Sequential Varicella and Herpes Zoster in an Immunocompetent Adult
Bibek Sharma, Supriya Paudel

TL;DR
This paper reports a rare case of an immunocompetent adult experiencing both chickenpox and shingles in different skin areas, highlighting the need for careful diagnosis.
Contribution
The paper presents a rare sequential case of varicella and herpes zoster in noncontiguous dermatomes in an immunocompetent adult.
Findings
Varicella and herpes zoster occurred sequentially in noncontiguous dermatomes.
Clinicopathological correlation is crucial for diagnosing atypical presentations of VZV infections.
Abstract
Varicella and herpes zoster, caused by primary infection and reactivation of varicella‐zoster virus (VZV) respectively, can present with a wide spectrum of cutaneous and systemic complications. This case highlights an uncommon sequential presentation of varicella and zoster in an immunocompetent adult in noncontiguous dermatomes and emphasizes the importance of clinicopathological correlation in atypical presentations.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3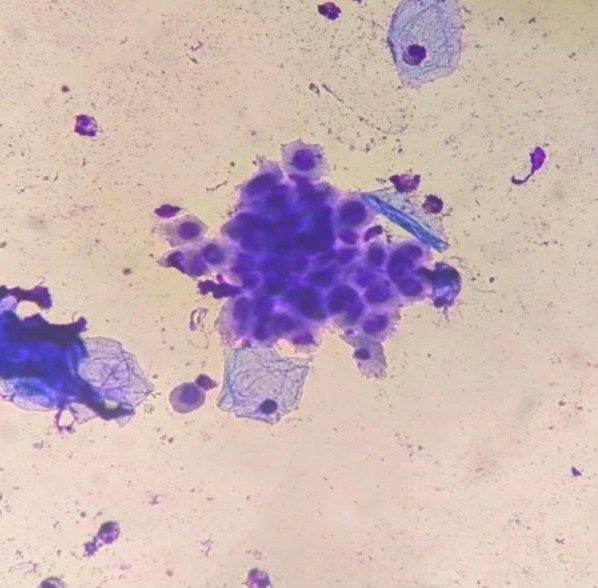 FIGURE 4
FIGURE 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Skin Diseases and Diabetes · Poxvirus research and outbreaks
Introduction
1
Varicella and herpes zoster are distinct clinical entities caused by varicella‐zoster virus (VZV). Primary infection manifests as varicella, while herpes zoster occurs due to viral reactivation from sensory ganglia, usually decades later. The risk of herpes zoster increases with age and immunosuppression [1]. Sequential or near‐simultaneous occurrence of varicella and herpes zoster in immunocompetent adults is exceptionally rare, with only a few cases reported in the literature [2, 3]. Here, we present such a case in a 45‐year‐old male, with clinicopathological confirmation and unusual cervical dermatomal involvement.
Case History
2
A 45‐year‐old previously healthy male with no known comorbidities presented with acute febrile illness followed by cutaneous eruptions. The patient initially developed fever and myalgia, followed 2 days later by generalized pleomorphic vesicles consistent with varicella. Within three subsequent days, he developed severe shoulder pain on the left side. On examination, the trunk and extremities showed pleomorphic papules, vesicles, and crusted lesions (Figure 1) In addition, grouped vesicles on an erythematous base were distributed along the left C4 and C7 dermatomes, suggestive of herpes zoster (Figures 2 and 3).
Grouped vesicles on left C4 dermatome.
Grouped vesicles on left C7 dermatome.
Varicella lesions on the trunk.
Methods
3
Laboratory investigations, including complete blood count, liver and renal function, fasting glucose, and HIV serology, were within normal limits. Giemsa stain of vesicular fluid revealed multinucleated giant cells with ballooning degeneration, consistent with herpesvirus cytopathic changes [4] (Figure 4).
Giemsa stain showing multinucleated giant cells with ballooning degeneration (×400).
He was treated with oral acyclovir 800 mg five times daily for 7 days; the lesions improved significantly, with complete resolution and no postherpetic neuralgia on follow‐up [5].
Conclusion and Results
4
The sequential development of varicella and herpes zoster in an immunocompetent adult is extremely uncommon as most zoster cases occur years to decades after primary infection [1].
Discussion
5
Several nonmutually exclusive mechanisms may explain this phenomenon. First, transient immune dysregulation induced by acute primary VZV infection or by other concurrent stress could permit a window for premature viral reactivation from sensory ganglia [3, 6]. Second, simultaneous exposure to distinct VZV strains or infection with multiple viral genotypes has been proposed in older case reports, and recent molecular studies confirmed different or vaccine‐strain sequences underlying atypical presentations. Where available, PCR and genotype analysis can help distinguish reactivation from coinfection [2, 6]. Third, true concurrent reactivation with other herpesviruses (e.g., HSV and VZV) has been described, highlighting the broader phenomenon of herpesvirus coreactivation in certain clinical settings [7].
Our patient demonstrated involvement of noncontiguous cervical dermatomes (C4 and C7). While thoracic dermatomes are most frequently affected in herpes zoster, cervical involvement, particularly multidermatomal, has been described and is often associated with severe neuropathic pain and risk of postherpetic neuralgia [8]. Early recognition is crucial to avoid misdiagnosis, particularly when zoster lesions appear atypically during or shortly after varicella. Previous reports suggest that early initiation of antiviral therapy, such as acyclovir, significantly reduces morbidity and prevents complications, even in immunocompetent adults. He received a 7‐day standard acyclovir course, consistent with international recommendations, leading to resolution without complications [5]. The addition of Giemsa cytology, demonstrating multinucleated giant cells, provided histopathological evidence, further strengthening the diagnosis.
Our case contributes to the limited literature on sequential varicella and herpes zoster in an immunocompetent adult with cervical noncontiguous dermatomal involvement, highlighting the possible molecular mechanism and importance of clinicopathological correlation, especially when faced with atypical presentations.
Author Contributions
Bibek Sharma: conceptualization, formal analysis, resources, software, validation, visualization, writing – original draft, writing – review and editing. Supriya Paudel: conceptualization, formal analysis, resources, supervision, validation, visualization, writing – original draft.
Funding
The authors have nothing to report.
Consent
A written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. A. Gershon , J. Breuer , J. I. Cohen , et al., “Varicella‐Zoster Virus Infection,” Nature Reviews Disease Primers 1 (2015): 15016.10.1038/nrdp.2015.16PMC 538180727188665 · doi ↗ · pubmed ↗
- 2G. Xie , Q. Wei , W. Guo , et al., “An Adult Co‐Presented With Varicella and Herpes Zoster Caused by Varicella Zoster Virus Genotype J: A Case Report,” BMC Infectious Diseases 20 (2020): 454.32600274 10.1186/s 12879-020-05192-3PMC 7325039 · doi ↗ · pubmed ↗
- 3F. Salvotti , S. Trapletti , G. Chiarini , M. Castellano , and M. L. Muiesan , “Atypical Varicella‐Zoster Virus Reactivation: A Case Report,” European Journal of Case Reports in Internal Medicine 10 (2023): e 003945.10.12890/2023_003945 PMC 1048213037680775 · doi ↗ · pubmed ↗
- 4N. Chhabra , C. Grover , and B. S. N. Reddy , “Concurrent Occurrence of Varicella and Herpes Zoster in an Immunocompetent Adult,” Indian Journal of Dermatology, Venereology and Leprology 75, no. 4 (2009): 432–434.
- 5D. Z. J. Lim , “Herpes Zoster and Post‐Herpetic Neuralgia—Diagnosis, Management and Prevention,” Pathogens 13 (2024): 596.39057822 10.3390/pathogens 13070596 PMC 11280284 · doi ↗ · pubmed ↗
- 6O. A. Fashina , T. M. Chuang , P. J. Galardy , et al., “Disseminated Vaccine‐Strain Varicella‐Zoster Virus Reactivation in an Adolescent With Secondary Immunodeficiency: A Case Report and Literature Review,” BMC Infectious Diseases 24 (2024): 1296, 10.1186/s 12879-024-09776-1.39543470 PMC 11566423 · doi ↗ · pubmed ↗
- 7M. Costa‐Silva , J. Sobrinho‐Simões , F. Azevedo , and C. Lisboa , “Concurrent Reactivation of Varicella Zoster Virus and Herpes Simplex Virus in an Immunocompetent Adult, BMJ Case Reports,” (2019).10.1016/j.abd.2019.01.003PMC 693909031789259 · doi ↗ · pubmed ↗
- 8J. W. Gnann, Jr. and R. J. Whitley , “Clinical Practice: Herpes Zoster,” New England Journal of Medicine 347 (2002): 340–346.12151472 10.1056/NEJ Mcp 013211 · doi ↗ · pubmed ↗