Acute Psychosis as the Initial Presentation of Systemic Lupus Erythematosus Complicated by Posterior Reversible Encephalopathy Syndrome With Hemorrhage: A Case Report
Anas E Ahmed, Bothinah M Al Zahib, Aisha R Al-Rashidi, Abdulnasir H Almassloom, Nawaf S Althobaiti

TL;DR
A young woman with no psychiatric history developed sudden psychosis due to an undiagnosed autoimmune disease and brain swelling, which improved with timely treatment.
Contribution
This case highlights acute psychosis as a rare initial sign of systemic lupus erythematosus complicated by PRES with hemorrhage.
Findings
Acute psychosis in a young patient was linked to undiagnosed systemic lupus erythematosus and PRES with hemorrhage.
Timely neuroimaging and systemic evaluation led to diagnosis and successful treatment with immunosuppression and blood pressure control.
The case underscores the importance of multidisciplinary care in managing complex neuropsychiatric autoimmune presentations.
Abstract
Acute psychosis may rarely represent the initial presentation of an underlying systemic and potentially life-threatening medical disorder, posing significant diagnostic and management challenges. We report the case of a young woman with no prior psychiatric history who presented with abrupt-onset psychosis and behavioral disturbance. Early neuroimaging revealed posterior-predominant vasogenic edema with associated intracerebral hemorrhage, consistent with posterior reversible encephalopathy syndrome (PRES). Further evaluation demonstrated hematological abnormalities, renal involvement, and positive autoimmune serology, leading to the diagnosis of previously unrecognized systemic lupus erythematosus (SLE) with neuropsychiatric involvement. The patient was managed with blood pressure control, immunosuppressive therapy, and supportive neurological and psychiatric care, resulting in marked…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1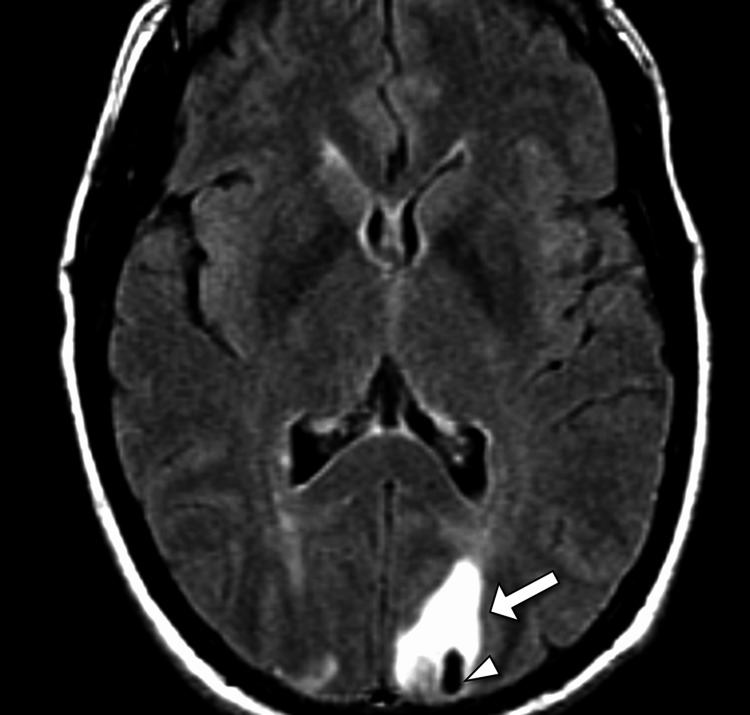 Figure 2
Figure 2| Parameter | Patient Value | Unit | Reference Range |
| Hemoglobin | 10.8 | g/dL | 12.0–16.0 |
| White blood cell count | 3.2 | ×10⁹/L | 4.0–11.0 |
| Neutrophils | 58 | % | 40–75 |
| Lymphocytes | 32 | % | 20–45 |
| Platelet count | 110 | ×10⁹/L | 150–400 |
| Mean corpuscular volume | 88 | fL | 80–100 |
| Erythrocyte sedimentation rate | 58 | mm/hour | <20 |
| C-reactive protein | 12 | mg/L | <5 |
| Serum creatinine | 0.9 | mg/dL | 0.6–1.1 |
| Blood urea nitrogen | 14 | mg/dL | 7–20 |
| Sodium | 138 | mmol/L | 135–145 |
| Potassium | 4.1 | mmol/L | 3.5–5.1 |
| Chloride | 102 | mmol/L | 98–107 |
| Bicarbonate | 24 | mmol/L | 22–28 |
| Aspartate aminotransferase | 28 | U/L | 10–40 |
| Alanine aminotransferase | 32 | U/L | 7–56 |
| Alkaline phosphatase | 84 | U/L | 44–147 |
| Total bilirubin | 0.7 | mg/dL | 0.2–1.2 |
| Thyroid-stimulating hormone | 2.1 | µIU/mL | 0.4–4.0 |
| Vitamin B12 | 420 | pg/mL | 200–900 |
| Serum ammonia | 26 | µmol/L | 15–45 |
| Antinuclear antibody | Positive | - | Negative |
| Anti-double-stranded DNA antibody | 180 | IU/mL | <30 |
| Anti-Smith antibody | Positive | - | Negative |
| Complement C3 | 48 | mg/dL | 90–180 |
| Complement C4 | 6 | mg/dL | 10–40 |
| Antiphospholipid antibodies | Negative | - | Negative |
| Urine protein-to-creatinine ratio | 1.8 | g/g | <0.2 |
| Urine red blood cells | 15–20 | /HPF | 0–3 |
| Urine white blood cells | 2–4 | /HPF | 0–5 |
| Urine toxicology | Negative | - | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological Complications and Syndromes · Neurological and metabolic disorders · Autoimmune Neurological Disorders and Treatments
Introduction
Acute psychosis as the initial manifestation of an underlying systemic medical disorder represents a significant diagnostic challenge in emergency and inpatient settings. While primary psychiatric illnesses are common causes of psychotic presentations in young adults, secondary etiologies such as autoimmune, metabolic, infectious, and vascular conditions must be carefully considered, particularly when neuroimaging or laboratory abnormalities are present [1-3]. Posterior reversible encephalopathy syndrome (PRES) is a clinico-radiological entity characterized by acute neurological symptoms, including altered mental status, seizures, visual disturbances, and, less commonly, prominent psychiatric features [1,3]. It is typically associated with acute blood pressure fluctuations, renal dysfunction, cytotoxic therapies, and autoimmune diseases, and is defined radiologically by reversible vasogenic edema predominantly affecting the posterior cerebral regions [3,4].
Systemic lupus erythematosus (SLE) is a chronic multisystem autoimmune disease with heterogeneous clinical manifestations, including neuropsychiatric involvement [1,3]. Neuropsychiatric systemic lupus erythematosus (NPSLE) encompasses a broad spectrum of central and peripheral nervous system manifestations, ranging from cognitive dysfunction and mood disorders to seizures, cerebrovascular disease, and psychosis [2,3]. PRES has increasingly been recognized as a neurological complication of SLE, often related to endothelial dysfunction, immune-mediated vascular injury, and disease activity, and may be further complicated by intracerebral hemorrhage [1-4]. The coexistence of acute psychosis, PRES with hemorrhagic features, and previously undiagnosed SLE is uncommon and underscores the importance of maintaining a high index of suspicion for systemic autoimmune disease in patients presenting with acute neuropsychiatric symptoms.
Case presentation
A previously healthy young adult woman in her early 20s, with no known psychiatric illness, was brought to the Emergency Department by her family because of abrupt-onset behavioral changes over 48 hours. According to relatives, she had been well until two days before presentation, when she developed insomnia, marked agitation, and progressive disorganized behavior. This was followed by paranoid ideation, incoherent speech, emotional lability, and visual hallucinations. There was no preceding fever, headache, seizure activity, head trauma, or substance use reported. Her past medical history was unremarkable, with no known autoimmune disease, hypertension, renal disease, or prior neurological events. She was not taking any regular medications, including oral contraceptives or illicit drugs. There was no family history of psychiatric disorders, autoimmune disease, or cerebrovascular events. Review of systems, obtained from family members, revealed intermittent joint pains and photosensitivity over the preceding several months, which had not been medically evaluated, but no prior neuropsychiatric symptoms.
On initial examination, the patient was acutely distressed, restless, and uncooperative. Vital signs showed a blood pressure of 158/96 mmHg, heart rate of 112 beats per minute, respiratory rate of 18 breaths per minute, temperature of 36.8°C, and oxygen saturation of 98% on room air. She was alert but disoriented to time and place, with poor attention and impaired judgment. Speech was pressured and tangential. Thought content was notable for persecutory delusions and visual hallucinations. Cranial nerve examination was limited by poor cooperation, but was grossly intact. Motor examination revealed normal tone and power in all four limbs, with no focal weakness. Sensory examination was noncontributory. Reflexes were symmetric, and plantar responses were flexor bilaterally. No meningeal signs were present. General physical examination revealed a faint malar rash sparing the nasolabial folds and mild non-erosive tenderness of the small joints of the hands without swelling. Cardiovascular, respiratory, and abdominal examinations were otherwise unremarkable.
Initial laboratory investigations demonstrated mild normocytic anemia (hemoglobin 10.8 g/dL), leukopenia (white blood cell count 3.2 × 10⁹/L), and thrombocytopenia (platelet count 110 × 10⁹/L). Serum electrolytes, renal function tests, liver enzymes, thyroid function tests, serum ammonia, vitamin B12, and toxicology screen were within normal limits. Inflammatory markers showed an elevated erythrocyte sedimentation rate of 58 mm/hour, with a mildly raised C-reactive protein. Given the acute psychosis with altered mental status, an urgent non-contrast computed tomography (CT) scan of the head was performed, which revealed bilateral parieto-occipital hypodensities consistent with vasogenic edema - more pronounced on the left - along with an acute intraparenchymal hemorrhage in the left occipital lobe, without significant midline shift. These findings raised concern for PRES, complicated by hemorrhage (Figure 1).
Axial CT image demonstrating subcortical hypodensity and hemorrhage in posterior reversible encephalopathy syndromeAxial non-contrast computed tomography (CT) of the brain shows a subcortical hypodense area in the left parietal lobe (arrow) with an associated focal intraparenchymal hemorrhage (arrowhead). These findings are consistent with posterior reversible encephalopathy syndrome (PRES) with hemorrhagic transformation.
Subsequent magnetic resonance imaging (MRI) of the brain demonstrated symmetrical hyperintense signals on T2-weighted and fluid-attenuated inversion recovery (FLAIR) sequences involving the bilateral occipital and parietal lobes, extending to the posterior temporal regions, consistent with vasogenic edema (Figure 2). Electroencephalography (EEG) performed due to fluctuating mental status showed diffuse slowing without epileptiform discharges.
Axial MRI FLAIR showing parietal hyperintensity and hemorrhage in posterior reversible encephalopathy syndromeAxial magnetic resonance imaging (MRI) using fluid-attenuated inversion recovery (FLAIR) demonstrates a hyperintense signal in the left parietal lobe (arrow). A corresponding blooming artifact on susceptibility-weighted imaging (arrowhead) indicates hemorrhage. These features are characteristic of posterior reversible encephalopathy syndrome (PRES) with hemorrhagic involvement.
Given the radiological diagnosis of PRES in a young patient without chronic hypertension, further etiological workup was undertaken (Table 1). Autoimmune testing revealed a strongly positive antinuclear antibody (ANA) with a homogenous pattern, elevated anti-double-stranded DNA (anti-dsDNA) antibodies, and low complement levels (C3 and C4). Urinalysis demonstrated proteinuria and microscopic hematuria, with a urine protein-to-creatinine ratio of 1.8 g/g. Additional testing showed positive anti-Smith antibodies, while antiphospholipid antibodies (aPL) were negative. Cerebrospinal fluid (CSF) analysis was deferred due to the presence of an intracerebral hemorrhage. Based on the Systemic Lupus International Collaborating Clinics (SLICC) criteria, a diagnosis of SLE, with neuropsychiatric involvement presenting as PRES, was established.
The patient was admitted to the Intensive Care Unit (ICU) for close neurological monitoring. Blood pressure was carefully controlled with intravenous antihypertensive agents to maintain systolic pressures below 140 mmHg. High-dose intravenous methylprednisolone was initiated for suspected lupus-related neuroinflammation, followed by a planned taper. Antipsychotic medication was used short-term to manage severe agitation, and seizure prophylaxis was administered, given the hemorrhagic lesion and EEG findings. Neurosurgical consultation recommended conservative management of the occipital hemorrhage. Over the ensuing days, the patient’s mental status gradually improved, with resolution of hallucinations and normalization of behavior.
She was discharged after three weeks on oral corticosteroids, hydroxychloroquine, and antihypertensive therapy, with close follow-up arranged with rheumatology, neurology, and psychiatry. At six-week outpatient follow-up, she was fully oriented, without residual psychotic symptoms or focal neurological deficits.
Discussion
The present case illustrates an uncommon but clinically significant presentation of SLE, in which acute psychosis was the dominant initial manifestation and was ultimately attributed to PRES complicated by intracerebral hemorrhage. This constellation of findings underscores the diagnostic complexity of acute neuropsychiatric presentations and highlights the critical importance of considering secondary, potentially reversible causes of psychosis, particularly in young patients without a prior psychiatric history. The case also contributes to the growing body of literature recognizing PRES as an important, albeit underappreciated, manifestation of NPSLE.
Neuropsychiatric involvement in SLE encompasses a broad and heterogeneous spectrum, ranging from mild cognitive dysfunction and mood disorders to severe manifestations such as seizures, cerebrovascular disease, and psychosis [1-4]. Psychosis occurs in a minority of patients with SLE but is a well-recognized and potentially severe manifestation, often associated with high disease activity and serological abnormalities, including elevated anti-dsDNA antibodies and hypocomplementemia, as observed in this case [2,5]. Distinguishing primary lupus psychosis from secondary neuropsychiatric complications such as PRES, infection, metabolic derangements, or medication-related effects is essential, as management strategies and prognoses differ significantly [4-7]. In this patient, the neuroimaging findings of posterior-predominant vasogenic edema with hemorrhagic transformation, along with rapid radiological reversibility following treatment, were more consistent with PRES rather than isolated lupus psychosis or cerebral vasculitis.
The occurrence of intracerebral hemorrhage in PRES, although relatively uncommon, has been increasingly reported, particularly in patients with autoimmune diseases [1-3]. Hemorrhagic complications may result from severe endothelial injury, reperfusion injury, or coexisting thrombocytopenia and coagulopathy, all of which are relevant in SLE. The presence of hemorrhage can complicate both diagnosis and management, limiting the use of certain diagnostic procedures such as lumbar puncture and increasing the risk of neurological morbidity [2,6]. Nevertheless, conservative management with close monitoring, blood pressure control, and treatment of the underlying cause is often sufficient, as demonstrated by the favorable outcome in this case.
From a diagnostic perspective, this case emphasizes the pivotal role of early neuroimaging in patients presenting with acute psychosis and altered mental status. Reliance solely on clinical psychiatric assessment risks misdiagnosis and delays in identifying potentially life-threatening neurological conditions [2-5]. CT remains a valuable initial modality in the emergency setting, particularly for detecting hemorrhage, while MRI provides superior characterization of PRES and helps differentiate it from ischemic stroke, infection, demyelination, or vasculitis [1,6]. Additionally, a systematic laboratory evaluation, including autoimmune serology, is essential in young patients with unexplained neuropsychiatric symptoms, especially when accompanied by systemic features such as cytopenias, rash, or renal abnormalities [2-5].
Therapeutically, management of PRES centers on prompt identification and correction of precipitating factors [1,4]. In SLE-associated PRES, this includes aggressive control of blood pressure, withdrawal of offending agents, if present, and treatment of active lupus with immunosuppressive therapy. High-dose corticosteroids are commonly employed in the setting of NPSLE, and were associated with marked clinical improvement in this patient. The favorable neurological and radiological recovery observed reinforces the concept that PRES is potentially reversible when recognized early and managed appropriately. However, delayed diagnosis, or inadequate treatment, may result in permanent neurological deficits or death, particularly in cases complicated by hemorrhage or infarction [5-8].
Conclusions
This case highlights the importance of a comprehensive and multidisciplinary approach to patients presenting with acute psychosis, particularly when clinical features are atypical for a primary psychiatric disorder. The identification of PRES with associated intracerebral hemorrhage on early neuroimaging was pivotal in prompting an expanded diagnostic evaluation that ultimately revealed previously undiagnosed SLE with neuropsychiatric involvement. Prompt recognition of the underlying autoimmune etiology allowed timely initiation of immunosuppressive therapy and strict blood pressure control, leading to significant clinical and radiological recovery.
The case underscores that acute psychosis may be the initial manifestation of serious systemic and neurological disease, and emphasizes the critical role of neuroimaging, autoimmune workup, and close interdisciplinary collaboration in such presentations. Early diagnosis and targeted management are essential to prevent irreversible neurological injury and to improve outcomes, reinforcing the need for clinicians to maintain a high index of suspicion for secondary causes of psychosis, including autoimmune disorders, in acute and atypical neuropsychiatric presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Neuropsychiatric lupus with posterior reversible encephalopathy syndrome: a rare presentation BMJ Case Rep Islam R Das S Chattopadhyay S Basu S 24149414202110.1136/bcr-2020-241494 PMC 821107234135075 · doi ↗ · pubmed ↗
- 2Psychiatric symptoms in systemic lupus erythematosus: a systematic review J Clin Psychiatry Meszaros ZS Perl A Faraone SV 99310017320122268774210.4088/JCP.11r 07425 PMC 9903299 · doi ↗ · pubmed ↗
- 3Posterior reversible encephalopathy syndrome: a truly treatable neurologic illness Perit Dial Int Hobson EV Craven I Blank SC 5905943220122321285810.3747/pdi.2012.00152 PMC 3524908 · doi ↗ · pubmed ↗
- 4Psychosis in a young female - a diagnostic and therapeutic challenge JRSM Short Rep Nizam S Gough A 22120102110311410.1258/shorts.2010.010025 PMC 2984349 · doi ↗ · pubmed ↗
- 5Systemic lupus erythematosus complicated with posterior reversible encephalopathy syndrome and intracranial vasculopathy Int J Rheum Dis Chen HA Lin YJ Chen PC Chen TY Lin KC Cheng HH 08213201010.1111/j.1756-185X.2010.01545.x 21199460 · doi ↗ · pubmed ↗
- 6Clinical features and outcomes of posterior reversible encephalopathy syndrome in patients with systemic lupus erythematosus Arthritis Care Res (Hoboken) Lai CC Chen WS Chang YS 176617746520132368706710.1002/acr.22047 · doi ↗ · pubmed ↗
- 7Post reversible encephalopathy syndrome attributed to mycophenolate mofetil used in the treatment of SLE: a case report and review of literature J Int Med Res Dai Y Liu W Hong F 862052202410.1177/03000605231218620 PMC 1075744238156668 · doi ↗ · pubmed ↗
- 8Posterior reversible encephalopathy syndrome with hemorrhagic transformation in the postoperative period of a kidney transplant Cureus Dehesa-Lopez E Irizar-Santana SS Valdez-Cruz MA Sosa-Guerrero S Lopez-Moreno F 016202410.7759/cureus.55584 PMC 1099310038576656 · doi ↗ · pubmed ↗