Depression, anxiety, burnout, and substance use disorders among auto workers and COVID-19 as a stressor in Mexico
Raúl A. Gutiérrez García, Abraham Sánchez Ruiz, Antonio de Jesús Serrano Carrera, Nancy Alejandra Vaca Rico, Mónica Natalia Arteaga Tovar, María Alicia Zavala Berbena, Marco Antonio Escobar Acevedo, María Abigail Paz Pérez, Kalina Isela Martínez Martínez

TL;DR
The study shows that the COVID-19 pandemic significantly worsened mental health among Mexican auto workers, with high rates of depression, anxiety, burnout, and substance use.
Contribution
This study is novel in examining the mental health impact of the pandemic on industrial workers in Mexico, linking specific stressors to psychiatric outcomes.
Findings
30.5% of workers experienced burnout, 29.3% anxiety, 24.3% depression, and 13.9% substance use problems.
Workers exposed to COVID-19 stressors were more likely to have comorbid anxiety, depression, and burnout.
Only 25.3% of workers with mental health symptoms had received treatment despite 74.8% feeling supported by their company.
Abstract
The COVID-19 pandemic intensified psychosocial risks, exposing vulnerabilities in labor conditions. Findings aim to inform mental health interventions and workplace policies tailored to industrial workers in post-pandemic settings. We evaluated the prevalence of occupational stress and associated psychiatric problems, including anxiety, depression, substance use disorders, and burnout among automotive workers, examining COVID-19 as a significant stressor. Participants were workers in the automotive industry (N = 1,020) from two manufacturing plants in Guanajuato, Mexico. We assessed four mental health outcomes: depression, anxiety, substance use disorders, and burnout, using validated instruments. Multinomial logistic regression was used to examine the associations between COVID-19 stressors and mental health symptoms, while adjusting for sociodemographic characteristics. Prevalence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
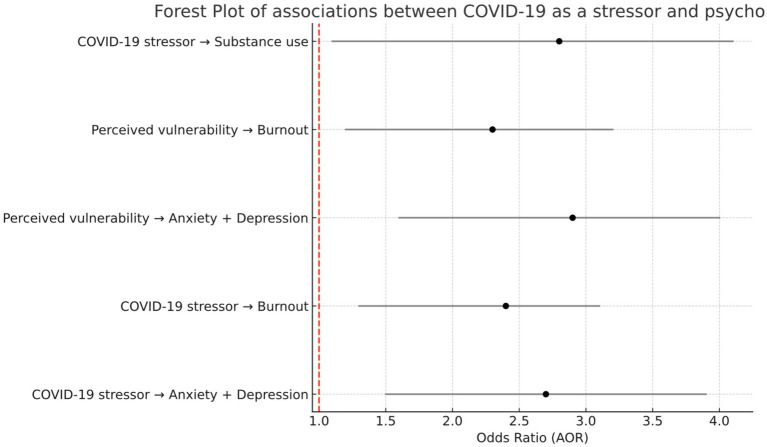 Figure 1
Figure 1| Characteristic | |
|---|---|
| Age (years) | 30.4 (1.01) |
| Age groups | |
| 18–24 | 306 (30.1) |
| 25–34 | 357 (35.9) |
| 35–44 | 204 (20.3) |
| 45+ | 153 (15.6) |
| Gender | |
| Male | 593 (58.1) |
| Female | 427 (41.9) |
| Sexual orientation | |
| Heterosexual | 977 (95.7) |
| Other | 43 (4.3) |
| Marital status | |
| Married/Cohabitating | 113 (51.1) |
| Single | 285 (39.1) |
| Separated/Divorced/Widowed | 102 (9.8) |
| Has children | |
| Yes | 581 (57.4) |
| No | 439 (43.6) |
| Education level | |
| High school or less | 398 (39.8) |
| Technical training | 337 (33.9) |
| Bachelor’s degree or higher | 173 (17.9) |
| Mental health indicators | Mean (SD) |
| Depression (PHQ-9) | 24.27 (6.34) |
| Anxiety (GAD-7) | 29.31 (4.23) |
| Burnout (MBI) | 30.53 (5.56) |
| Substance use (ASSIST) | 19.93 (7.28) |
| COVID-19 stress (IES-R) | 34.19 (6.11) |
| Variable | Total (%) | San Francisco (%) | Irapuato (%) | |
|---|---|---|---|---|
| Work-related traumatic stress (COVID-19 event) | 34.2 | 37.7 | 31.7 | 0.012 |
| Work-related stress symptoms (MBI) | 30.5 | 33.1 | 27.8 | <0.001 |
| Anxiety symptoms (GAD-7) | 29.3 | 30.1 | 28.4 | <0.001 |
| Depressive symptoms (PHQ-9) | 24.3 | 23.5 | 25.1 | <0.001 |
| Variable | Total (%) | San Francisco (%) | Irapuato (%) | |
|---|---|---|---|---|
| Substance use problems (ASSIST) | 13.9 | 15.1 | 12.8 | <0.001 |
| Exposure to violence (lifetime) | 62.7 | 66.0 | 62.4 | <0.001 |
| Received mental health treatment (past 12 months) | 25.3 | 22.9 | 27.7 | <0.001 |
| Feels supported by company to seek help | 74.8 | 72.2 | 77.3 | 0.004 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Workplace Health and Well-being · Employment and Welfare Studies
Introduction
1
Manufacturing workers globally face elevated mental health risks due to unique occupational stressors including shift work, repetitive tasks, production pressures, and physical demands (1, 2). The global automotive industry employs approximately 10 million workers directly and 50 million indirectly (3), with significant regional concentrations: the European Union employs 13.8 million across the automotive value chain (4), while Mexico’s transport equipment sector has grown to 1.3 million workers, representing 20% of national manufacturing employment and 20% of North American vehicle production (5), represents a critical yet understudied population for mental health research (6, 7). Recent evidence from multiple countries demonstrates concerning mental health prevalence rates among automotive workers: Iranian automotive workers showed 22.6% depression, 24% anxiety, and 29.3% stress symptoms, with 66.7% experiencing high occupational stress (6); Malaysian automotive workers reported mild to severe depression (9.9% severe), anxiety (18.7% severe), and stress symptoms (8); Chinese manufacturing workers demonstrated 25%–30% psychological distress (9); while Vietnamese industrial workers reported 22% depression rates (10).
The Job Demands-Resources model (11) and the psychosocial safety climate framework (12–14) provide theoretical grounding for understanding how workplace factors influence mental health outcomes. In automotive settings specifically, the interaction between high job demands, limited autonomy, and safety pressures creates unique stressors affecting psychological well-being (15, 16). Despite growing recognition of these challenges, evidence-based workplace mental health interventions remain limited (17–19). Barriers include stigma, limited workplace support, cost, and service accessibility (20, 21). Understanding these barriers within specific cultural and organizational contexts is essential for developing effective interventions.
The COVID-19 pandemic fundamentally altered occupational mental health landscapes globally (22, 23). Essential workers, including automotive manufacturing employees who continued on-site work, faced compound stressors: infection risk, job insecurity, and work-family conflict (24–26). Studies across multiple sectors document significant mental health impacts, with healthcare workers showing 30%–40% anxiety/depression rates (27, 28) and industrial workers experiencing similar elevations (29). The pandemic’s prolonged nature created sustained psychological pressure, with evidence of cumulative mental health deterioration across successive waves (30, 31).
In Latin America, only 25% of those with mental disorders receive treatment (32). It has been found that more than 20% of people in Mexico have at least one mental disorder, one in four will suffer from it at least once in their lifetime in the following years (33, 34). This number is expected to increase as a result of COVID-19 (35).
Mexico’s automotive industry, the world’s seventh-largest producer, employs over 900,000 workers (36). The Bajío region, particularly Guanajuato state, represents Mexico’s automotive manufacturing hub. This workforce faces unique challenges: existing mental health service gaps (37, 38), regional violence concerns (39), and recent regulatory changes through NOM-035-STPS-2018 mandating psychosocial risk assessment (40). Mexican healthcare workers during COVID-19 showed elevated mental health impacts (41), yet automotive workers’ experiences remain undocumented.
This study addresses critical gaps by: (1) establishing mental health prevalence (depression, anxiety, burnout, substance use) among Mexican automotive workers; (2) examining COVID-19 as a specific occupational stressor using validated instruments; (3) identifying treatment-seeking patterns and barriers; and (4) comparing outcomes between manufacturing sites. Our findings contribute to global understanding of pandemic impacts on essential manufacturing workers while informing evidence-based interventions for this vulnerable population. Results have implications for international occupational health policy and practice, particularly in emerging economies, balancing industrial growth with worker wellbeing.
Materials and methods
2
This study investigated the prevalence and correlates of mental health symptoms among automotive manufacturing workers during the COVID-19 pandemic, with particular focus on depression, anxiety, burnout, and substance use patterns. The research employed validated psychometric instruments to assess mental health outcomes and examined the role of pandemic-related stressors as potential risk factors within this essential worker population.
Study design
2.1
This cross-sectional study was conducted between July and November 2022 to assess mental health prevalence and associated factors among automotive manufacturing workers in Guanajuato, Mexico. The research protocol adhered to the Declaration of Helsinki ethical principles. The personal information, classified as sensitive by the Federal Law for the Protection of Personal Data in the Possession of Private Parties, was treated confidentially.
Participants and recruitment
2.2
The total workforce population of approximately 7,000 employees across both facilities, we calculated a required sample size of 1,020 participants to achieve 95% confidence level with a 2.837% margin of error. Recruitment employed a multi-modal approach combining institutional email invitations and in-person recruitment sessions conducted by human resources and occupational health personnel. Although 1,119 workers were invited, 101 decided not to participate.
The inclusion criteria comprised (1) a minimum age of 18 years, (2) current employment in either manufacturing facility, and (3) voluntary informed consent. The exclusion criteria consisted of temporary contractors and individuals on medical or administrative leave during the data collection period. The final analytical sample consisted of 1,020 participants, representing a response rate of 91.1% of the target sample.
Data collection procedures
2.3
Data collection utilized a self-administered online survey deployed through QuestionPro® platform. The survey incorporated adaptive questioning logic to minimize completion time while maintaining comprehensive assessment coverage. Prior to full deployment, the instrument underwent pilot testing with 30 workers to assess comprehension, technical functionality, and completion time.
Participants received unique, anonymized access codes ensuring confidentiality while preventing duplicate responses. The survey remained accessible 24/7 during the collection period to accommodate varying work shifts. Automated reminder emails were sent at 7 and 14 days to non-responders. All responses were encrypted and stored on secure servers compliant with institutional data protection protocols.
Measures
2.4
The comprehensive assessment battery included internationally validated instruments adapted and validated for Mexican Spanish-speaking populations:
Depression assessment
2.4.1
The Patient Health Questionnaire-9 (PHQ-9) measured depressive symptom severity over the preceding 2 weeks (42). Items are scored 0–3, yielding total scores ranging 0–27, with established cutoffs: minimal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe (20–27) depression. Internal consistency in this sample was excellent (Cronbach’s α = 0.83).
Anxiety assessment
2.4.2
The Generalized Anxiety Disorder-7 (GAD-7) scale evaluated anxiety symptoms, including nervousness, restlessness, and catastrophic thinking (43). The instrument demonstrated high internal consistency (α = 0.92) with validated cutoffs: minimal (0–4), mild (5–9), moderate (10–14), and severe (≥15) anxiety.
Burnout syndrome
2.4.3
The Maslach Burnout Inventory (MBI) assessed three dimensions of occupational burnout (44): emotional exhaustion (9 items, α = 0.837), depersonalization (5 items, α = 0.869), and personal accomplishment (8 items, α = 0.881). Dimensional scores were calculated following standardized protocols with normative comparisons for manufacturing workers. Burnout was defined as high emotional exhaustion (≥27), high depersonalization (≥10), and low personal accomplishment (≤33).
Substance use screening
2.4.4
The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) evaluated lifetime and past three-month use patterns for 10 substance categories (45). Risk scores were categorized as low (0–3), moderate (4–26), or high (≥27) for alcohol, and adjusted thresholds for other substances per WHO guidelines.
COVID-19 stress impact
2.4.5
The Impact of Event Scale-Revised (IES-R) measured pandemic-related traumatic stress across three domains: intrusion (8 items), avoidance (8 items), and hyperarousal (6 items) (46). Items were rated 0–4 regarding distress intensity during the previous week, with subscale scores indicating subclinical (<33) or probable PTSD (≥33) symptomatology.
Sociodemographic and occupational variables
2.4.6
Structured questions assessed age, gender, education, marital status, job position (production line, technical, administrative), shift schedule, tenure, and COVID-19 exposure history, including personal infection, family losses, and vaccination status.
Statistical analysis
2.5
Data analysis employed SPSS version 25.0 (IBM Corp., Armonk, NY). Descriptive statistics characterized the sample demographics and prevalence rates with 95% confidence intervals. Internal consistency was verified using Cronbach’s alpha, with values ≥0.70 considered acceptable.
Bivariate analyses examined associations between mental health outcomes and potential risk factors using Chi-square tests for categorical variables and Student’s t-test for continuous variables. The Kolmogorov–Smirnov normality test was performed for all quantitative variables included in the analyses. In all cases, the p-values were greater than 0.05, indicating that the null hypothesis of normality is not rejected. Multinomial logistic regression was used to analyze the associations between COVID-19 stressors and different profiles of psychological distress. The reference category was the absence of clinically significant symptoms. The final model included the following covariates: age, sex, educational level, presence of medical comorbidities, exposure to COVID-19-related stressors, and perception of vulnerability, adjusting for sociodemographic covariates identified as significant (p < 0.10) in bivariate analyses.
Model assumptions were verified including multicollinearity assessment (VIF < 5), and goodness-of-fit evaluated using Hosmer-Lemeshow tests. Adjusted odds ratios (AOR) with 95% confidence intervals were calculated. Statistical significance was set at p < 0.05 for all analyses. Missing data patterns were examined, with complete case analysis employed given <5% missingness across variables.
Results
3
Sample characteristics
3.1
The final sample comprised 1,020 automotive manufacturing workers from two plants in Guanajuato, Mexico: Irapuato (n = 607, 59.5%) and San Francisco del Rincón (n = 413, 40.5%). Participants had a mean age of 30.4 years (SD = 10.1), with 58.1% identifying as male (n = 593) and 41.9% as female (n = 427). The majority (51.0%, n = 520) were married or in domestic partnerships, 39.0% (n = 398) were single, and 10.0% (n = 102) were separated, divorced, or widowed. Educational attainment varied, with 39.0% (n = 398) completing high school, 33.0% (n = 337) technical training, and 17.0% (n = 173) holding undergraduate or postgraduate degrees. Over half (57.0%, n = 581) reported having children (mean = 2.8 children). Regarding occupational characteristics, 56.0% (n = 571) worked as direct production workers, 32.0% (n = 326) in indirect/operational support roles, and 12.0% (n = 122) in administrative positions. The production department employed 77.0% (n = 785) of participants, with the remaining workers distributed across quality control, human resources, logistics, and other departments. Half worked morning shifts (50.0%, n = 510), 42.0% (n = 428) afternoon shifts, and 8.0% (n = 82) rotating schedules. Complete demographic and baseline mental health scores are presented in Table 1.
Mental health prevalence
3.2
Mental health symptoms were prevalent across the sample, with 34.2% experiencing COVID-19–related traumatic stress symptoms were prevalent across the sample, with 34.2% (n = 349) experiencing clinically significant symptoms based on IES-R scores ≥33. Burnout affected 30.5% (n = 311) of workers, with emotional exhaustion being the predominant dimension. Anxiety symptoms (GAD-7 ≥ 10) were present in 29.3% (n = 299) of participants, while 24.3% (n = 248) met criteria for moderate to severe depression (PHQ-9 ≥ 10). Substance use problems, assessed via ASSIST, were identified in 13.9% (n = 142) of workers, primarily involving tobacco (38.0% lifetime use, n = 388) and alcohol (73.0% lifetime use, n = 745).
Between-plant comparisons
3.3
Significant differences emerged between manufacturing sites Student’s t-test (Table 2). Workers from San Francisco del Rincón reported a higher prevalence of COVID-19–related traumatic stress symptoms (37.7%, n = 156) compared to those from Irapuato (31.7%, n = 192) (p = 0.012). Similarly, work-related burnout was more common in San Francisco (33.1%, n = 137) than in Irapuato (27.8%, n = 169) (p < 0.001). Anxiety prevalence was comparable between sites, with 30.1% (n = 124) in San Francisco and 28.4% (n = 172) in Irapuato (p < 0.001). In contrast, depression symptoms showed a slightly higher prevalence in Irapuato (25.1%, n = 152) compared to San Francisco (23.5%, n = 97) (p < 0.001).
Risk factors and help-seeking patterns
3.4
Lifetime violence exposure was reported by 62.7% (n = 640) of participants, with higher rates in San Francisco del Rincón (66.0%, n = 273) compared to Irapuato (62.4%, n = 379) (p < 0.001; Table 3). Despite high symptom prevalence, only 25.3% (n = 258) had accessed mental health services in the past year, with Irapuato workers showing higher utilization (27.7%, n = 168) compared to San Francisco (22.9%, n = 95) (p < 0.001). Notably, 74.8% (n = 763) felt their employer would support help-seeking, though this perception was stronger among workers in Irapuato (77.3%, n = 469) than in San Francisco (72.2%, n = 298) (p = 0.004), with Student’s t-test.
COVID-19 stressor associations
3.5
Multinomial logistic regression revealed that COVID-19 stressors significantly increased odds of comorbid mental health symptoms (Figure 1). Workers experiencing pandemic-related stressors had 2.65 times higher odds (95% CI: 1.26–3.26) of concurrent anxiety and depression compared to those without such stressors. Feeling vulnerable to COVID-19 infection showed the strongest association, with 3.34 times higher odds (95% CI: 2.17–4.06) of multiple mental health symptoms after adjusting for sociodemographic factors.
Forest plot of adjusted odds ratio (AOR) and 95% confidence intervals associated with COVID-19 stressors among automotive workers.
Barriers to mental health services
3.6
Primary barriers to seeking professional help included wanting to handle problems independently (mean importance = 1.98), preference for informal support (2.18), cost concerns (2.25), administrative obstacles (2.11), sociocultural stigma (2.81), and fear of job repercussions (2.61). These barriers persisted despite three-quarters of workers perceiving organizational support for mental health help-seeking.
Discussion
4
This study documents a substantial mental health burden among Mexican automotive workers during the COVID-19 pandemic, with prevalence rates of 34.2% for work-related stress (n = 349), 30.5% for burnout (n = 311), 29.3% for anxiety (n = 299), and 24.3% for depression (n = 248).
These findings contribute to the limited but growing body of research examining pandemic impacts on industrial workers who maintained essential production while facing unique occupational and psychosocial stressors, warranting urgent attention from both occupational health and public health perspectives.
Significant differences emerged between manufacturing sites despite shared corporate policies and regional location. San Francisco workers showed higher COVID-19-related stress (37.7% vs. 31.7%, p = 0.012) and burnout (33.1% vs. 27.8%, p < 0.001) compared to Irapuato, yet paradoxically reported lower mental health service utilization (22.9% vs. 27.7%, p < 0.001) and perceived organizational support (72.2% vs. 77.3%, p = 0.004). These variations suggest local workplace cultures, community factors, or workforce composition significantly influence both mental health outcomes and help-seeking behaviors, highlighting that one-size-fits-all interventions may be insufficient even within the same company.
Perhaps our most concerning finding is the disconnect between perceived support and actual help-seeking behavior. While 74.8% of workers reported feeling supported by their company to seek psychological help, only 25.3% had accessed mental health services in the past year, despite approximately one-third reporting clinically significant symptoms. The primary barriers identified, desire for self-reliance (1.98), preference for informal support (2.18), and fear of job repercussions (2.61), reflect deeply embedded cultural and structural factors that organizational support alone cannot overcome.
Principal findings and international comparisons
4.1
Our depression prevalence (24.3%) closely parallels findings from U.S. automotive workers [22.3%; (29)] but falls below rates reported among U.S. essential workers more broadly, where 74%–78% reported anxiety or depression symptoms (47). The anxiety prevalence in our sample (29.3%) exceeds that reported in U.S. automotive workers [23.6%; (29)] but is substantially lower than the combined anxiety/depression rates in Brazilian and Spanish essential workers, where 27.4% experienced both conditions and 11.6% anxiety alone (24). Notably, De Boni et al. found that Brazilian essential workers had significantly higher odds of depression (AOR 2.89), anxiety (AOR 2.81), and comorbidity (AOR 5.99) compared to Spanish workers, suggesting that socioeconomic inequalities in middle-income countries may exacerbate pandemic mental health impacts.
The burnout rate of 30.5% in our sample significantly exceeds that reported among New Zealand essential workers post-lockdown [14%, (48)], though direct comparison is complicated by different measurement approaches and timing. Indian automotive workers also experienced substantial psychosocial impacts during COVID-19, with job anxiety emerging as a three-dimensional construct encompassing stimuli-related, socially-related, and health-related stressors (49). Finnish workers showed fluctuating COVID-19 anxiety across pandemic waves, with the highest levels during lockdown periods (50), highlighting the temporal dynamics of pandemic-related distress.
The global framework synthesis by Sheridan Rains et al. (51), analyzing data from 28 countries, documented widespread deterioration in mental health symptoms and service access challenges during early pandemic phases, consistent with our findings. The International Labour Office (52) further confirmed differential pandemic impacts across worker categories and regions, with essential workers in developing economies facing compounded vulnerabilities.
COVID-19 as an occupational stressor
4.2
Our finding that COVID-19 stressors increased odds of comorbid anxiety and depression by 2.65-fold (95% CI: 1.26–3.26) aligns with international evidence on pandemic mental health impacts among essential workers. De Boni et al. (24) demonstrated that an unhealthy lifestyle during confinement dramatically increased odds of depression (AOR 4.00), anxiety (AOR 2.39), and comorbidity (AOR 8.30), suggesting that pandemic-related behavioral changes mediate mental health outcomes. Similarly, Naghavi-Konjin et al. (53) found complex relationships between COVID-19 risk perception and anxiety among Iranian manufacturing workers, where higher risk awareness paradoxically reduced anxiety, possibly through enhanced control perceptions.
The stronger association with feeling vulnerable (AOR: 3.34, 95% CI: 2.17–4.06) in our study parallels findings across essential worker populations. Amsalem et al. (47) identified vulnerability factors, including younger age, female gender, and transgender identity, as predictors of higher symptom severity among U.S. essential workers. This vulnerability-distress relationship was particularly pronounced among healthcare workers globally, with Mexican healthcare workers showing similar patterns (41), suggesting universal psychological mechanisms operating across essential worker categories.
Our findings must be understood within the broader context of pandemic impacts on developing economies. The ILO (52) documented how workers in developing countries faced pronounced income losses with minimal stimulus support, creating a “vicious circle” affecting well-being and recovery. This is particularly relevant for Mexican automotive workers who, despite maintaining employment, operated within systems characterized by “decent work deficits”: inadequate income or economic insecurity, excessive working hours or unstable schedules, lack of occupational safety and health protections, limited access to social protection or health services, absence of voice, representation, or workplace participation, exposure to discrimination, violence, or harassment, and constraints on personal development or work life balance; and limited social protection factors that likely amplified the psychological burden of pandemic stressors beyond what objective exposure alone would predict.
The psychosocial pathways linking COVID-19 exposure to mental health outcomes involve multiple mechanisms. Building on Oksanen et al.’s (50) identification of psychological distress, work exhaustion, and technostress as predictors, our study demonstrates that perceived vulnerability operates independently from actual exposure, with subjective threat appraisal (AOR: 3.34) showing stronger associations than objective stressor exposure (AOR: 2.65). This suggests interventions targeting threat perception and coping resources may be as important as reducing actual exposure risks.
Limitations
4.3
While this study provides valuable insights, several limitations merit consideration. The cross-sectional design prevents causal inference about COVID-19 stressors and mental health outcomes. Self-report measures in a workplace setting may underestimate true prevalence due to stigma concerns. Our sample from two plants in Guanajuato limits generalizability, and the absence of pre-pandemic baseline data prevents determining whether observed rates reflect COVID-specific increases or ongoing occupational challenges. Additionally, unmeasured factors including work conditions, home stressors, and mental health history may confound observed relationships. Despite these constraints, our findings document substantial mental health burden requiring urgent intervention in Mexican automotive workers. We acknowledge that unmeasured contextual factors such as differences in sociodemographic characteristics between worksites, variability in job demands, pre-existing mental health conditions, and unequal access to support services may act as confounders in the observed associations. Additionally, methodological constraints inherent to the study design, including its cross-sectional nature, reliance on self-reported data, and lack of longitudinal follow-up, limit causal inference.
Conclusion
5
This study documented the prevalence of mental health symptoms among Mexican automotive workers during COVID-19, with approximately one-third experiencing work-related stress and burnout, one-quarter reporting clinically significant anxiety and depression, and 14% engaging in hazardous substance use. The association between COVID-19 stressors and increased mental health symptoms (AOR: 2.65) underscores the pandemic’s amplification of existing occupational vulnerabilities in manufacturing settings. These findings highlight the urgent need for culturally-adapted workplace mental health interventions in Mexico’s automotive sector, including enhanced psychosocial safety protocols, accessible mental health services tailored for shift workers, and organizational strategies to reduce stigma. Specifically, service use includes individual psychotherapy, and mental health counseling or brief psychological support, and, in some cases, employer-provided wellness or stress-management programs. Implementation of evidence-based workplace interventions could substantially reduce psychological morbidity while improving productivity and retention in this essential industrial workforce.
On-site psychological services, available during all shifts (morning, afternoon, and night), with a focus on immediate care, accessibility, and confidentiality. Extended coverage responds to the need to provide support to students, teachers, or workers who, due to their schedules, cannot access traditional services. Peer support programs based on psychosocial intervention models that train students or volunteer collaborators as initial emotional support agents. These programs promote a sense of community, reduce stigma, and facilitate the timely detection of people at risk. Psychoeducation and mental health promotion campaigns aimed at informing people about common symptoms, healthy coping mechanisms, and available care options. These campaigns should be culturally relevant and use digital, print, and in-person media to ensure their reach. Effective integration of mental health services with occupational health units, both in educational institutions and workplaces. This coordination allows for continuous monitoring of emotional well-being, facilitates early interventions, and promotes healthy work and study environments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brown JP Martin D Nagaria Z Verceles AC Jobe SL Wickwire EM. Mental health consequences of shift work: an updated review. Curr Psychiatry Rep. (2020) 22:7. doi: 10.1007/s 11920-020-1131-z, 31955278 · doi ↗ · pubmed ↗
- 2Roche AM Pidd K Fischer JA Lee N Scarfe A Kostadinov V. Men, work, and mental health: a systematic review of depression in male-dominated industries and occupations. Saf Health Work. (2016) 7:268–83. doi: 10.1016/j.shaw.2016.04.005, 27924229 PMC 5127922 · doi ↗ · pubmed ↗
- 3Willums J-O Midttun A Staurem E. The automotive industry: meandering towards green transition in the European Union and the United States In: Midttun A Witoszek N, editors. Energy and transport in green transition. London: Routledge (2015)
- 4Helmold M. New work in the automotive industry In: Helmold M, editor. New work, transformational and virtual leadership. Singapore: Springer International Publishing (2021). 157–69.
- 5Sanginés J. C. Russo M. Simonazzi A. 2021. Mexico’s automotive industry: a success story? (SSRN Scholarly Paper No. 3952148). Social Science Research Network. Available online at: https://papers.ssrn.com/abstract=3952148 (Accessed January 9, 2026).
- 6Eftekhari S Karimi L Sharifian SA Aminian O Rasooli SR Zia G. Association between occupational stress and mental health in an automobile manufacturing factory in Iran. Int J Occup Saf Health. (2025) 15:1–14. doi: 10.3126/ijosh.v 15i 1.61572 · doi ↗
- 7Omair M Ullah M Ganguly B Noor S Maqsood S Sarkar B. The quantitative analysis of workers’ stress due to working environment in the production system of the automobile part manufacturing industry. Mathematics. (2019) 7:627. doi: 10.3390/math 7070627 · doi ↗
- 8Abdul Ghapa NA Hashim H Rasdi I Zainal Abidin E. The relationship between safety culture maturity and mental health among workers in automotive industry. Malays J Med Health Sci. (2023) 19:101–8. doi: 10.47836/mjmhs.19.s 14.11 · doi ↗