, and whether the patient would recommend the treatment to others |
|
| Point estimates (scores for pain and categorize satisfaction as ‘yes’ or ‘no’), at each time point |
|
|
|
| Yamada et al. ( | Delayed |
Oral Health Impact Profile (OHIP‐J49) Postoperative pain |
Oral health‐related quality of life (domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap) Postoperative pain |
|
| Point estimates at each time point |
|
|
|
| Zembic et al. ( | Delayed |
Oral Health Impact Profile (OHIP‐EDENT) Patient satisfaction with the prosthesis | Oral health‐related quality of life (domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap) and the impact of the prosthetic treatment on the quality of life, and patient satisfaction |
|
| Point estimates at each time point |
|
|
|
| Zhang et al. ( | Delayed |
Patient satisfaction with the prosthesis | Patient satisfaction, |
| Ratings of “excellent” and “good” reflect positive satisfaction, while “fair” and “poor” indicate areas where the patient experienced dissatisfaction or challenges. | Point estimates at each time point |
| Baseline (immediately after prosthesis placement), 1, 3, 5, and 10 years. |
|
| Study | Timing of implant placement | Clinician‐reported outcome measures (CROMs) | Methods | Interpretation | Analysis metric | Method of aggregation | Time point | Pre‐/Post‐intervention analysis (ClinROs/CROMs) |
|---|---|---|---|---|---|---|---|---|
| Bouhy et al. ( | Delayed |
Prosthodontic outcomes – Prosthetic complications Prosthodontic success Acceptable prosthodontic maintenance events Prosthesis failure (repeated fractures of the overdenture for which the installation of a metallic reinforcement was then necessary) Implant survival Sulcular Modified Bleeding Index Plaque Index Probing depth |
|
| Point estimates at each time point |
|
|
|
| Boven et al. ( | Delayed |
Implant survival Peri‐implant bone level changes Modified plaque Index Presence of calculus Peri‐implant inflammation Sulcular Modified Bleeding Index Probing depth |
|
Probing depth: NA |
|
| 5 years after implant placement |
|
| Erkapers et al. ( | Delayed |
Prosthetic complications |
|
| Point estimates at each time point |
| 3 and 6 months, 1, 2, and 3 years |
|
| Fonteyne et al. ( | Delayed |
Articulation Oromyofunctional behavior |
|
| Point estimates at each time point |
| Beseline (before implant placement), provisional loading, final connection (6 months after implant placement) |
|
| Menini et al. ( | Some immediate and some delayed |
Swelling |
|
| Point estimates at each time point |
| Assessed 48 h after the surgery |
|
| Pomares‐puig et al. ( | Some immediate and some delayed |
Accuracy variables (implant position deviation) |
|
| Point estimates of deviation |
| After implant placement (before abutment connection) |
|
| Testori et al. ( | Immediate |
Implant survival Prosthetic survival |
|
| Point estimates at each time point |
| 1 year and 8 months (20 months) |
|
| Van Doorne et al. ( | Delayed |
Implant survival Prosthetic survival |
|
| Point estimates at each time point |
| 6 months, 1 and 2 years |
|
| Yamada et al. ( | Delayed |
Insertion torque Surgical time Implant survival. Prosthetic survival. Peri‐implant bone level changes Post operative swelling Complications (surgical, with the provisional and postoperative) |
|
|
|
|
|
|
| Zhang et al. ( | Delayed |
Implant success Prosthetic success Prosthetic–Technical complications Modified Plaque Index Probing depth Sulcular Modified Bleeding Index Peri‐implant bone level changes—Marginal bone loss Peri‐implantitis |
|
|
|
|
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Implant Techniques and Outcomes · Orthodontics and Dentofacial Orthopedics · Cleft Lip and Palate Research
Introduction
1
Edentulism negatively impacts a patient's life by impairing psychosocial functioning, nutrition, and overall health and diminishing quality of life (Felton 2009). This challenge is even greater in the maxilla due to the high aesthetic demands (Busenlechner et al. 2016).
Patients with maxillary hopeless residual dentition who are to be rehabilitated with implants and implant‐supported restorations often face difficulties and express concerns about the post‐extraction process (Cordaro et al. 2010) and the management of the provisional phase until their definitive prosthetic restoration (Busenlechner et al. 2016). One crucial decision in this context is the timing of implant placement after teeth extraction.
The traditional two‐stage protocol involves waiting 3–6 months after tooth extraction before implant placement (Brånemark et al. 1977; Adell et al. 1981). To shorten treatment time, early and immediate implant placement protocols have been proposed. Early implant placement occurs 4–8 weeks after extraction, following most soft‐tissue healing but before complete bone maturation. Immediate implant placement takes place at the time of extraction or within 10 days (Tonetti et al. 2019). The choice of the protocol should be made before tooth extraction, based on a careful analysis of factors such as bone volume, the integrity of the socket, the presence of infection, and hard‐ and soft‐tissue defects. Additionally, patient‐specific factors, such as smoking habits, should be considered (Tonetti et al. 2019). High survival and similar failure rates have been observed for implants placed at different times in the fully edentulous maxilla (Covani et al. 2012; Ciabattoni et al. 2017).
Traditional outcome measures, such as marginal bone levels, peri‐implant clinical parameters, and the survival of implants and prostheses, have limitations due to their focus on biological and mechanical aspects, which do not reflect the patient's perspective (De Bruyn et al. 2015). Consequently, the scientific community has recently shifted towards incorporating patient‐reported outcome measures (PROMs) and clinician‐reported outcome measures (CROMs) (Powers et al. 2017; Yu et al. 2023). Patient‐reported outcomes (PROs) refer to the actual health outcomes as experienced by patients, such as pain, quality of life, or satisfaction. PROMs are the structured tools, like questionnaires or scales, that capture these PROs directly from patients, without any alterations or interpretations by clinicians or others, ensuring a standardized assessment of the patient's perspective (Weldring and Smith 2013; FDA Glossary 2018). In contrast, clinician‐reported outcomes (ClinROs) are derived from evaluations made by healthcare professionals based on clinical observations and objective tests, requiring specialized training to accurately interpret signs, behaviors, or other manifestations related to a condition (FDA Glossary 2018). CROMs include reports of specific clinical findings or events and/or the use of rating scales (FDA Glossary 2018).
Recently, the ID‐COSM project established a minimum core outcome set to standardize research in implant dentistry, identifying essential domains for clinical studies in this field. This project, along with its supporting systematic reviews, highlighted four core areas—pathophysiology, lifespan, life impact, and access to care‐health economics—and defined 11 mandatory outcome domains that should be included in the protocol and reporting of clinical trials in implant dentistry (Tonetti et al. 2023). However, while ID‐COSM provides valuable guidance on essential outcomes, particularly traditional ones, it does not specify which PROMs and CROMs should be used in specific clinical scenarios. Additionally, it does not provide guidance on the specific tools, methods of aggregation, analysis metrics, or ideal time points for assessing these outcomes and the interpretation and reporting of results.
There is a growing trend to analyze PROMs and CROMs alongside traditional metrics in implant dentistry for a more comprehensive evaluation (De Bruyn et al. 2015; Messias et al. 2023), and this shift highlights the need for standardizing these outcomes (De Bruyn et al. 2015; Souza et al. 2023; Messias et al. 2023). Consistent methodologies are essential to ensure that findings are comparable and valuable for clinical decision‐making. The rationale for this review is the necessity of harmonization in PROMs and CROMs reporting in clinical studies concerning the timing of implant placement in the edentulous maxilla.
The systematic review aims to identify, categorize, and summarize the PROs, PROMs, ClinROs, CROMs, and methods used in these studies over the past 10 years, allowing for the establishment of consistent outcomes and methodologies for future research in this clinical scenario, which in turn will facilitate the development of a core outcome set.
Materials and Methods
2
Protocol and Registration
2.1
The protocol for this systematic review was registered at PROSPERO (CRD42024519353). This review was reported in accordance with the guidelines of the Preferred Reporting Items for Systematic Review and Meta‐Analyses (PRISMA 2020; Page et al. 2021). This systematic review was commissioned by the Consensus Committee of the 1st Global Consensus for Clinical Guidelines and conducted in accordance with its established guidelines.
Focused Questions and PICOS Outline
2.2
Question 1
2.2.1
(1) In patients in need of full rehabilitation of the maxillary arch with dental implant therapy according to different implant placement timing protocols, what PROs and ClinROs have been reported?
Question 2
2.2.2
(2) In patients in need of full rehabilitation of the maxillary arch with dental implant therapy according to different implant placement timing protocols, what measures PROMs and CROMs have been employed to assess PROs and ClinROs?
Although the present review addresses two focused questions, they explore complementary aspects of the same population, intervention, and outcomes: Question 1 focuses on the identification of reported PROs and ClinROs, while Question 2 addresses the measures used to assess these outcomes (PROs and ClinROs).
PIOS Outline
2.2.3
- Population (P): Patients with an edentulous maxilla or those with residual dentition scheduled for extraction and in need of an implant‐supported prosthesis.
- Intervention (I): Implant therapy, including immediate implant placement at the time of tooth extraction and subsequent placements at various stages of healing: early soft‐tissue healing [4–8 weeks post‐extraction], partial bone healing [3–4 months post‐extraction], delayed implant placement [more than 4 months post‐extraction] and following alveolar ridge preservation [within 4–8 weeks or 3–4 months after the alveolar ridge preservation procedure].
- Outcomes (O): Primary outcomes: PROs/PROMs; Secondary outcomes: ClinROs/CROMs.
- Study (S): Prospective interventional and observational studies.
Eligibility Criteria
2.3
Inclusion Criteria
2.3.1
- Studies clearly reporting the time of implant placement after tooth extraction, regardless of the presence of a comparative group.
- Prospective interventional and observational studies (e.g., randomized controlled trials, non‐randomized controlled trials, cohort studies, case series with at least 10 cases) to capture a comprehensive range of PROMs and CROMs from both controlled and observational contexts.
- Patients with a completely edentulous maxilla or those scheduled for all maxillary teeth extraction who will receive implants and complete‐arch implant‐supported prostheses.
- Studies evaluating both PROs/PROMs and/or ClinROs/CROMs.
- Studies published within the past 10 years (from 2014 to present) focus on recent practices, in alignment with the guidance provided by the consensus committee that commissioned this review.
- Studies in the English language to promote consistency in data extraction and analysis, as it is the predominant language in this field.
Exclusion Criteria
2.3.2
- Retrospective studies, cross‐sectional studies, case reports, in vitro, and preclinical studies.
- Studies involving implants that had already been placed prior to the study initiation.
- Studies involving implants placed in the pterygoid or zygomatic bones.
Search Methods
2.4
The electronic databases searched between April 27 and May 17, 2024, included the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (PubMed), and SCOPUS. Additionally, the bibliographies of the included articles were manually searched. Search results from all databases were then combined, and duplicates were removed. The detailed search strategies are listed in Table S1.
Study Selection and Data Collection
2.5
After searching the mentioned electronic databases, the retrieved articles underwent a three‐phase screening process independently conducted by two authors (I.N.R.R. and M.A.H.). Initially, the Rayyan platform (Ouzzani et al. 2016) was used to select titles and abstracts based on the eligibility criteria. Articles that appeared to meet the inclusion criteria or those with insufficient information in the titles and abstracts for a clear decision were chosen for full manuscript evaluation. Subsequently, the full‐text versions of these studies were reviewed. Studies meeting all selection criteria proceeded to data extraction. To ensure consistency, reviewers participated in initial calibration sessions and held periodic meetings after every 100 articles to resolve discrepancies and align methods. Reviewer agreement was measured using the Kappa coefficient. Disagreements were resolved through discussion and consensus, with a third reviewer (C.M.P.) providing arbitration if necessary.
The data extraction included the first author's name, year of publication, country, setting (university or private practice), study design, number of arms, funding, number of patients, sex, mean age, study's maximum follow‐up, primary outcome, timing of implant placement, timing of loading, whether the implants were placed in the maxilla or both the maxilla and mandible, number of implants, number of implants per patient, implant type (e.g., standard implants vs. mini‐dental implants), and type of prosthesis (fixed or removable). For PROs and ClinROs, specific measure (PROMs/CROMs) and methods, interpretation, analysis metrics, method of aggregation, and time points were collected (FDA Glossary 2018; Hopewell et al. 2025).
Risk of Bias
2.6
The risk of bias in the included randomized controlled trial was assessed in duplicate by two authors (I.N.R.R. and M.A.H.) as part of the data extraction process, using version 2 of the Cochrane risk‐of‐bias tool (RoB2) for randomized trials (Sterne et al. 2019). Quality assessment of the included case series was done according to the guidelines of the Joanna Briggs Institute (JBI) checklist for case series (Martin 2017).
Data Synthesis
2.7
The outcomes for each of the two focused questions were described in detail and analyzed using STATA version 16.1 (StataCorp, College Station, TX, USA). PROMs and CROMs were presented separately. Descriptive statistics, including numbers and percentages, were applied to summarize the frequency distribution of assessed outcomes and measurements. Within each category, similar outcomes were grouped, and tables were constructed to display key information.
Results
3
Search and Screening
3.1
The flowchart of the entire selection process is reported in Figure 1. The literature search resulted in 2560 titles. After the exclusion of duplicates, 1014 titles were screened, out of which 56 potentially relevant articles were selected. Following full‐text reading, 43 articles were excluded, and 13 fulfilled the eligibility criteria and were used for data extraction. Inter‐rater reliability, quantified by the Kappa statistic, was 0.83 for the title and abstract screening stage and 1.00 for the full‐text review. The reasons for exclusion are presented in Table S2.
Flowchart with detailed selection process.
General Characteristics of the Included Studies
3.2
Out of the 13 included studies, 1 was an RCT (Menini et al. 2016), and 12 were case series (Yamada et al. 2015; Misumi et al. 2015; Fürhauser et al. 2016; Zhang et al. 2016; Erkapers et al. 2017; Boven et al. 2017; Zembic et al. 2019; Fonteyne et al. 2019; Van Doorne et al. 2020; Testori et al. 2021; Pomares‐Puig et al. 2023; Bouhy et al. 2023). The studies were performed in Belgium (Fonteyne et al. 2019; Van Doorne et al. 2020; Bouhy et al. 2023), the Netherlands (Boven et al. 2017; Zembic et al. 2019), the United States and Sweden (Erkapers et al. 2017), Austria (Fürhauser et al. 2016), Italy (Menini et al. 2016; Testori et al. 2021), Japan (Yamada et al. 2015; Misumi et al. 2015), Spain (Pomares‐Puig et al. 2023), and China (Zhang et al. 2016). The study's maximum follow‐up ranged from 48 h after implant placement (Menini et al. 2016) to 10 years (Zhang et al. 2016; Table 1).
The number of included patients ranged from 10 (Testori et al. 2021; Pomares‐Puig et al. 2023) to 51 (Erkapers et al. 2017). The patients' mean age ranged from 56 (Yamada et al. 2015) to 71.10 years (Testori et al. 2021). The primary outcome was reported in 5 (Misumi et al. 2015; Menini et al. 2016; Erkapers et al. 2017; Pomares‐Puig et al. 2023; Bouhy et al. 2023) out of 13 studies. PROMs were the primary outcomes in two studies (Misumi et al. 2015; Erkapers et al. 2017; Table 1).
The number of implants ranged from 42 (Zembic et al. 2019) to 306 (Erkapers et al. 2017). The number of implants per patient ranged from 2 (Zembic et al. 2019) to 8 (Zhang et al. 2016; Pomares‐Puig et al. 2023). The timing of implant placement was delayed in 9 studies (Yamada et al. 2015; Misumi et al. 2015; Zhang et al. 2016; Erkapers et al. 2017; Boven et al. 2017; Zembic et al. 2019; Fonteyne et al. 2019; Van Doorne et al. 2020; Bouhy et al. 2023), immediate in two studies (Fürhauser et al. 2016; Pomares‐Puig et al. 2023), and two studies performed both protocols, delayed and immediate implants (Menini et al. 2016; Pomares‐Puig et al. 2023). In eight studies, the implants were placed only in the maxilla (Yamada et al. 2015; Zhang et al. 2016; Erkapers et al. 2017; Boven et al. 2017; Zembic et al. 2019; Fonteyne et al. 2019; Van Doorne et al. 2020; Bouhy et al. 2023); in one study, the implants were installed in the maxilla or maxilla and mandible (Misumi et al. 2015), and in three studies, the implants were installed in the maxilla and mandible (Menini et al. 2016; Testori et al. 2021; Pomares‐Puig et al. 2023; Table 2).
Eleven studies used standard implants (Yamada et al. 2015; Misumi et al. 2015; Fürhauser et al. 2016; Menini et al. 2016; Zhang et al. 2016; Erkapers et al. 2017; Boven et al. 2017; Zembic et al. 2019; Testori et al. 2021; Pomares‐Puig et al. 2023; Bouhy et al. 2023), and two used mini‐dental implants (Fonteyne et al. 2019; Van Doorne et al. 2020). Five studies used removable prostheses (Boven et al. 2017; Zembic et al. 2019; Fonteyne et al. 2019; Van Doorne et al. 2020; Bouhy et al. 2023), and eight studies used fixed prostheses (Yamada et al. 2015; Misumi et al. 2015; Fürhauser et al. 2016; Menini et al. 2016; Zhang et al. 2016; Erkapers et al. 2017; Testori et al. 2021; Pomares‐Puig et al. 2023; Table 2).
Due to the variety of outcomes and measurements, results were organized into PROs/PROMs and ClinROs/CROMs, detailing the outcomes and their respective assessment methods.
Risk of Bias
3.3
The randomized controlled trial was categorized as having some concerns according to the RoB2 tool (Menini et al. 2016). These concerns stemmed from the lack of information regarding allocation sequence concealment (Domain 1) and the absence of a registered protocol (Domain 5; Figure 2).
Risk of bias assessment of the included RCT.
For the 12‐case series, quality assessment using the JBI 10‐point checklist revealed a mean quality score of 7.5. One case series received the highest score (10/10) (Bouhy et al. 2023), 6 received 8/10 (Yamada et al. 2015; Boven et al. 2017; Zembic et al. 2019; Fonteyne et al. 2019; Van Doorne et al. 2020; Pomares‐Puig et al. 2023), 2 received 7/10 (Fürhauser et al. 2016; Testori et al. 2021), and 3 received 6/10 (Misumi et al. 2015; Zhang et al. 2016; Erkapers et al. 2017). The highest‐scoring criteria were clearly describing the patient's demographic characteristics (12/12) and site/clinic demographic information (11/12). The lowest scores were for complete inclusion of participants (7/12), clear reporting of outcomes or follow‐up results (7/12), and clear reporting of clinical information of the participants (5/12; Figure 3).
Methodological quality assessment of the included case series.
PROs and PROMs
3.4
The following domains or key aspects were analyzed using respective methods, ordered by frequency of assessment:
- Oral health‐related quality of life, encompassing the domains of functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap, was evaluated in 7 out of 13 studies, accounting for 53.85% of the total studies reviewed. This assessment used various versions of the Oral Health Impact Profile (OHIP):
- OHIP‐14 (14‐item questionnaire) and its variant OHIP‐J14 were applied in 3 studies, constituting 23.08% (Misumi et al. 2015; Fonteyne et al. 2019; Pomares‐Puig et al. 2023).
- OHIP‐20 or OHIP‐EDENT (20‐item questionnaire) was employed in 2 studies, representing 15.38% of the total (Zembic et al. 2019; Bouhy et al. 2023).
- OHIP‐49 (49‐item questionnaire) was used in 1 study, accounting for 7.69% (Erkapers et al. 2017).
- The OHIP‐J49 (54‐item questionnaire, which includes additional Japanese‐specific questions) was used in 1 study, representing 7.69% (Yamada et al. 2015).
- Pain intensity was analyzed in 5 out of 13 studies, accounting for 38.46% of the total studies reviewed. This was assessed using:
- Postoperative pain, using a 0–100 mm VAS in 2 studies, representing 15.38% (Yamada et al. 2015; Pomares‐Puig et al. 2023).
- Postoperative pain, using a 10 cm VAS in 1 study, representing 7.69% (Fürhauser et al. 2016).
- Postoperative pain, using a verbal rating scale (VRS) with six levels (categories) in 1 study, represents 7.69% (Menini et al. 2016).
- Postoperative pain, using a numeric rating scale (NRS) from 1 to 10 and after, classified according to scores in 1 study, representing 7.69% (Van Doorne et al. 2020).
- Intraoperative pain, using a 0–100 mm VAS in 1 study, represents 7.69% (Pomares‐Puig et al. 2023).
- Patient satisfaction with the prosthesis was analyzed in 3 out of 13 studies, accounting for 23.08% of the total studies reviewed. This was assessed using
- A 100 mm visual analog scale (VAS) in 2 studies, representing 15.38% of the total (Zembic et al. 2019; Bouhy et al. 2023).
- A questionnaire with multiple‐choice options (categories) in 1 study, representing 7.69% of the total (Zhang et al. 2016).
- Postoperative drug administration was analyzed in 2 out of 13 studies, representing 15.38%, by recording postoperative drug use (Menini et al. 2016; Pomares‐Puig et al. 2023).
- Patient overall satisfaction with the treatment was analyzed in 1 study (7.69%), using a 10‐point rating scale (Boven et al. 2017).
- Overall satisfaction with oral health was analyzed in 1 study (7.69%), using a 10 cm VAS (Fonteyne et al. 2019).
- Patient well‐being during the surgical procedure was assessed in 1 study (7.69%), using a questionnaire with a Likert scale ranging from −2 to 2 (Pomares‐Puig et al. 2023).
- Satisfaction during the surgery was assessed in 1 study (7.69%), using a 0–100 mm VAS (Pomares‐Puig et al. 2023).
- Psychosocial impact (comfort) using a device dedicated to managing postoperative swelling and pain was analyzed in 1 study (7.69%), using a numerical rating scale (NRS) from 0 to 10 (Menini et al. 2016).
- Postoperative impairment of everyday life and work was analyzed in 1 study (7.69%) using a 10 cm VAS (Fürhauser et al. 2016).
- Postsurgical quality of life was assessed in 1 study (7.69%), using a questionnaire with multiple‐choice options, scored from 0 to 10 (Testori et al. 2021).
- Postprosthetic quality of life was assessed in 1 study (7.69%), using a questionnaire with multiple‐choice options, scored from 0 to 10 (Testori et al. 2021).
- Functional complaints about the prosthesis were analysed in 1 study (7.69%), using a 7‐item questionnaire with a four‐point rating scale with multiple‐choice options (scores; Boven et al. 2017).
- Patient's eating ability was analyzed in 1 study (7.69%), using a questionnaire with multiple‐choice options (scores; Boven et al. 2017).
- Speech measured by one OHIP‐14 question from the domain “functional limitation” was analysed in 1 study (7.69%; Fonteyne et al. 2019).
- Satisfaction with speech was analyzed in 1 study (7.69%), using a 10 cm VAS (Fonteyne et al. 2019).
PROs related to the immediate postoperative period (up to 1 week) were consistently evaluated in studies with immediate implant placement. However, similar outcomes were also reported in studies with delayed implant placement.
Further details on the PROs and PROMs are provided in Table 3, while references for the methods cited in the respective studies, along with information on validation, can be found in Table S3.
ClinROs and CROMs
3.5
Ten of the included studies assessed ClinROs. The following domains or key aspects were evaluated using respective methods, listed in order of their frequency of assessment:
- Implant survival was reported in five studies (27.8%), defined as the clinical presence of the implant without signs of mobility (Boven et al. 2017; Van Doorne et al. 2020; Testori et al. 2021; Bouhy et al. 2023) or, in addition to the aforementioned criteria, the absence of discomfort, symptoms of neurologic problems, or signs of peri‐implantitis (Yamada et al. 2015).
- Prosthetic complications were reported in four studies (22.2%), including abutment loosening, prosthesis misfit, veneer chipping, fractures, screw loosening, significant wear, loss, or wear of the matrix component (in overdentures), need for prosthesis modification, and others (Yamada et al. 2015; Zhang et al. 2016; Erkapers et al. 2017; Bouhy et al. 2023).
- Prosthetic survival was reported in three studies (16.7%), defined as a prosthesis in function without the need for replacement (Yamada et al. 2015; Van Doorne et al. 2020; Testori et al. 2021).
- Peri‐implant bone level changes—marginal bone loss was reported in three studies (16.7%), assessed using standardized intraoral radiographs (Yamada et al. 2015; Zhang et al. 2016) and panoramic radiographs (Boven et al. 2017).
- Probing depth was reported in three studies (16.7%), measured at multiple sites per implant using calibrated periodontal probes (Zhang et al. 2016; Boven et al. 2017; Bouhy et al. 2023).
- Modified plaque index or plaque index was reported in three studies, scored from 0 to 3 according to established criteria (16.7%) (Zhang et al. 2016; Boven et al. 2017; Bouhy et al. 2023).
- Sulcular Modified Bleeding Index was reported in three studies (16.7%), scored from 0 to 3 according to established criteria (Zhang et al. 2016; Boven et al. 2017; Bouhy et al. 2023).
- Swelling was analyzed in two studies (11.1%), using standardized frontal and side images, comparing presurgery and postsurgery conditions, and classified into categories (Menini et al. 2016). The other study analyzed swelling clinically through a questionnaire and classified it into categories (Yamada et al. 2015).
- Presence of calculus was reported in one study (5.6%), recorded dichotomously (present/absent; Boven et al. 2017).
- Gingival index (peri‐implant inflammation) was reported in 1 study (5.6%), scored 0–3 based on clinical inflammation severity (Boven et al. 2017).
- Peri‐implantitis was reported in 1 study (5.6%), defined as bone loss > 3 mm with bleeding or suppuration (Zhang et al. 2016).
- Accepted prosthodontic maintenance events were analyzed clinically in one study (5.6%), defined as no more than two replacements of patrices, matrices, or matrix components in the first year and no more than five in 5 years (Bouhy et al. 2023).
- Prosthesis failure, defined as more than two repeated fractures of the overdenture necessitating metallic reinforcement, was analyzed clinically in one study (5.6%; Bouhy et al. 2023).
- Articulation was analyzed clinically in one study (5.6%), using a picture naming test of images covering sounds. Digitally recorded samples were rated by two speech‐language therapists (Fonteyne et al. 2019).
- Oromyofunctional behavior was analysed clinically in one study (5.6%), including analysis of the tongue, jaw, lip, and facial muscle movements, as well as blowing and whistling. A questionnaire checked for sucking habits, mouth breathing, lip incompetence, drooling, nail‐biting, and bruxism (Fonteyne et al. 2019).
- Accuracy of implant positioning was reported in one study (5.6%), based on CBCT‐measured deviation (2D, 3D, angular; Pomares‐Puig et al. 2023).
- Insertion torque was reported in one study (5.6%), measured using an implant insertion micromotor (Yamada et al. 2015).
- Surgical time was reported in one study (5.6%), registered during the surgery for implant placement (Yamada et al. 2015).
Additional information on the ClinROs and CROMs is presented in Table 4, with references for the methods cited in the respective studies found in Table S3.
Discussion
4
Main Findings
4.1
The aim of the present systematic review was to assess the outcomes and measures used to analyze PROs and ClinROs in prospective clinical studies focusing on the timing of implant placement in fully edentulous maxilla or maxilla with residual dentition scheduled for extraction and requiring implant‐supported prosthesis. The review shows a wide array of PROs (16) and ClinROs (18) used across the 13 included studies, with varying assessment tools and methods. While this diversity demonstrates the tailored nature of outcome measures, it also underscores the importance of harmonizing core outcomes to improve comparability and consistency across studies, which is an essential step in developing a core outcome set (Williamson et al. 2017; Kirkham et al. 2017). Regardless of the timing of implant placement, no clear trend emerged in terms of the outcomes assessed and the analysis methods employed, indicating variability across studies.
The organization of the results in this study was adapted following data extraction due to substantial heterogeneity in the outcomes and measurement methods encountered, which were categorized into PROs/PROMs and ClinROs/CROMs.
PROs and PROMs
4.2
The PROs in the included studies covered various aspects of patient experience, such as treatment impact on quality of life and satisfaction with treatment and oral health. They also assessed surgery‐related outcomes, including pain intensity, postoperative drug use, everyday life impairment, patient well‐being, and comfort. Additionally, outcomes related to implant‐supported prostheses, such as satisfaction, functional complaints, and masticatory function, were evaluated. Within each of these main areas, the outcomes and assessment methods varied significantly.
Some studies focused on specific aspects such as speech, eating ability, and psychosocial impact, while others provided a more general assessment of quality of life and satisfaction. This variety reflects the comprehensive nature of PROs but also points to the need for a consensus on essential PROs (Williamson et al. 2017). Establishing a minimum core outcome set would ensure that key PROMs are consistently included in trials within this area, facilitating more standardized and comparable results (Kirkham et al. 2017).
Oral health‐related quality of life was the most assessed outcome of PROMs. Different versions of the Oral Health Impact Profile (OHIP) were used for this purpose, including OHIP‐14, OHIP‐20, OHIP‐49, and OHIP‐J49. OHIP‐49, with its 49 items, is the original and most comprehensive version, covering a wide range of issues related to oral health and its impact on quality of life (Slade and Spencer 1994). It offers in‐depth insight into the seven domains (functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap; Slade and Spencer 1994), but can be time‐consuming to administer. The OHIP‐14 was the most used instrument in the included studies. Comprising 14 items, it is a highly abbreviated version of the OHIP‐49, focusing on the most critical aspects of oral health‐related quality of life (Slade 1997). It retains the seven original domains but only two items per domain, making it quick to administer but potentially less comprehensive. However, OHIP‐14 may have compromised measurement properties for edentulous patients due to the exclusion of items related to chewing and denture‐wearing during its development (Locker et al. 2001; Allen and Locker 2002). Additionally, it may experience floor effects, where many participants score at the lower end of the scale (Bindman et al. 1990). This occurs because the instrument lacks sensitivity at the lower end, often due to the exclusion of relevant items (Locker et al. 2001; Allen and Locker 2002). As a result, it can underestimate the true extent of issues or changes in edentulous patients' oral health status. In contrast, OHIP‐20, dedicated to edentulous patients, includes questions on chewing difficulty, food catching, denture fitting, and others, addressing specific needs (Allen and Locker 2002). Standardizing certain OHIP versions is important, as using different versions across studies complicates result comparison.
VAS, NRS, and VRS were frequently used to measure pain intensity. The VAS is statistically robust and provides ratio‐level data, but it is the most challenging to use and has the highest failure rate (Williamson and Hoggart 2005; Karcioglu et al. 2018). Elderly patients and individuals with cognitive impairments and communication difficulties often found verbal descriptors or rating scales more practical for expressing pain intensity (Karcioglu et al. 2018). Both the VAS and NRS are highly sensitive in detecting changes in pain levels. The NRS offers interval‐level data, is easy to administer, and is more suitable for pain assessment, audits, and research. Although the VRS is the least sensitive, it is the simplest to use (Williamson and Hoggart 2005; Karcioglu et al. 2018). However, all three scales are valid, reliable, and appropriate for clinical practice (Williamson and Hoggart 2005; Karcioglu et al. 2018). Despite their validity and reliability, the specific implementations of these scales varied, leading to inconsistent reporting. Additionally, there was significant variation in the interpretation of the results, with different studies using varying levels, categories, and thresholds. Methods of reporting also differed, with some studies presenting the variables as categories and frequencies while others used continuous variables.
Patient satisfaction was also evaluated in the included studies, and VAS was the most used tool. Measuring patient satisfaction is challenging due to its complex definition and the influence of confounders, which can be patient‐ or measurement‐related (Voutilainen et al. 2016). Despite its limitations, the VAS is sensitive and appropriate for this measurement. It demonstrates reduced susceptibility to the ceiling effect, which occurs when respondents frequently achieve the highest possible score, limiting the scale's ability to capture the full range of variability (Voutilainen et al. 2016).
The most common baseline for evaluating PROs was before implant placement. However, subsequent time points varied depending on the outcomes, even for the same outcomes. For oral health‐related quality of life using different OHIP questionnaires, the second evaluation ranged from 1 week to 1 year after surgery. Pain was analyzed intraoperatively (immediately after surgery) and postoperatively (within the first 2 days or 1 week after surgery). Patient satisfaction was primarily assessed before implant placement, with follow‐up periods ranging from the time of provisional prosthesis delivery (1 week after surgery) to 5 years after implant placement. This variability in follow‐up times can challenge the analysis and interpretation of PROs, potentially affecting the consistency and comparability of the results.
Clear differences were observed not only in the selected outcomes but also in the assessment tools and timing used for similar PROs. This variability hinders result comparisons across studies and underscores the need for standardized PROs in implant dentistry. Diverse tools and methods for assessing and interpreting similar outcomes challenge meaningful comparisons and data synthesis. This heterogeneity leads to inconsistencies in reported outcomes, making it difficult to identify the most effective clinical practices from the patient's perspective.
ClinROs and CROMs
4.3
Ten of the included studies assessed ClinROs, encompassing a broad range of clinical outcomes, including traditional clinical parameters on peri‐implant health and implant stability, surgical parameters, function, and prosthetic performance. ClinROs also exhibited considerable variability in the methods and domains assessed.
The most frequently reported were implant survival and prosthetic complications. Implant survival was evaluated in five studies, generally defined as the implant being in place without mobility, with one study also requiring the absence of discomfort, pain, or neurologic symptoms. Although this outcome is fundamental in implant dentistry, heterogeneity in its definition and the lack of standardized follow‐up protocols may hinder direct comparisons (Papaspyridakos et al. 2012). Prosthetic complications and prosthetic survival were the second most commonly reported ClinROs, covering a wide spectrum of mechanical and technical issues. Inconsistent categorization and varying definitions for what constitutes a “complication” across studies pose challenges for synthesis (Papaspyridakos et al. 2012).
Other traditional ClinROs, such as peri‐implant bone level changes, probing depth, plaque accumulation, presence of calculus, and bleeding indices, were also reported. These are indicators of peri‐implant health and implant stability. However, differences in radiographic methods (e.g., standardized intraoral vs. panoramic imaging; Dos Reis et al. 2025), clinical techniques (e.g., probe type and measurement method; Monje and Salvi 2024), and data aggregation and reporting approaches may affect measurement accuracy and comparability.
Peri‐implantitis incidence was assessed in one study. As a composite outcome, it requires standardized diagnostic parameters to enable consistent and comparable incidence estimates across studies. In this sense, the case definitions for peri‐implant diseases should follow those established in the 2017 World Workshop (Berglundh et al. 2018; Tonetti et al. 2023).
The accuracy of implant positioning, assessed via CBCT superimposition, was reported in one study involving immediate implant placement and loading (Pomares‐Puig et al. 2023), highlighting a gap in the literature regarding the precision of surgical execution in such cases.
Insertion torque and surgical time, two intraoperative outcomes, were reported in one study (Yamada et al. 2015). Insertion torque reflects primary implant stability and is influenced mainly by implant design and bone quality (Hadaya et al. 2022). Surgical time provides an indirect measure of procedural complexity and operator efficiency. While both are valuable for intraoperative assessment, they remain underreported.
Finally, the inclusion of outcomes such as articulation, oromyofunctional behavior, and swelling reflects an effort to capture broader functional aspects of rehabilitation. However, these outcomes were rarely reported, and typically by single studies. Future studies should also focus on these outcomes, as the clinician's subjective perspective is crucial in defining the success of implant procedures and guiding treatment plans and interventions. Moreover, ClinROs can complement PROs by offering a clinical perspective that balances the patient's subjective experiences (Powers et al. 2017).
Postsurgical swelling was assessed in two of the four studies using standardized frontal and side images and a clinical examination using questionnaires, both classifying swelling into categories. While swelling is an important indicator of postoperative inflammation (Antonelli et al. 2023), the heterogeneity in assessment methods (images vs. questionnaires) impairs comparability across studies.
The ClinROs related to the prosthesis were derived from one study, which defined criteria for acceptable prosthodontic maintenance events, prosthetic complications, and prosthesis failure. These criteria provide a framework for evaluating the long‐term success and durability of implant‐supported prostheses. By establishing clear thresholds for acceptable maintenance and complications, clinicians can better manage patient expectations and improve treatment planning. This focus is also crucial because frequent interventions can lead to increased patient discomfort, higher costs, and reduced overall satisfaction (Karimbux et al. 2023). However, more comprehensive research and validation of these criteria are needed, as they currently rely on a single study. A clear and standardized definition for complications and failures for both prostheses and implants would be beneficial for future studies (Papaspyridakos et al. 2012).
Regarding articulation and oromyofunctional behavior, both outcomes were assessed in one study. Articulation, speech clarity, and quality are relevant aspects of patient quality of life (Allen et al. 2001). Oromyofunctional behavior, a comprehensive evaluation that identifies issues like tongue thrust during swallowing and problems with jaw mobility, is important for ensuring proper oral function and comfort with implant‐supported prostheses (Fonteyne et al. 2019). Despite this, these outcomes were evaluated in only one of the included studies. Other studies have used these methods in different clinical contexts, not specifically for the rehabilitation of the fully edentulous maxilla with implant‐supported prostheses (Van Lierde et al. 2011, 2012).
Clear differences were observed in the selection and assessment of ClinROs, with notable variability in the methods, domains, and criteria applied across studies. Standardized clinical tests and objective measures were often lacking, with many studies relying on subjective clinician evaluations. This reliance can introduce bias and variability, limiting the comparability and reliability of findings (Powers et al. 2017).
Risk of Bias
4.4
The included randomized controlled trial showed risk of bias concerns due to two main issues: insufficient information on allocation sequence concealment and the lack of a registered protocol. Allocation sequence concealment prevents selection bias, and a registered protocol ensures transparency and accurate reporting. Without these, it is challenging to verify if the study was conducted and reported as intended (Spieth et al. 2016).
Regarding the included case series, the lowest scores were in three critical areas: complete inclusion of participants (Q5), clear reporting of clinical information (Q7), and outcomes or follow‐up results (Q8). These low scores indicate significant gaps in the transparency and completeness of the data presented (Martin 2017). The low score in Q5 suggests that not all eligible participants were included, potentially introducing selection bias. Poor reporting of clinical information (Q7) can obscure important details about the patient population and their treatment, which could influence the outcomes, including PROMs and CROMs. Inadequate reporting of outcomes or follow‐up results (Q8) hinders the ability to evaluate the effectiveness and long‐term outcomes (Mayo‐Wilson et al. 2017; Souza et al. 2023).
Comprehensive outcome reporting, ideally following the CONSORT guidelines (Schulz et al. 2010) and the five levels of outcome reporting as outlined in the SPIRIT statement (Chan et al. 2013; Calvert et al. 2018), is essential for accurately evaluating the success and durability of interventions. An outcome is fully defined when it encompasses five levels: (1) domain, (2) specific measure, (3) specific metric, (4) aggregation method, and (5) time point. Incomplete specification of outcomes in the protocol or publication can lead to selective reporting, where authors may choose measures, metrics, and time points that yield statistically significant results (Mayo‐Wilson et al. 2017; Souza et al. 2023).
Strengths and Limitations
4.5
Some limitations of this review should be considered. When applying all the eligibility criteria, no comparative studies regarding the timing of implant placement in the maxilla were found. As a result, this topic was not the primary focus of the included studies, most of which were single‐arm studies. Additionally, the review was limited to manuscripts published in English. Restricting the review to manuscripts published in English aimed to maintain consistency in reporting and interpretation, though it resulted in the exclusion of one study published in another language (Table S2).
This review adopted the consensus definition of immediate implant placement, specifying it as occurring at the time of extraction or within 10 days (Tonetti et al. 2019). However, it is acknowledged that clinical outcomes and patient experiences associated may differ significantly between same‐day placement and placement occurring up to 10 days post‐extraction. An alternative, perhaps more contextually appropriate definition describes immediate implant placement as performed immediately after tooth extraction within the same surgical procedure (Chen et al. 2004; Hämmerle et al. 2004; Gallucci et al. 2018). Notably, all studies included in this review that adhere to an immediate protocol involved implant placement during the same surgical procedure as the extraction. These timing variations may impact PROs/PROMs and ClinROs/CROMs, such as pain and swelling, and should therefore be carefully considered when selecting outcomes to be assessed.
Different loading protocols (immediate, early, or delayed) may also influence PROs/PROMs and ClinROs/CROMs, and information on loading timing has been provided for each study to offer context (Gallucci et al. 2018). However, this review specifically addresses outcomes related to implant placement timing, while a separate systematic review assessed outcomes associated with implant loading timing.
Additionally, although bone augmentation was performed in a subset of patients in four of the included studies, its specific impact on PROs/PROMs and ClinROs/CROMs was not evaluated.
The strengths of this review include the diverse range of outcomes identified and the comprehensive search strategy implemented, covering five major databases along with detailed hand searching. The data from this systematic review can be used for the establishment of a core outcome set in the field of rehabilitation of maxillary edentulous patients. Rather than evaluating the effectiveness of individual outcomes, this review aims to identify existing tools and facilitate an evidence‐based consensus process to guide the selection of standardized outcomes for future studies.
Future Perspectives
4.6
For future research, integrating both PROs and ClinROs should be considered for a comprehensive understanding of treatment efficacy and patient satisfaction (Kirkham et al. 2017). Developing a core set of PROMs and CROMs should be a priority to improve the selection and reporting of these outcomes, enhancing the comparability and utility of findings, and making them more actionable for clinical practice (Kirkham et al. 2017).
Moreover, it is important to consistently report contextual factors of the treatment that may influence PROs, such as whether treatments are provided under subsidized or research‐based settings, which may or may not cover patient costs. Treatment expenses and the perceived cost‐effectiveness can influence patient perceptions and subsequently affect reported outcomes (Dean et al. 2021; Bianchim et al. 2023). Additional biases in PROs can arise when perceived satisfaction is influenced more by the treatment setting than by clinical outcomes alone. Influential factors include patient‐related influences (like trust in the professional team, social desirability, and expectations shaped by pre‐treatment counseling or awareness of other patient outcomes) and treatment‐specific effects (such as the innovative nature of the treatment and placebo responses). To mitigate these biases, future studies should employ strategies like blinding patients to intervention type, center, and professional reputation; using control groups, and assessing baseline expectations. Consistently reporting these fundamental characteristics will enhance the interpretability and comparability of PROs across diverse treatment settings (Roydhouse et al. 2019; Kluzek et al. 2022).
It is essential to emphasize that PROMs should be validated for the specific conditions and outcomes they are intended to measure. These instruments can be either general or condition‐specific. General PROMs assess broad aspects related to a variety of health conditions, but they may lack sensitivity to detect the specific symptoms of a condition, such as complete edentulism, which could influence treatment options and outcomes. In contrast, condition‐specific instruments are designed to focus on particular symptoms and their impact on the patient's health, making them more capable of detecting and quantifying specific symptoms both cross‐sectionally and over time related to that condition (Leles et al. 2022; Needleman et al. 2023).
In the context of implant treatment for complete edentulism in the maxilla, the instruments should be adapted and validated for this unique clinical scenario. This differs from assessing partial tooth loss or areas generally considered to have less aesthetic relevance in this context, such as the mandible. Therefore, PROMs must account for the clinical characteristics of edentulous patients and the effects of different treatment options, such as dental implants. The use of validated instruments specifically designed for this context would allow for a more precise assessment of patient outcomes. There should be a preference for using validated instruments that are tailored to the clinical context of interest, and further validation for implant placement specifically would enhance their applicability.
The validation of PROMs is a key process in ensuring their appropriateness for measuring the specific outcomes in a given context (McKenna 2011). As shown in Table S3, some studies conducted a formal validation process for the specific PROM, testing reliability, validity, and sensitivity, thereby confirming the tool's suitability for assessing the desired condition (i.e., OHIP‐14 for oral health‐related quality of life). However, in other cases, although the PROM was used in referenced studies, no formal validation was conducted. Instead, some studies relied on previous research where the PROM was adopted without specific validation. Additionally, there were instances where the PROM was used without any previous formal validation or reference to prior studies, suggesting the tool was applied based on the authors' judgment or adapted for the specific study. Beyond general PROM validation, a limited number of studies conducted validation specifically within the context of implant treatment. Therefore, the use of validated tools should be prioritized, ideally those specifically validated for the clinical context in which they will be applied, such as in implant treatments, as previously discussed.
The ID‐COSM project (Tonetti et al. 2023), grounded in previously performed systematic reviews, established a core outcome set for implant dentistry, focusing on essential outcome domains. However, it did not address specific PROs and ClinROs, measurement methods, or ideal assessment points for diverse clinical scenarios. The findings of the present review complement the ID‐COSM framework by providing groundwork for a future consensus aimed at defining these specific outcomes and measures, thereby enhancing consistency and precision in studies that will be planned and conducted in the future.
Conclusions
5
The PROs and ClinROs reported in the included studies exhibit substantial variability in domains, assessment methods, and reporting practices. These findings highlight the need for harmonization in outcome selection and the development of a core outcome set for PROs/PROMs and ClinROs/CROMs to enhance comparability and reliability across studies.
Author Contributions
Giuseppe A. Romito: conceptualization, writing – review and editing, project administration, writing – original draft, formal analysis. Isabella Neme Ribeiro dos Reis: investigation, writing – original draft, methodology, software, data curation, formal analysis, writing – review and editing. Mohamed A. Hassan: investigation, writing – original draft, writing – review and editing, methodology, software, formal analysis, data curation. Cristina Cunha Villar: writing – review and editing, supervision. Helena Francisco: writing – review and editing. Claudio Mendes Pannutti: conceptualization, writing – review and editing, methodology.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Table S1. Search strategies for each database.
Table S2. List of the excluded studies (N = 43).
Table S3. References for the methods used in the studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adell, R. , U. Lekholm , B. Rockler , and P. I. Brånemark . 1981. “A 15‐Year Study of Osseointegrated Implants in the Treatment of the Edentulous Jaw.” International Journal of Oral Surgery 10: 387–416.6809663 10.1016/s 0300-9785(81)80077-4 · doi ↗ · pubmed ↗
- 2Allen, F. , M. Anne , and W. David . 2001. “A Patient‐Based Assessment of Implant‐Stabilized and Conventional Complete Dentures.” Journal of Prosthetic Dentistry 85: 141–147.11208203 10.1067/mpr.2001.113214 · doi ↗ · pubmed ↗
- 3Allen, F. , and D. Locker . 2002. “A Modified Short Version of the Oral Health Impact Profile for Assessing Health‐Related Quality of Life in Edentulous Adults.” International Journal of Prosthodontics 15: 446–450.12375458 · pubmed ↗
- 4Antonelli, A. , S. Barone , F. Bennardo , and A. Giudice . 2023. “Three‐Dimensional Facial Swelling Evaluation of Pre‐Operative Single‐Dose of Prednisone in Third Molar Surgery: A Split‐Mouth Randomized Controlled Trial.” BMC Oral Health 23: 614.37653378 10.1186/s 12903-023-03334-y PMC 10468892 · doi ↗ · pubmed ↗
- 5Berglundh, T. , G. Armitage , M. G. Araujo , et al. 2018. “Peri‐Implant Diseases and Conditions: Consensus Report of Workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions.” Journal of Clinical Periodontology 45, no. Suppl 20: S 286–S 291.29926491 10.1111/jcpe.12957 · doi ↗ · pubmed ↗
- 6Bianchim, M. S. , E. Crane , A. Jones , et al. 2023. “The Implementation, Use and Impact of Patient Reported Outcome Measures in Value‐Based Healthcare Programmes: A Scoping Review.” P Lo S One 18: e 0290976.38055759 10.1371/journal.pone.0290976 PMC 10699630 · doi ↗ · pubmed ↗
- 7Bindman, A. B. , D. Keane , and N. Lurie . 1990. “Measuring Health Changes Among Severely Ill Patients. The Floor Phenomenon.” Medical Care 28: 1142–1152.2250498 10.1097/00005650-199012000-00003 · doi ↗ · pubmed ↗
- 8Bouhy, A. , M. Lamy , Y. Altaep , and F. Lambert . 2023. “Maxillary Implant Overdenture Retained by Four Unsplinted Attachments and Opposed by a Natural or Fixed Dentition: Five‐Year Clinical Outcomes. A Prospective Case Series.” Clinical Oral Implants Research 34: 285–296.36692949 10.1111/clr.14033 · doi ↗ · pubmed ↗