Knowledge and Awareness of Glaucoma: A Comparative Study Among Rural and Urban Patients in Bangladesh
Habiba Sultana, Khairul Islam, Md Sajidul Huq, Shajeda Azizi, Md Rezwanul Hasan

TL;DR
This study compares glaucoma awareness between rural and urban populations in Bangladesh, finding significantly lower knowledge in rural areas.
Contribution
The study provides new insights into the disparity of glaucoma awareness in rural versus urban Bangladesh, emphasizing the need for targeted education.
Findings
Only 20.8% of participants were aware of glaucoma, with urban participants slightly more informed than rural ones.
Rural participants had higher reported glaucoma history but lower knowledge of risk factors like optic nerve involvement.
Urban participants showed significantly better glaucoma knowledge, with 31.3% having excellent knowledge compared to 9.0% in rural areas.
Abstract
Background: Glaucoma is a leading cause of irreversible blindness worldwide and often progresses silently until significant vision loss occurs. Early detection and timely treatment are crucial to preventing visual impairment; however, these efforts largely depend on public awareness. Assessing glaucoma-related knowledge, particularly among underserved populations, is therefore essential for developing effective prevention and control strategies. This study aimed to assess and compare the level of knowledge and awareness of glaucoma among rural and urban patients. Methodology: This comparative study included a total of 706 respondents, with 353 participants each from urban and rural areas. Participants were recruited at the Deep Eye Care Foundation in Rangpur, Bangladesh, between April and September 2023. Ethical approval was obtained from the Ethical Review Committee of the Deep Eye…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
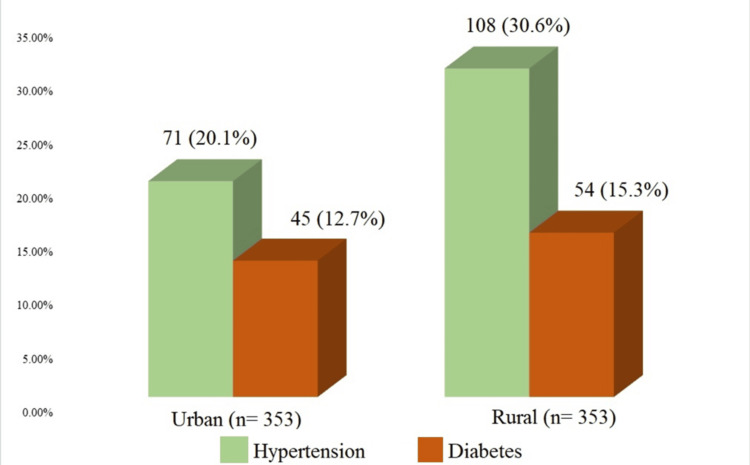 Figure 1
Figure 1| Parameters | Urban (n = 353) | Rural (n = 353) |
| Age (years) | ||
| ≤20 | 40 (11.3) | 5 (1.4) |
| 21-40 | 143 (40.5) | 88 (24.9) |
| 41-60 | 147 (41.6) | 151 (42.8) |
| ≥61 | 23 (6.5) | 109 (30.9) |
| Mean ± SD | 39.31 ± 14.1 | 52.01 ± 14.2 |
| Gender | ||
| Male | 156 (44.2) | 201 (56.9) |
| Female | 197 (55.8) | 152 (43.1) |
| Education | ||
| No formal education | 40 (11.3) | 159 (45) |
| Primary education | 49 (13.9) | 96 (27.2) |
| Secondary education | 70 (19.8) | 51 (14.4) |
| Higher secondary | 69 (19.5) | 24 (6.8) |
| Graduate | 81 (22.9) | 18 (5.1) |
| Post-graduate | 44 (12.5) | 5 (1.4) |
| Occupation | ||
| Homemaker | 112 (31.7) | 92 (26.1) |
| Business | 43 (12.2) | 77 (21.8) |
| Farmer | 12 (3.4) | 91 (25.8) |
| Service holder | 56 (15.9) | 29 (8.2) |
| Student | 58 (16.4) | 9 (2.5) |
| Unemployed | 21 (5.9) | 31 (8.8) |
| Retired | 12 (3.4) | 9 (2.5) |
| Day labor | 9 (2.5) | 12(3.4) |
| Others | 30 (8.5) | 3 (0.8) |
| Monthly family income (BDT) | ||
| <10,000 | 124 (35.1) | 186 (52.7) |
| 10,000-20,000 | 44 (12.5) | 97 (27.5) |
| 20,001-30,000 | 92 (26.1) | 53 (15) |
| 30,001-40,000 | 41 (11.6) | 9 (2.5) |
| 40,001-50,000 | 23 (6.5) | 4 (1.1) |
| >50,000 | 29 (8.2) | 4 (1.1) |
| Questions | Parameters | Urban (n = 353) | Rural (n = 353) | p-value | Chi-square value | Total, n (%) |
| History of eye examination | Yes | 229 (64.9) | 276 (78.2) | <0.001 | 15.364 | 505 (71.5) |
| No | 124 (35.1) | 77 (21.8) | 201 (28.5) | |||
| If yes, time of examination | Within 12 months | 112 (48.9) | 157 (56.9) | 0.074 | 3.198 | 269 (53.3) |
| Before 12 months | 117 (51.1) | 119 (43.1) | 236 (46.7) | |||
| If yes, place of examination | Government hospital/clinic | 24 (10.5) | 93 (33.7) | <0.001 | 74.482 | 117 (23.2) |
| Private hospital/clinic | 197 (86) | 137 (49.6) | 334 (66.1) | |||
| Outreach | 8(3.5) | 46(16.7) | 54 (10.7) | |||
| Have you ever heard of the term glaucoma before? | Yes | 80 (22.7) | 67 (19) | <0.001 | 22.063 | 147 (20.8) |
| No | 249 (70.5) | 284 (80.5) | 533 (75.5) | |||
| Don’t know | 24 (6.8) | 2 (0.6) | 26 (3.7) | |||
| Do you know that glaucoma is an eye disease? | Yes | 58 (16.4) | 64 (18.1) | <0.001 | 549.017 | 122 (17.3) |
| No | 7 (2) | 287 (81.3) | 294 (41.6) | |||
| Don’t know | 288 (81.6) | 2 (0.6) | 290 (41.1) | |||
| Source of information | Family member | 12 (15) | 32 (47.8) | <0.001 | 20.858 | 44 (29.9) |
| Relatives/friends | 27 (33.8) | 17 (25.4) | 44 (29.9) | |||
| Health professional | 22 (27.5) | 13 (19.4) | 35 (23.8) | |||
| Mass media | 19 (23.5) | 5 (7.5) | 24 (16.3) | |||
| Do you have a history of glaucoma? | Yes | 11 (13.3) | 43 (64.2) | <0.001 | 47.426 | 54 (36) |
| No | 47(56.6) | 8 (11.9) | 55 (36.7) | |||
| Don’t know | 25 (30.1) | 16 (23.9) | 41 (27.3) | |||
| If yes, types of treatment received | Medical | 6 (54.5) | 35 (81.4) | 0.005 | 13.030 | 41 (75.9) |
| Laser | 1 (9.1) | 6 (14) | 7 (13) | |||
| Surgical | 1 (9.1) | 2 (4.7) | 3 (5.6) | |||
| No treatment | 3 (27.3) | 0 | 3 (5.6) | |||
| Do you have a family history of glaucoma? | Yes | 6 (7.4) | 36 (53.7) | <0.001 | 55.651 | 42 (28.4) |
| No | 43 (53.1) | 3 (4.5) | 46 (31.1) | |||
| Don’t know | 32 (39.5) | 28 (41.8) | 60 (40.5) | |||
| If yes, mention the family with glaucoma diagnosis | Father | 2 (33.3) | 12 (33.3) | 0.174 | 6.358 | 14 (33.3) |
| Mother | 1 (16.7) | 19 (52.8) | 20 (47.6) | |||
| Sister | 2 (33.3) | 3 (8.3) | 5 (11.9) | |||
| Brother | 1 (16.7) | 1 (2.8) | 2 (2.4) | |||
| Grandfather | 0 | 1 (2.8) | 1 (2.4) |
| Questions | Urban (n = 80), n (%) | Rural (n = 67), n (%) | ||||
| Yes | No | I don’t know | Yes | No | I don’t know | |
| Do you know that glaucoma affects the optic nerve? | 26 (32.5) | 22 (27.5) | 32 (40) | 8 (11.9) | 34 (50.7) | 25 (37.3) |
| The risk of glaucoma increases with age | 41 (51.2) | 17 (21.3) | 22 (27.5) | 11 (16.4) | 2 (3) | 54 (80.6) |
| Glaucoma is inherited | 31 (38.8) | 26 (32.5) | 23 (28.7) | 8 (11.9) | 6 (9) | 53 (79.1) |
| Glaucoma can occur without symptoms | 26 (32.5) | 28 (35) | 26 (32.5) | 7 (10.4) | 6 (9) | 54 (80.6) |
| Associated with high intraocular pressure | 42 (52.5) | 18 (22.5) | 20 (25) | 15 (22.4) | 2 (3) | 50 (74.6) |
| Glaucoma progresses over time | 39 (48.8) | 19 (23.8) | 22 (27.5) | 13 (19.4) | 3 (4.5) | 51 (76.1) |
| Glaucoma can be cured | 38 (47.5) | 19 (23.8) | 23 (28.7) | 12 (17.9) | 4 (6) | 51 (76.1) |
| Glaucoma has treatment | 46 (57.5) | 11 (13.8) | 23 (28.7) | 21 (31.3) | 2 (3) | 44 (65.7) |
| Do you know that glaucoma can be treated with drops, laser therapy, or surgery? | 26 (32.5) | 22 (27.5) | 32 (40) | 9 (13.4) | 34 (50.7) | 24 (35.8) |
| Glaucoma causes blindness | 47 (58.8) | 9 (11.3) | 24 (30) | 18 (26.9) | 2 (3) | 47 (70.1) |
| Knowledge level | Urban (n = 80), n (%) | Rural (n = 67), n (%) | p-value | Chi-square value | Total, n (%) |
| Excellent (>75%) | 25 (31.3) | 6 (9) | <0.001 | 13.771 | 31 (21.1) |
| Good (50%-75%) | 14 (17.5) | 8 (11.9) | 22 (15) | ||
| Poor (<50%) | 41 (51.2) | 53 (79.1) | 94 (63.9) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlaucoma and retinal disorders · Ophthalmology and Visual Impairment Studies · Ophthalmology and Visual Health Research
Introduction
Glaucoma is a chronic, progressive optic neuropathy characterized by specific alterations in the optic disc and visual field loss, frequently associated with increased intraocular pressure (IOP) [1]. The gradient across the lamina cribrosa is significantly increased by elevated IOP and low perfusion pressure, resulting in papillary hypoperfusion. This process leads to structural changes and remodeling of the lamina cribrosa, as well as impaired axonal transport in the optic nerve fiber [2]. It is the primary cause of irreversible blindness worldwide and is the second most common cause of blindness globally, following cataracts. Unfortunately, due to its insidious nature, it is often diagnosed in advanced stages, leading to severe ocular damage [3]. Early intervention can help avert permanent vision loss, but a general lack of awareness and inadequate screening mechanisms contribute to delayed diagnoses, even among the educated population [4].
The global glaucoma prevalence among individuals aged 40-80 years is estimated at 3.54%. Primary open-angle glaucoma (POAG) is most prevalent in Africa, while primary angle-closure glaucoma (PACG) is more common in Asia. In 2013, an estimated 64.3 million people aged 40-80 years were affected by glaucoma worldwide. This number increased to 76.0 million in 2020 and is projected to reach 111.8 million by 2040 [5]. In Bangladesh, the prevalence of confirmed glaucoma among those aged 40 years and older ranges from 2.1% [6] to 3.2%, with an additional 10.1% categorized as glaucoma suspects [7].
Several studies have suggested that a significant number of glaucoma cases, spanning from 50% to 90%, remain undiagnosed [8]. Lack of awareness is frequently the primary cause of delayed glaucoma diagnosis, which greatly raises the risk of blindness from glaucoma [3,4]. Awareness is shaped by several socioeconomic variables, such as educational attainment, family history, availability of recreational sources, and outreach by public or non-governmental health education initiatives [8]. Limited awareness not only delays diagnosis but also deters people from utilizing essential eye care services [9].
There is no denying that glaucoma has significantly impacted family finances [10]. In low- and middle-income countries, the economic toll of blindness is particularly severe due to productivity losses and caregiving costs, which constrain national resources [11]. Financial hardship often undermines treatment adherence, and as the disease advances, patients require more frequent tests, medications, and clinical visits, driving up expenses [12]. The cornerstone of glaucoma treatment is IOP reduction, which is the only proven method to halt disease progression. Determining an individual’s target IOP involves considering several factors, including baseline pressure, age, optic nerve condition, and risk of progression. The American Academy of Ophthalmology recommends an initial 25% IOP reduction from baseline for managing POAG [13]. Surgical approaches, such as laser trabeculoplasty or trabeculectomy, are considered when medication fails to control IOP [14].
Major risk factors for glaucoma include increasing age, high IOP, a family history of the condition, and ethnic background [1]. Unfortunately, glaucoma is frequently detected at an advanced stage, resulting in considerable vision loss [15]. For this reason, assessing public knowledge and awareness is essential to formulate effective educational and communication strategies. Improving awareness can promote routine eye exams and help mitigate the financial strain associated with this condition [4,9]. This study was undertaken to assess the knowledge and awareness of glaucoma among rural and urban populations, to combat this sight-threatening disease.
Materials and methods
The study was conducted from April to September 2023. A total of 706 participants aged 18 years or older were included from rural and urban areas in the Rangpur district. The rural patients were selected from rural eye camps of the Deep Eye Care Foundation in Rangpur, Bangladesh. The urban population was selected from the general outpatient department of the Deep Eye Care Foundation. Individuals who consented to participate were briefed about the purpose of the study and were provided with a written consent form to sign. The study was conducted by doctors, optometrists, and refractionists who were trained on the questionnaire and had extensive knowledge of glaucoma. Inclusion criteria included patients over 18 years of age who provided informed written consent. Patients who were severely ill, unwilling to participate, under the age of 18, or mentally unstable were excluded from the study.
Sample size
The sample size for this study was calculated using the following formula:
\begin{document}n= \Bigg([P1(100-P1)+ P2(100-P2)]/(P1-P2)^2 \Bigg) (Zα+Zβ)^2\end{document}
where n represents the sample size, Zα denotes the Z-value of the standard normal deviation at a given level of significance (1.28 at 20% level of significance), Zβ states the standard normal deviation at a given power (typically set at 0.84 for an 80% power), P1 indicates the assumed prevalence of the awareness level in the urban group based on a previous study (25.94%), and P2 represents the estimated prevalence of the awareness level in the rural group from the same study (19.9%) [16].
By substituting these values into the formula, the initial estimated sample size was approximately 433 participants for each group (urban and rural). However, due to the unavailability of eligible participants, the targeted sample size could not be achieved. Consequently, a total of 706 participants were ultimately enrolled in the study, with 353 participants included in each group.
Development of the questionnaire
The survey questionnaire was developed after reviewing relevant literature and previously published studies on glaucoma awareness and knowledge [15,17-19]. Participants were asked to answer a pretested, semi-structured questionnaire to assess their awareness and knowledge of glaucoma. It was designed to collect information on three main areas: participants’ sociodemographic characteristics, awareness of glaucoma, and knowledge of the disease among those who were aware. The questionnaire was initially drafted in English and then translated into the local language, with back-translation performed to ensure accuracy and clarity.
Testing of the questionnaire
A pretest was conducted on a small sample of participants who were not included in the final study to assess the clarity of the questions, ease of understanding, and the practical feasibility of administering the questionnaire, including the time required and the smoothness of the interview process. Based on the feedback from the pretest, minor modifications were made to improve readability and overall administration.
Validation of the questionnaire
Content validity was established through expert review by ophthalmologists and public health specialists to ensure that all questions were relevant, clear, and comprehensive. Reliability was ensured by standardizing the administration procedures, which included providing consistent instructions to participants, maintaining the same order of questions, using a uniform method of delivery (face-to-face interviews), and addressing participants’ queries in a predefined manner. Scoring methods were also standardized to ensure consistency in evaluating responses.
Assessment of awareness and knowledge
The respondents who had heard of glaucoma were considered aware of the disease, and their knowledge was assessed based on their understanding of it. Participants who were unable to answer any questions were deemed not to know about glaucoma. Following the collection of demographic data, participants were asked awareness-related questions, including inquiries about medical history (e.g., history of diabetes mellitus (DM) and hypertension (HTN)), history of eye examinations, family history of glaucoma, and their sources of information. Awareness was assessed by asking participants, “Have you ever heard of the term ‘Glaucoma’?” [15].
Knowledge details were obtained only from participants who were aware of glaucoma [18]. Knowledge was assessed by questioning participants about the altered anatomical site, different types, clinical presentation, risk factors, association with high IOP and visual field, and treatment options for glaucoma. A Likert scale was used to measure the respondents’ knowledge and analyze their responses, where 1 = Yes, 2 = No, and 3 = I don’t know [15]. For each question, a correct answer was given a +1 score, while a wrong answer received no score. The sum of the scores from all 10 knowledge-related questions provided the final score for each participant. The knowledge level was then divided into three grades: poor, good, and excellent. Participants’ knowledge was categorized as “Excellent” if they achieved more than 75% of the total score, “Good” if they scored between 50% and 75%, and “Poor” if they scored less than 50% [17].
Data handling and analysis
The obtained data were entered into a Microsoft Excel (Microsoft Corp., Redmond, WA, USA) spreadsheet and analyzed using the IBM SPSS Statistics for Windows, Version 26.0 (Released Year; IBM Corp., Armonk, NY, USA). The chi-square test was applied, and a p-value less than 0.05 was considered statistically significant.
Ethical approval
Ethical approval was obtained from the Institutional Review Board (IRB) of the Deep Eye Care Foundation, Rangpur, Bangladesh (Ref. No: IRB/DECF/2023/R12).
Results
Table 1 presents the sociodemographic characteristics of the participants. The mean age of urban and rural participants was 39.31 ± 14.1 and 52.01 ± 14.2 years, respectively. In urban areas, most participants were aged 41-60 years (41.6%), followed by 21-40 years (40.5%). In rural areas, the largest group was also 41-60 years (42.8%), followed by ≥61 years (30.9%), compared to 6.5% in urban areas. Female participants predominated in urban areas (55.8%), while males were more common in rural areas (56.9%). A stark contrast was observed in educational attainment. Urban participants were more educated, with 22.9% being graduates and 12.5% postgraduates, while rural respondents had a high rate of no formal education (45%). Regarding occupation, urban areas had more homemakers (31.7%) and students (16.4%), whereas rural areas had higher proportions of homemakers (26.1%), farmers (25.8%), and business workers (21.8%). Urban families generally had higher incomes, with 8.2% earning over BDT 50,000 compared to only 1.1% in rural areas. More than half of rural participants (52.7%) earned less than BDT 10,000 monthly, reflecting significant economic disparities.
Figure 1 shows that both HTN (30.6%) and diabetes (15.3%) were more prevalent among rural participants than urban participants, with hypertension being the more common comorbidity in both groups.
History of comorbidities
Table 2 presents glaucoma awareness among participants. Rural participants were more likely to have had an eye exam (78.2%) compared to urban participants (64.9%) (p < 0.001). In urban areas, most eye exams occurred more than 12 months ago (51.1%), while in rural areas, most eye exams (56.9%) were recent (within 12 months), with no significant difference between urban and rural participants. Both urban (86%) and rural (49.6%) participants primarily visited private hospitals or clinics, whereas rural participants often relied on government facilities (33.7%) and outreach services (16.7%) (p < 0.001). Only 20.8% of participants had heard of the term “glaucoma,” with urban participants slightly more aware than rural participants (22.7% vs. 19%, p < 0.001). Just 17.3% recognized it as an eye disease. Alarmingly, 81.6% of urban and 81.3% of rural respondents either did not know or were unsure (p < 0.001). In rural areas, family members (47.8%) were the primary source of information, whereas urban participants relied more on relatives/friends (33.8%) and healthcare professionals (27.5%). A history of glaucoma was more common among rural respondents (64.2% vs. 13.3%, p < 0.001), as was a family history (53.7% vs. 7.4%, p < 0.001), with mothers being the most frequently reported affected family member (47.6%). Among participants with glaucoma, medical treatment was the most common approach (75.9%), more prevalent among rural participants (81.4%) than urban participants (54.5%) (p = 0.005). Very few reported laser or surgical treatments.
Table 3 evaluates participants’ knowledge of specific aspects of glaucoma. Urban participants consistently demonstrated greater knowledge than rural participants: 32.5% of urban and 11.9% of rural participants knew that glaucoma affects the optic nerve; 51.2% of urban versus 16.4% of rural participants knew that the risk of glaucoma increases with age. The statement “glaucoma is inherited” was known to 38.8% of urban participants and only 11.9% of rural participants. Additionally, 48.8% of urban participants knew that glaucoma is a progressive disease, compared to just 19.4% of rural participants. More urban participants knew that glaucoma is often asymptomatic (32.5% vs. 10.4%), linked to high IOP (52.5% vs. 22.4%), and can cause blindness (58.8% vs. 26.9%). Urban respondents were also more aware that glaucoma can be treated (57.5% vs. 31.3%) and were familiar with the available treatment modalities (drops, laser, surgery). Rural participants largely responded with “I don’t know,” highlighting significant knowledge gaps.
Table 4 summarizes overall glaucoma knowledge levels among urban and rural participants. A statistically significant association was found between the place of residence and knowledge level (p < 0.001). Excellent knowledge was more common among urban participants (31.3%) than rural participants (9%). Poor knowledge was predominant in rural areas (79.1%) compared to 51.2% in urban areas. Only 15% of all participants had “good” knowledge.
Discussion
Glaucoma is a leading cause of irreversible blindness, yet early diagnosis and timely treatment can effectively prevent vision loss. However, inadequate awareness and delayed presentation remain significant barriers to proper management and prevention of blindness associated with the disease. To the best of our knowledge, few comprehensive studies have simultaneously assessed glaucoma-related knowledge and awareness in both urban and rural populations of Bangladesh. In this cross-sectional study, we analyzed the level of knowledge and awareness regarding glaucoma among urban and rural populations, including a total of 706 respondents, with an equal distribution of 353 participants from each area.
The mean age of urban and rural respondents was not comparable (39.31 ± 14.1 vs. 52.01 ± 14.2 years). Female participants predominated in urban areas, whereas males were more common in rural areas. Interestingly, 53.7% of rural participants and only 7.4% of urban participants reported a family history of glaucoma. These findings are consistent with a study conducted in Bihar, India, by Sharma Pal [16].
Our study revealed that only 22.7% of urban and 19% of rural respondents were aware of the term “glaucoma.” Among those aware, 16.4% of urban and 18.1% of rural participants correctly identified glaucoma as an eye disease. Overall, respondents from urban areas demonstrated significantly higher awareness compared to their rural counterparts (Table 2). Notably, the overall level of awareness in our study was relatively low compared to previous studies in Bangladesh, where awareness levels ranged from 34.6% to 50% [15,19]. In contrast, a study in Ethiopia reported that only 2.4% of respondents were aware of glaucoma [20]. Similarly, studies conducted in various regions of India indicated lower levels of awareness among their study populations [21,22]. This variation in awareness levels across countries and regions may be attributed to differences in healthcare infrastructure, the reach and effectiveness of public health education campaigns, and the degree to which such programs penetrate urban versus rural communities.
Ocansey et al. reported that awareness about glaucoma in the general population is very poor [23]. In their study, over two-thirds of respondents were not aware of glaucoma, and more rural dwellers than urban dwellers were unaware of the condition. Even among those who reported being aware of glaucoma, some were unaware that it could cause blindness [23]. In our study, rural participants were more likely to have undergone an eye examination than their urban counterparts; however, urban respondents demonstrated greater awareness regarding key aspects of glaucoma. They were more likely to recognize it as a progressive disease, understand its potential to cause blindness, and be informed about treatment options. The reduced levels of awareness in certain populations may be attributed to lower educational attainment and less developed eye care systems, which limit access to both care and information.
Urban participants in our study consistently demonstrated a higher level of knowledge. For instance, 32.5% accurately identified the anatomical site affected by glaucoma, compared to only 11.9% of rural participants (Table 3). Similar patterns have been reported in studies by Sultana et al. and Becerril-Ledezma et al., who also highlighted greater knowledge among certain populations [15,24]. In Nepal, Sahu et al. reported that glaucoma awareness was only 14% among the rural population, compared to 65% in urban areas [25]. In Ghana, researchers found that overall knowledge of respondents about glaucoma was low [23]. Studies in India similarly revealed that knowledge of glaucoma among rural populations was very poor compared with urban populations [26]. These findings closely align with the results of our study.
A key finding of our study was the significant influence of education on glaucoma-related knowledge across both urban and rural groups. A marked disparity in educational attainment was observed, with 45% of rural respondents having no formal education. Participants with higher educational qualifications were statistically more likely to be aware of glaucoma, regardless of the place of residence. This association between education and awareness has also been supported by several studies conducted in northern and southern India, emphasizing that educational status plays a crucial role in improving knowledge and awareness of glaucoma [27,28].
In our study, the primary source of glaucoma awareness among rural participants was family members (47.8%), whereas urban participants most commonly cited relatives or friends (33.8%) and healthcare professionals (27.5%). In contrast, studies from southern India reported television and magazines as the most common sources of awareness, with family members affected by glaucoma ranking second. Similarly, surveys conducted in Germany found that friends were the leading source of glaucoma awareness (38%), surpassing physicians (16%), a trend also observed among urban populations in South India [26,29]. These differences highlight the varying impact of social networks and media exposure on health awareness across different cultural and geographic contexts.
Recall bias is an important limitation of this study, as it involved a degree of self-reporting. Participants were asked questions that required them to remember past events, which may have led to inaccuracies in their recollections, particularly among older individuals. To address the knowledge gap, strengthening community outreach, improving communication by healthcare providers, and integrating glaucoma awareness into routine eye care services are recommended. Enhancing public understanding is vital for facilitating early detection, ensuring timely treatment, and ultimately reducing the long-term burden of this preventable cause of blindness. These results can guide the development of targeted health education programs both within the study population and in similar communities, aiming to enhance awareness and knowledge of common eye diseases.
Conclusions
This study highlights a significant disparity in glaucoma awareness and knowledge between urban and rural populations. Urban participants, with higher education and better access to private healthcare, showed greater awareness and understanding of glaucoma. In contrast, rural respondents, despite a higher prevalence of glaucoma and more frequent eye examinations, demonstrated poor knowledge, with many unaware that glaucoma is an eye disease or that it can lead to irreversible blindness. The findings suggest that lack of education and limited access to reliable information contribute to delayed diagnosis and poor disease management in rural areas. There is a clear need for targeted health education initiatives focusing on glaucoma, especially in underserved communities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Glaucoma awareness among patients at outpatient department of ophthalmology in Smt. Kashibai Navale Medical College and General Hospital, Narhe, Pune IJSR Vakharia D Gokhale S 2415241932014 https://www.ijsr.net/getabstract.php?paperid=OCT 1434
- 2The diagnosis and treatment of glaucoma Dtsch Arztebl Int Schuster AK Erb C Hoffmann EM Dietlein T Pfeiffer N 2252341172020 https://www.aerzteblatt.de/10.3238/arztebl.2020.02253234366810.3238/arztebl.2020.0225 PMC 7196841 · doi ↗ · pubmed ↗
- 3Awareness and knowledge of glaucoma among adult patients at the eye clinic of a teaching hospital Ghana Med J Nkum G Lartey S Frimpong C Micah F Nkum B 1951994920152669319610.4314/gmj.v 49i 3.11PMC 4676595 · doi ↗ · pubmed ↗
- 4Glaucoma awareness in undiagnosed literate individuals attending routine eye clinic at a tertiary care center Indian J Clin Exp Ophthalmol Gupta S Rishi P 37037222016 https://ijceo.org/archive/volume/2/issue/4/article/20628
- 5Global prevalence of glaucoma and projections of glaucoma burden through 2040. A systematic review and meta-analysis Ophthalmology Tham YC Li X Wong TY Quigley HA Aung T Cheng CY 2081209012120142497481510.1016/j.ophtha.2014.05.013 · doi ↗ · pubmed ↗
- 6The prevalence of glaucoma in Bangladesh: a population based survey in Dhaka division Br J Ophthalmol Rahman MM Rahman N Foster PJ Haque Z Zaman AU Dineen B Johnson GJ 149314978820041554879610.1136/bjo.2004.043612 PMC 1772445 · doi ↗ · pubmed ↗
- 7Population-based survey of the prevalence and types of glaucoma in Bangladesh BMJ Open Ophthalmol Mannaf SM Islam MS Islam MN Rahman MM Parvin S Rahman S Sarker BK 9202410.1136/bmjophth-2023-001609 PMC 1098276338538147 · doi ↗ · pubmed ↗
- 8A study of awareness of glaucoma among ophthalmology out patients in a 2-tier city, Tumkur Ind Jour of Clin and Exper Ophth Sandhya R Sinha A Shetty N 15615812015 https://ijceo.org/archive/volume/1/issue/3/article/20525