Motion-based tissue ex vivo (MOTEX) assay to assess proton and X-ray irradiation responses in head and neck squamous cell carcinoma
Katrin S. Pachler, Iris Lauwers, Nicole S. Verkaik, Marta Rovituso, Hetty Mast, Brend P. Jonker, Bernd Kremer, Sjors A. Koppes, Thierry P.P. van den Bosch, Gerda M. Verduijn, Steven Petit, Brita S. Sørensen, Dik C. van Gent, Marta E. Capala

TL;DR
A new ex vivo assay shows some head and neck tumors respond better to proton than X-ray radiation, linked to DNA repair issues or low immune cell presence.
Contribution
Introduces MOTEX, an ex vivo assay to assess proton and X-ray irradiation responses in HNSCC with novel insights into tumor heterogeneity.
Findings
Three out of nine tumors showed increased sensitivity to proton irradiation.
Proton-sensitive tumors were either HR-deficient or had low immune infiltration.
Not all immune-deserted tumors exhibited X-ray resistance.
Abstract
•Proton-sensitive HNSCC tumors were identified with an ex vivo irradiation.•One of the proton-sensitive tumors was homologous recombination (HR) deficient.•Two X rays-resistant but proton-sensitive tumors had low immune cell infiltration. Proton-sensitive HNSCC tumors were identified with an ex vivo irradiation. One of the proton-sensitive tumors was homologous recombination (HR) deficient. Two X rays-resistant but proton-sensitive tumors had low immune cell infiltration. Proton radiotherapy is applied for various tumor sites, offering better dose distribution resulting in decreased excess radiation of healthy tissue. Furthermore, the biological effects of proton irradiation may be different from X-ray irradiation, depending on tumor characteristics. This is particularly relevant for head and neck squamous cell carcinoma (HNSCC), which displays high biological heterogeneity.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
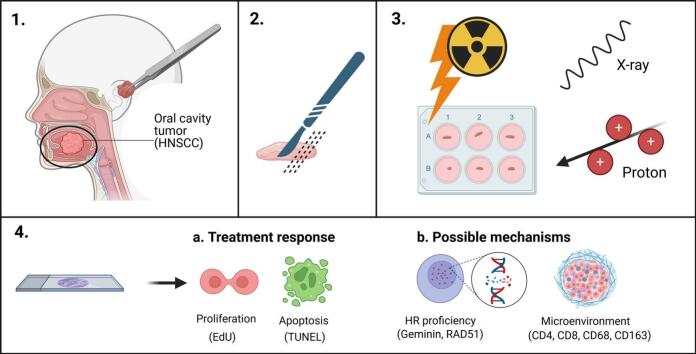 Figure 1
Figure 1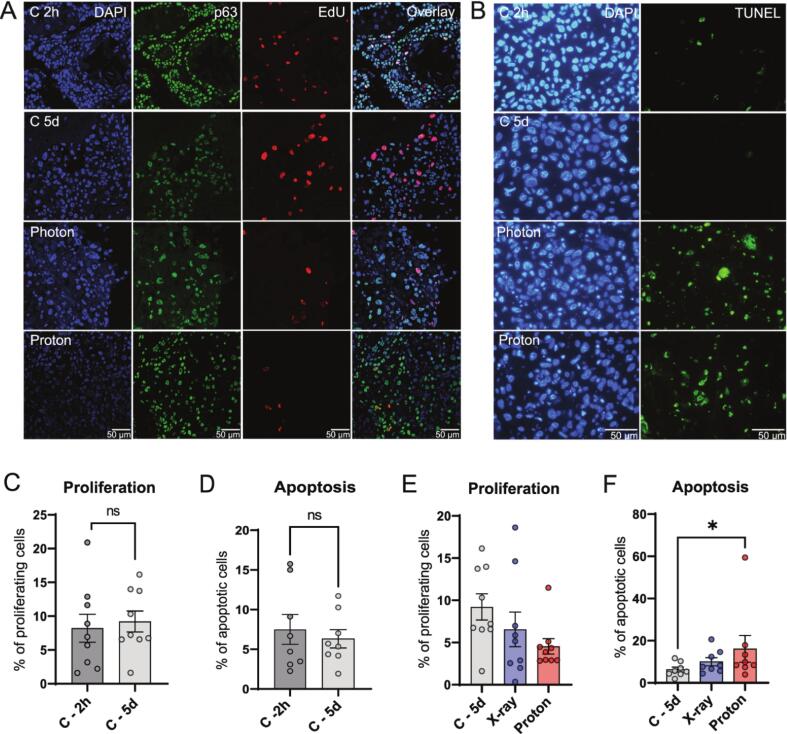 Figure 2
Figure 2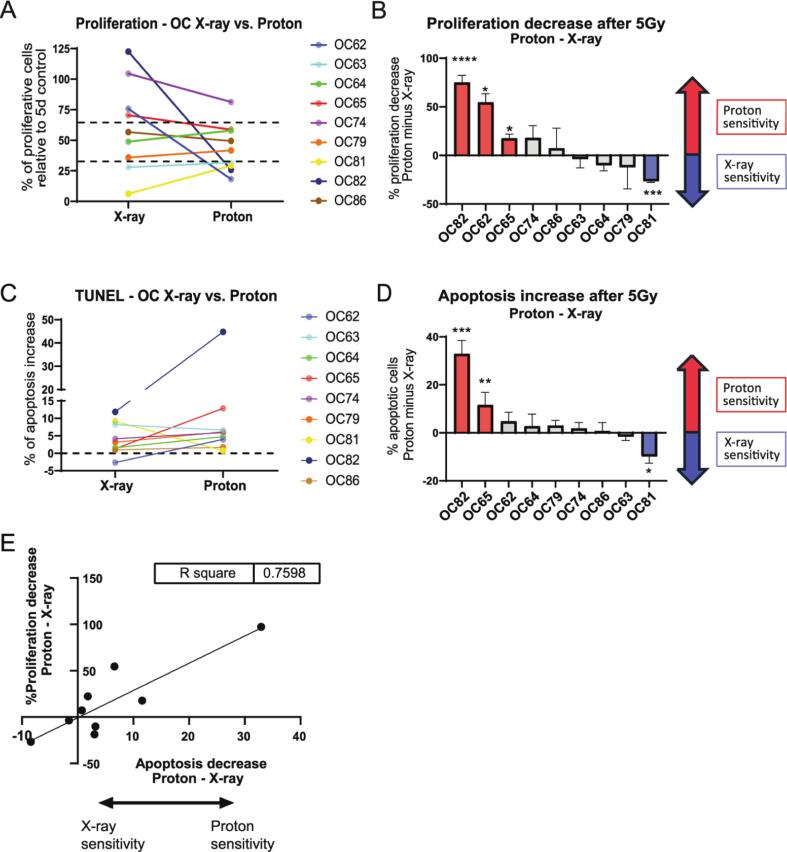 Figure 3
Figure 3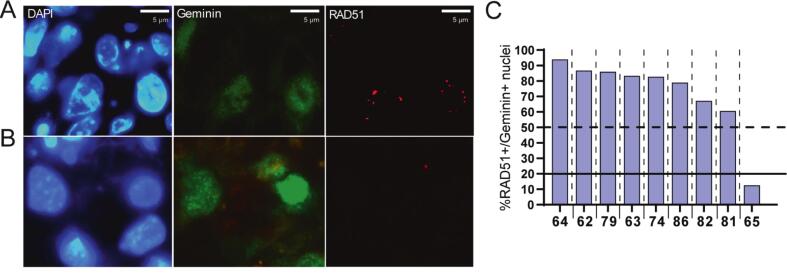 Figure 4
Figure 4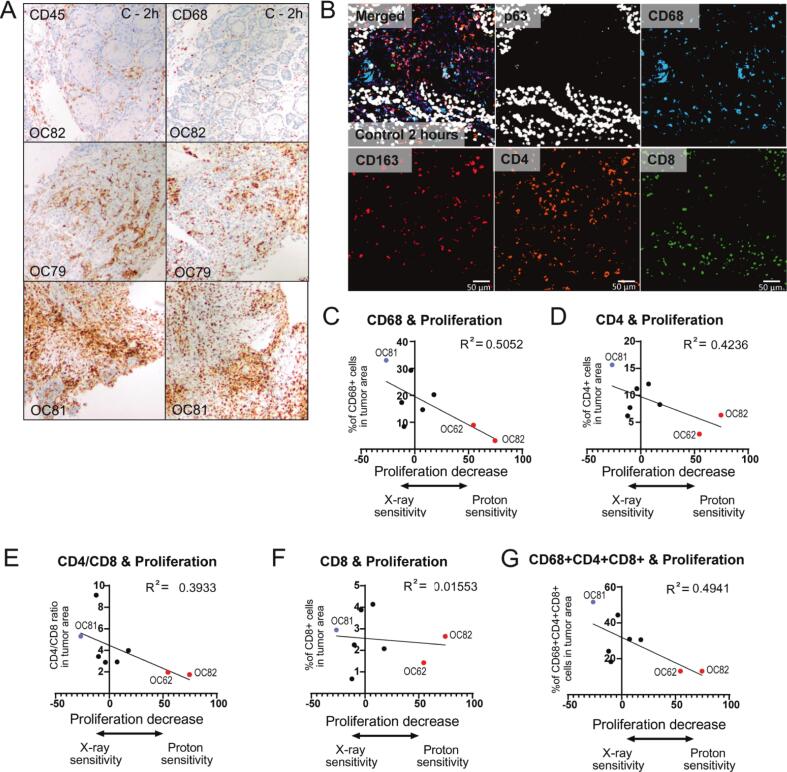 Figure 5
Figure 5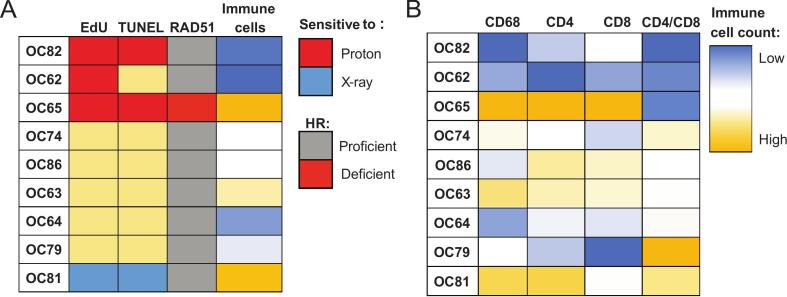 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiation Therapy and Dosimetry · Advanced Radiotherapy Techniques · Effects of Radiation Exposure
Introduction
Surgical resection and (chemo-)radiotherapy are the most common treatment modalities for head and neck squamous cell carcinoma (HNSCC) [1]. The radiotherapy dose is limited for tumors in the pharynx and oral cavity area, due to surrounding vital structures, so-called organs-at-risks (OARs) [2]. Proton radiotherapy offers a favorable dose distribution and decreased excess radiation of healthy tissue in comparison to conventional X-ray radiotherapy [3], [4], [5], [6]. Treatment requires balancing sufficient radiation dose to the tumor against sparing of the OARs, which is hampered by the heterogeneity in tumor responses. As this high level of heterogeneity cannot be explained entirely by clinical factors [7], several biological properties of the tumor have been proposed to influence radiotherapy response [1], [2].
Repair of DNA double strand breaks (DSBs), the main cell-killing effect of ionizing radiation, has been investigated extensively. Mutations in DNA repair pathways rendered some patients more sensitive to irradiation [8]. The main DNA repair pathways that counteract radiation-induced DSBs are homologous recombination (HR) and non-homologous end joining (NHEJ). While NHEJ is important for repairing both X-ray and proton induced DNA damage, several studies reported that HR is relatively more important for the repair of DSBs caused by proton irradiation [8], [9]. Due to higher linear energy transfer (LET) in the Bragg peak, protons can cause more clustered and complex DNA damage than X-rays. HR may be required for repair of these complex DSBs [8], [9], suggesting that differences in sensitivity to various types of radiation might be explained by the relative efficiency of HR and NHEJ.
The heterogeneous response to radiotherapy in HNSCC patients could also be related to the immune system. In general, HNSCC tumors can be categorized as immune-infiltrated “hot” and immune-deserted or immune-excluded “cold” tumors, based on the abundance of immune cell invasion [3]. The “immune-cold” HNSCC tumors generally have a worse prognosis, highlighting the potential benefit of including HNSCC microenvironment characteristics in the treatment response prediction models [4], [5]. Furthermore, several studies suggest that the type of radiation influences HNSCC tumor microenvironment responses, which could also have an effect on the tumor control upon radiotherapy [6], [7].
Existing predictive models for patient-specific radiosensitivity all have important drawbacks. While mouse models and 3D tumor organoids lack the complex patient-specific immune system, sequencing studies often miss the functional validation [8], [10]. To overcome this problem, we have established a motion-based ex vivo tissue slice culture (MOTEX) model using precision cut tumor slices. This model sustains cancer cell and immune cell viability in culture over several days, enabling evaluation of functional treatment response fitting the clinical timeframe [9].
Here, we describe the analysis of HNSCC tissue slices treated with proton and X-ray irradiation to investigate the patient-specific sensitivity to both modalities and elucidate the underlying mechanisms.
Materials and methods
Collection of tumor tissue
Resection material was acquired from HNSCC patients, which were undergoing surgery at the Erasmus University Medical Center (Erasmus MC), The Netherlands, as described previously [9]. Samples were pseudonymized according to the code of proper secondary use of human tissue in the Netherlands established by the Dutch Federation of Medical Scientific Societies, and approved by the Erasmus MC Medical Ethical Committee (number MEC-2017-1049).
Tissue slice culture and irradiation
Tumor tissue processing and culture have been performed as described previously [9], [11]. X-ray irradiation was performed at Erasmus MC in an X-Strahl RS320 X-ray cabinet with 0.5 mm Cu filter at 195 keV with a dose rate of 1.6 Gy/min. Proton irradiation was performed at Holland Proton Therapy Center (HPTC) in the R&D beam line. From a therapeutic pencil beam, a passive scattering system produced a field size of 8 × 8 cm^2^, with dose uniformity of 98% over the whole area, irradiating the whole sample uniformly with a dose rate of 9 Gy/min. To create a Spread-out-Bragg peak (SOBP), a 2D range energy modulator was used with an initial energy of 150 MeV, creating a SOBP of 25 mm with 98% ±1% uniformity [3]. A physical dose of 5 Gy was given (not RBE weighted). Irradiations were performed simultaneously at both locations. Fixation was undertaken at 2 h and 5 days with prior 2-hour EdU incubation (30 μmol/L) [11], [12].
Immunohistochemistry (IHC) and Immunofluorescence (IF)
All IHC stainings were automated by using the Ventana Benchmark ULTRA (Ventana Medical Systems Inc.) as reported previously [11]. IF was done as described previously [9], [13]. In Situ Cell Death Detection Kit (Roche Life Sciences) was used for apoptosis staining (TUNEL) as described [13].
Image acquisition
H&E and CD68 IHC staining (DAB) were visualized using an Olympus BX40 F4 System microscope. CD45 immunohistochemistry staining (DAB) was imaged with a Zeiss Axio Imager II with Axiocam 208 camera. TUNEL staining (at least three fields of view (FoV) per sample) and RAD51 staining (at least 30 Geminin-positive cells per sample) were imaged using a Leica DM4000B fluorescent microscope with a Leica DFC300 FX camera. A Leica Stellaris 5 LIA confocal microscope was used for EdU incorporation (at least three FoV per sample).
Image analysis
To calculate apoptosis levels, nuclei were segmented on the DAPI images and on the TUNEL images using a previously described StartDist module in Python 3.8 [11]. To calculate the proliferation, segmentation of EdU-positive cells was done as described previously [11].
RAD51 foci were analyzed as described previously [9], [13].
For CD45 quantification, all images were analyzed in QuPath with positive cell detection and two separate thresholds (1st hematoxylin for nuclei, 2nd DAB for CD45).
Multiplex immunofluorescence
Multiplex IF analysis was performed by automated IF using the Ventana Benchmark Discovery ULTRA (Ventana Medical Systems Inc.; Supplementary Material and Methods; Supplementary Table 1) [14]. Immune cell numbers were calculated as a percentage relative to the total cell number in the tumor area.
Statistical analysis
Statistical analysis and graph generation were performed using GraphPad Prism 8.0. Statistical differences were tested with Mann Whitney U Test and Kruskal Wallis test with Dunn’s comparison (independent values) or Wilcoxon Test and Friedman Test (dependent values) and p-values < 0.05 were considered significant.
Results
Simultaneous X-ray and proton irradiation in MOTEX culture
HNSCC tissue slices were irradiated either with X-ray, or in the horizontal proton beam as previously described (Supplementary Fig. 1A; [11]). A single dose of 5 Gy was used, as our previous study showed that this dose resulted in the largest heterogeneity in treatment response in HNSCC tumor samples [9]. Morphology of the untreated HNSCC tissue slices was preserved during culture (Supplementary Fig. 1B). Moreover, apoptosis (TUNEL assay) and proliferation (EdU incorporation) were constant for up to five days in culture for the majority of the samples (Supplementary Fig. 1C-F). Two samples increased in apoptosis by more than 10% in the absence of treatment and were therefore excluded from analysis (Supplementary Fig. 1G-H). Treatment outcome in the remaining samples showed on average decreased proliferation and increased apoptosis after both X-ray and proton irradiation after 5 days in culture, although only apoptosis induction after proton irradiation reached statistical significance (Fig. 1A–F).Fig. 1Ex vivo proliferation and apoptosis assays. (A) Representative confocal microscopy images of Edu incorporation of untreated control, 5 Gy X-ray and 5 Gy proton irradiated samples after 2 h and 5 days of culture (blue = DAPI for nuclei, green = p63, red = EdU; not RBE corrected). (B) Representative images of TUNEL staining of untreated control, 5 Gy X-ray and 5 Gy proton irradiated samples after 2 h and 5 days of culture (blue = DAPI for nuclei, green = TUNEL). (C) Percentage of proliferating cells in untreated control at the beginning of culture (2 h) and after 5 days of culture. (D) Percentage of apoptotic cells cells in untreated control at the beginning of culture (2 h) and after 5 days of culture. (E) Percentage of proliferating cells per treatment condition. (F) Percentage of apoptotic cells per treatment condition. Bar graphs represent mean of all samples (≥3 FoV per sample), and error bars depict SEM. Wilcoxon test (C, D) and Friedman test (E, F) were used for significance (paired values). *p < 0.05. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
Identification of HNSCC samples specifically sensitive to proton irradiation
Next, we investigated whether there was a differential response to proton and X-ray irradiation in the individual HNSCC tumors. We compared the effect of X-ray and proton irradiation on tissue slices from the same tumor. For 5 samples, more than one individual slice of the same tumor was used per condition. Given no statistically significant differences in the percentage of EdU and TUNEL-positive cells between the individual slices in the majority of the samples (Supplementary Fig. 2), the FoV from the individual slices were pooled for further analysis.
While the effects of both treatment modalities were comparable for most samples (n = 5), three tumors displayed a significantly larger decrease in proliferation upon proton than X-ray irradiation (Fig. 2A and B; Supplementary Fig. 3A). Moreover, two of these samples displayed markedly higher apoptosis levels upon proton irradiation (OC82, OC65; Fig. 2C and D; Supplementary Fig. 3B) Interestingly, one sample showed more severely decreased proliferation and increased apoptosis levels upon X-ray irradiation (OC81; Fig. 2A–D; Supplementary Fig. 3A and B). Overall, we found a positive correlation between the two measures of an increased proton sensitivity: the samples with the highest relative decrease of proliferation after proton irradiation displayed also the highest relative induction of apoptosis (R^2^ = 0.76; p = 0.0022, Fig. 2E).Fig. 2. Comparison of X-ray and proton sensitivity. (A) Proliferation per sample relative to untreated control after X-ray or proton irradiation. (B) Difference in proliferation decrease upon proton or X-ray irradiation; decrease in proliferation was calculated relative to the experiment-specific control, followed by subtraction of the X-ray value from the proton value. Significance was calculated by directly comparing X-ray and proton irradiated samples. Sample numbers are displayed from high to low proton sensitivity. (C) Apoptosis induction (in percentage of apoptotic cells) per treatment condition, relative to untreated control. (D) Difference in apoptosis induction between proton and X-ray irradiation; experiment-specific control was subtracted from the irradiated condition, followed by subtraction of X-ray value from proton value. Significance was calculated by directly comparing X-ray and proton irradiated samples. Sample numbers are ordered from high to low proton sensitivity. (E) Correlation between the relative decrease of proliferation after proton irradiation (y-axis) and the relative induction of apoptosis after proton irradiation (x-axis). Bar graphs represent mean of all samples (≥3 FoV per sample; A,B,C,D), and error bars depict SEM (B,D). Kruskal-Wallis test with Dunn’s comparison was used for significance. *p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001.
The HR-deficient sample displayed an increased proton radiation sensitivity ex vivo
We did not find a clear difference in the patient characteristics between proton- or X-ray sensitive HNSCC tumors (Supplementary Table 2). Therefore, the observed heterogeneity in the ex vivo treatment response points to tumor-intrinsic determinants, such as differences in the activity of DNA damage repair pathways. Studies suggest that the repair of proton-induced DNA damage is relatively more dependent on the HR DNA damage repair pathway [15], [16]. Therefore, we employed the REpair CAPacity (RECAP) assay to measure HR proficiency by quantifying RAD51 foci formation ([17] and Fig. 3A). Notably, only the proton-sensitive HNSCC sample OC65 was HR-deficient, while all the remaining samples were HR-proficient (Fig. 3B and C).Fig. 3HR proficiency analysis. (A, B) Representative fluorescent images of RAD51 DNA damage foci of 5 Gy X-ray irradiated samples after 2 h for HR proficient (A) and HR deficient (B) sample (blue = DAPI for nuclei, green = geminin for cell cycle, red = RAD51). (C) RAD51 foci quantification two hours after irradiation. Geminin-positive cells were counted RAD51-positive when ≥ 5 RAD51 foci were present per nucleus. Samples were classified as proficient (above 50%), intermediate (20–50%) and deficient (under 20%). All bar graphs represent % of geminin positive cells (n ≥ 30) with 5 or more RAD51 foci. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
HNSCC immune cell infiltration correlates with radiosensitivity ex vivo
Further, we investigated whether differences in the immune cell infiltration could explain the heterogenous ex vivo proton and X-ray sensitivity. CD45 was used as a general marker for leukocytes and CD68 as macrophage marker. The X-ray radiosensitive sample OC81 displayed relatively high immune cell levels, while two of proton radiosensitive samples showed low levels of immune cell infiltration (OC82; OC62; Fig. 4A; Supplementary Fig. 4A).Fig. 4. Immune cell infiltration and radiosensitivity ex vivo. (A) Representative brightfield microscopy image of immunohistochemistry staining (Blue (Hematoxylin = Nuclei, brown (DAB) = CD45 or CD68). (B) Representative fluorescent microscopy image of multiplex staining. (C-D) Correlation plots comparing immune cell infiltration to proliferation values after X-ray vs. proton irradiation for CD68 (general macrophages; C) and CD4 (T-helper cells; D). (E) Correlation plot for CD4/CD8 values. (F) Correlation plots for CD8 (cytotoxic T-cells). (G) Correlation plots comparing combined immune cell infiltration (CD68, CD4, CD8). Goodness of fit is displayed as R squared. Proton sensitive samples are marked in red (OC62, OC82), X-ray sensitive sample is marked in blue (OC81). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
To further define which immune cells could possibly explain the observed radiosensitivity, we performed multiplex staining detecting T-helper cells (CD4), cytotoxic T-cells (CD8), and macrophages (CD68), specifically M2 (tumor associated) macrophages (CD163; Fig. 4B). P63-positive areas were selected to directly define immune infiltration into tumor areas (Supplementary Fig. 4B; [18]). General macrophages (CD68+), T-helper cells (CD4+), the CD4+/CD8+ratio, as well as combined immune cells (CD68+, CD4+, CD8+) in tumor areas correlated with the treatment outcome ex vivo, with higher immune cell infiltration detected in the samples that were relatively more sensitive to X-ray irradiation (Fig. 4C–E and G; Supplementary Fig. 4C–E and I). This correlation was not observed for M2 macrophages or cytotoxic T-cells (Fig. 4 F; Supplementary Fig. 4F–H).
The X-ray radiosensitive sample OC81 showed high immune cell infiltration and the proton radiosensitive samples OC62 and OC82 lacked immune cells in the tumor area. However, the proton radiosensitive sample OC65, that was HR-deficient, did not show the same trend. Moreover, not all immune cell low tumors showed an increased proton radiosensitivity (e.g. OC64; Fig. 5A). All three proton radiosensitive samples displayed a low CD4+/CD8+ T-cell ratio (Fig. 5B).Fig. 5HNSCC microenvironment composition and HR deficiency correlate with radiosensitivity ex vivo (A) Schematic representation of tumor sensitivity, HR deficiency (RAD51 foci formation), and immune cell infiltration. For tumor cell sensitivity (based on proliferation (EdU, first column) and apoptosis (TUNEL, second column)), the relatively proton sensitive samples are depicted in red, the relatively X-ray sensitive sample in blue and the rest in yellow. The RAD51 foci deficient (HRD) sample is depicted in red and the relative level of immune cell infiltration as a gradient from low (blue) to high (yellow). (B) Immune cell infiltration per cell type (blue = low, yellow = high). Samples have been ordered from relatively high to low proton sensitivity based on proliferation (EdU incorporation) results. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
To conclude, we found in this limited sample set that immune cell infiltration correlated stronger to the general increased radiation response than to the specific proton radiosensitivity (Supplementary Fig. 3J–S).
Discussion
HNSCC patient response to radiotherapy treatment is heterogeneous and cannot be explained by clinical factors only. In this study, we employed an ex vivo radiosensitivity assay to compare response of individual HNSCC tumors to proton and X-ray irradiation. We assessed the radiation response by combining proliferation and apoptosis assays, which have been described in literature as possible predictive assays for radiosensitivity [19], [20]. Three samples exhibited specifically increased sensitivity to protons, as compared to X-rays. One of the relatively more proton-sensitive samples was HR deficient and the other two showed very low immune infiltration, suggesting that these two parameters could determine the differential sensitivity.
For the comparison of proton and X-ray effects, a single dose of 5 Gy irradiation was used in the experimental setup. We have previously seen that at higher radiation doses (7 Gy and 10 Gy) the vast majority of HNSCC samples showed a very strong decrease in proliferation and therefore we reasoned that at those radiation doses any added effect of proton treatment would be lost. At 5 Gy we previously found the largest heterogeneity in response to X-ray irradiation and anticipated that this dose would be most suited to detect an increased sensitivity to protons in otherwise less (X-ray) responsive samples [9]. Indeed, three tumors specifically more sensitive to proton irradiation were detected (Fig. 2A).
We found a good concordance between a relative proliferation decrease and apoptosis induction after proton irradiation as compared with X-ray irradiation. However, the level of apoptosis after treatment, except for one proton-sensitive sample, remained low, consistent with previous observations [9]. Due to the previously observed large heterogeneity in the therapy response between individual HNSCC tumors, all samples were included in the analysis, even if they could be interpreted as outliers. When the one proton-sensitive sample with high apoptosis levels was excluded, the analysis still showed statistically significant increase of apoptosis after proton irradiation (p = 0.0485), Importantly, all the analyzed samples consistently displayed low level of apoptosis in the untreated condition after 5 days of culture. The optimal assay, or combination of assays, for determining radiosensitivity will require a larger clinical validation study. For X-ray irradiation, this is currently addressed in a prospective clinical study [21].
One of the samples with increased proton sensitivity ex vivo was HR deficient, in agreement with the hypothesis that the HR pathway is specifically required for repair of DNA damage induced by proton irradiation [15], [16], [22]. This has previously been suggested based on the increased proton sensitivity of HR deficient cell lines [23], [24], and our results in primary HNSCC tissue support this conclusion. The proton hypersensitivity of HR deficient cells and tumors may be the consequence of more clustered damage after proton irradiation, which may pose specific problems to DSB repair. This effect may be more pronounced at the distal end of the Bragg peak (where LET is higher) than in the SOBP, which would create heterogeneous responses throughout HR deficient tumors. More careful investigation will be necessary to address this issue directly in the proton-irradiated patients. Functional HR deficiency screening could identify patients that would specifically benefit from proton treatment. However, in our current and previously published cohort of HNSCC tumors the HR deficiency prevalence was low (<5%) [9], making this approach less relevant for the clinical practice.
Two of the X-ray resistant samples had very low immune cell infiltration, and the sample that was the most radiosensitive in general had high immune cell infiltration. According to the classification by Su et al. [25] this sample would most likely be categorized as immunoactive (type 1). This positive effect of an increased immune cell infiltration on X-rays sensitivity of tumors has been described previously [12], [26]. Conversely, several studies found that tumors with low immune cell infiltration showed increased radioresistance [25], [27]. Two out of three immunodeserted samples responded to protons, but not X-rays in our assay, suggesting that proton radiotherapy could be a better alternative for these patients. We are currently investigating whether a similar X-ray radioresistant effect is observed for the deserted immune type in an extended cohort of oropharyngeal squamous cell carcinoma (OPSCC) patients [21].
In our dataset, CD4+ T-helper cells as well as CD4+/CD8+ ratio seemed to be the most indicative of low ex vivo X-ray sensitivity. Low CD4+ T-helper cell infiltration has also been found to correlate with poor overall survival in HNSCC patients [28]. A low CD4+/CD8+ ratio has been shown to correlate in both cervical cancer and triple negative breast cancer with a worse 5-year survival rate [26], [29]. In the cervical cancer, both low CD4+/CD8+ ratio and low CD4+ T-helper cell infiltration correlated with an increase chance of patient’s death [29]. Although these immune parameters can be used to describe the response of a population, they do not appear to be sufficient to predict radiation responses of individual patients. Therefore, a functional assay may be crucial to define radioresistant patients on an individual level.
Most other ex vivo assays are costly and require extended culture time, making them less suitable for the clinical workflow [23], [24], [30]. Our MOTEX assay provides a rapid read-out of radiation response in less than 10 days, compatible with the clinical diagnostic timeframe. Moreover, the use of the complete tumor tissue preserves all cell types of the patient-specific tumor microenvironment, which appears to be specifically important for the sensitivity measurements that are dependent on immune components, such as X-ray sensitivity. However, there are also limitations to this assay. First, a minority of samples did not survive the experimental procedures optimally, which may be related to periods on ice and transport for irradiation at different locations (Erasmus MC and Holland PTC). Second, small differences between the experimental conditions at both locations (e.g. different incubators) cannot be excluded. Both issues could be solved by culturing and irradiating the tissue specimen with both X-rays and protons exclusively at the proton center. Through this change, diagnostic biopsy studies with smaller tissue specimens would become feasible.
In summary, our radiosensitivity assay was able to identify HNSCC samples that were specifically sensitive to proton irradiation, although the findings need to be confirmed in a larger group of patients. We are currently optimizing this assay for smaller tissue samples, which paves the way for the clinical studies, that would use biopsy material from a primary HNSCC tumor to predict specific radiosensitivity to protons ex vivo. After validation in a clinical study, this assay could be of value not only for personalized radiotherapy, but also as a platform for testing novel combination therapies.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Erasmus MC (protocol code MEC-2017-1049 (2017)).
Informed consent statement
Patient consent was waived for surgical material due to laws in the Netherlands for opting out. All use of human material was approved by the Erasmus MC Medical Ethics Commission.
CRediT authorship contribution statement
Katrin S. Pachler: Data curation, Investigation, Writing – original draft. Iris Lauwers: Formal analysis, Visualization. Nicole S. Verkaik: Data curation, Investigation. Marta Rovituso: Resources, Writing – review & editing. Hetty Mast: Resources, Writing – review & editing. Brend P. Jonker: Resources, Writing – review & editing. Bernd Kremer: Resources, Writing – review & editing. Sjors A. Koppes: Resources, Writing – review & editing. Thierry P.P. van den Bosch: Resources, Writing – review & editing. Gerda M. Verduijn: Writing – review & editing. Steven Petit: Writing – review & editing. Brita S. Sørensen: Writing – review & editing. Dik C. van Gent: Conceptualization, Methodology, Project administration. Marta E. Capala: Conceptualization, Methodology, Project administration.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Dr. Marta Capala has received consulting fees for consultancy for GE Healthcare on behalf of the Department of Radiotherapy, Erasmus Medical Center Rotterdam, though not related to the research described in the manuscript.
Prof. Brita Singers Sørensen is an Editorial Board Member with Radiotherapy and Oncology and was not involved in the editorial review or the decision to publish this article.
Erasmus MC Cancer Institute has research collaborations with Accuray Inc., Sunnyvale, USA, Elekta AB, Stockholm, Sweden and with Varian, a Siemens Healthineers Company (Palo Alto, CA, USA).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fiedler M.Infiltrating immune cells are associated with radiosensitivity and favorable survival in head and neck cancer treated with definitive radiotherapy Oral Surg Oral Med Oral Pathol Oral Radiol 129620206126203240919110.1016/j.oooo.2020.02.010 · doi ↗ · pubmed ↗
- 2Nicole G.Deficiency in homologous recombination renders mammalian cells more sensitive to proton versus photon irradiation Int. J. Rad. Oncol. Biol. Phys.881201417518110.1016/j.ijrobp.2013.09.04124239385 · doi ↗ · pubmed ↗
- 3Wu B.Cold and hot tumors: from molecular mechanisms to targeted therapy Signal Transduct Target Ther 9120242743942020310.1038/s 41392-024-01979-x PMC 11491057 · doi ↗ · pubmed ↗
- 4Ribbat-Idel J.Immunologic “cold” squamous cell carcinomas of the head and neck are associated with an unfavorable prognosis Front Med (Lausanne)8202162233010.3389/fmed.2021.622330 PMC 787359733585526 · doi ↗ · pubmed ↗
- 5Knitz M.W.Targeting resistance to radiation-immunotherapy in cold HNSC Cs by modulating the Treg-dendritic cell axis J Immunother Cancer 94202110.1136/jitc-2020-001955 PMC 806182733883256 · doi ↗ · pubmed ↗
- 6Chimote A.A.Proton treatment suppresses exosome production in head and neck squamous cell carcinoma Cancers (Basel)16202410.3390/cancers 16051008 PMC 1093100538473367 · doi ↗ · pubmed ↗
- 7Lupu-Plesu M.Effects of proton versus photon irradiation on (lymph)angiogenic, inflammatory, proliferative and anti-tumor immune responses in head and neck squamous cell carcinoma Oncogenesis 672017 e 3542867167710.1038/oncsis.2017.56PMC 5541708 · doi ↗ · pubmed ↗
- 8Kürten C.H.L.Investigating immune and non-immune cell interactions in head and neck tumors by single-cell RNA sequencing Nat Commun 121202173383492114310.1038/s 41467-021-27619-4PMC 8683505 · doi ↗ · pubmed ↗