Rethinking Neonatal Vaccination Policies: A Neuroimmune Perspective
Zeinab Paymani, Mostafa Nazari, Kayvan Mirnia, Razieh Sangsari, Marzieh Ebrahimi, Fatemeh Haghighi

TL;DR
This paper reviews how early-life vaccinations might affect brain and immune development, suggesting a cautious approach to neonatal vaccine timing.
Contribution
The paper introduces the ALLARA principle for individualized neonatal vaccination strategies based on neuroimmune interactions.
Findings
Vaccine-induced immune activation may influence brain development via epigenetic and cytokine pathways.
Immune overstimulation and microbiome disruption could be linked to autoimmune and neurodevelopmental risks.
Current evidence gaps highlight the need for more research on long-term neurological and immunological outcomes.
Abstract
Neonatal vaccination is a cornerstone of early-life infectious disease prevention. However, the timing and safety of these interventions require careful consideration. This review explored the neuroimmune implications of early immunization, with a specific focus on the interplay between the developing immune and nervous systems. We examined potential mechanisms through which vaccine-induced immune activation might influence brain development, through epigenetic modifications and sustained cytokine responses, particularly involving interleukin-6 (IL-6). The discussion addressed concerns related to immune overstimulation, regulatory T-cell suppression, and microbiome disruption, considering their potential links to autoimmune and neurodevelopmental disorders. In light of the identified evidence gaps, we advocate for a cautious, individualized vaccination approach guided by the “As Low and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
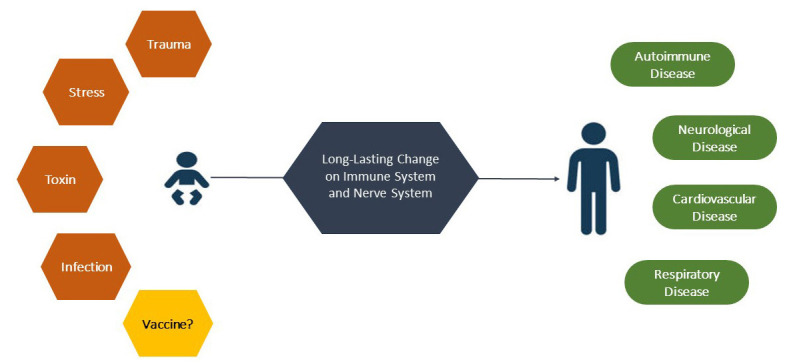 Figure 1
Figure 1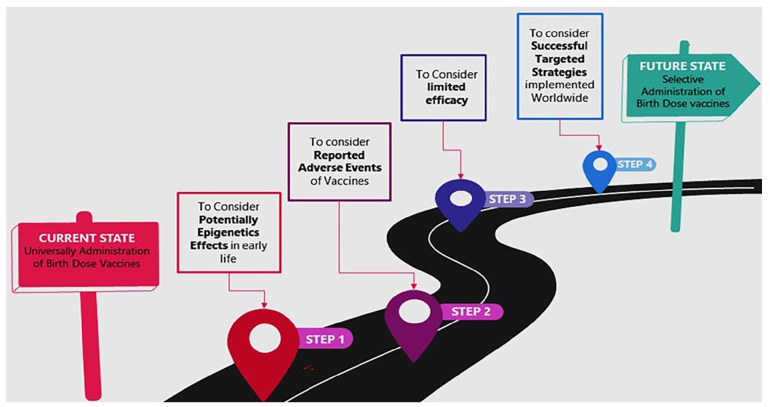 Figure 2
Figure 2| Author, year, reference | Events | Type of study |
|---|---|---|
| Geier et al., 2005
| Multiple sclerosis, optic neuritis, vasculitis, arthritis, alopecia, lupus erythematosus, rheumatoid arthritis | Case control |
| Geier M et al., 2003
| Erythema nodusum, lichen planus, polyarteritis nodosa, Reiter syndrome, thrombocytopenic purpura, Evans syndrome, acute posterior multifocal placoid pigment epitheliopathy, optic neuritis, transverse myelitis, central nervous system demyelination, cerebellar ataxia, multiple sclerosis, chronic fatigue syndrome | Review |
| Maubec et al., 2005
| Cutaneous pseudolymphoma, vitiligo, chronic fatigue syndrome | Case series |
| Júnior et al., 2020
| Graves’ Disease, rheumatoid arthritis (RA), psoriasis, lupus, Hashimoto’s thyroiditis (HT), vitiligo | Case control |
| Oscar-Danilo et al., 2009
| Chronic fatigue syndrome | Review |
| Mikaeloff et al., 2009
| Multiple sclerosis | Case control |
| Herroelen et al., 1991
| Multiple sclerosis | Case reports |
| Tourbah et al., 1999
| Central nervous system demyelination | Case series |
| Agmon-Levin et al., 2014
| Chronic fatigue syndrome, fibromyalgia | Case control |
| Nancy et al., 2008
| Chronic fatigue syndrome | Case reports |
| Richardson et al., 2018
| Alopecia areata | Case reports |
| Choffray et al., 2007
| Lupus panniculitis | Case reports |
| Luhadia et al., 2022
| Multiple sclerosis | Case reports |
| Case Series et al., 2002
| Lichen planus | Case series |
| de la Fuente et al., 2013
| Childhood bullous pemphigoid | Case series |
| Erbagci et al., 2002
| Childhood bullous pemphigoid | Case reports |
| Berkun et al., 2005
| Pemphigus | Case reports |
| Vital et al., 2002
| Inflammatory neuropathy | Case reports |
| De Carvalho et al., 2008
| Systemic polyarteritis nodosa | Review |
| Maillefert et al., 1997
| Polyarthralgia | Case reports |
| Zaas et al, 2001
| Takayasu’s arteritis | Case reports |
| Agmon-Levin et al., 2009
| Systemic lupus erythematosus | Case series |
| Bogdanos et al., 2009
| Multiple sclerosis | Case control |
| Altman et al., 2008
| Dermatomyositis | Case reports |
| Geier et al., 2004
| Arthritis, rheumatoid arthritis, myelitis, optic neuritis, multiple sclerosis, Guillain-Barré syndrome, glomerulonephritis, thrombocytopenia, systemic lupus erythematosus | Case series |
| Geier et al., 2002
| Arthralgia, arthrosis, arthritis, thrombocytopenia, hepatitis, erythema, Guillain-Barré Syndrome, myelitis, vasculitis | VAERS |
| Pennesi et al., 2002
| Glomerulonephritis | Case reports |
| Poierriez J et al., 2004
| Transverse myelitis, neurolupus | Case reports |
| Schattner et al., 2005
| Rheumatoid arthritis, reactive arthritis, vasculitis, encephalitis, neuropathy, thrombocytopenia | Review |
| Cohen et al., 1996
| Erythema nodosum, immune thrombocytopenia, myasthenia gravis, uveitis, Reiter’s syndrome, arthritis, systemic lupus erythematosus, central nervous system demyelination, anti-DNA antibodies emergence, Evans’ syndrome | Review |
| Ramirez Rivera et al., 2003
| Polymyositis | Case report |
| Agmon-Levin, 2009
| Transverse myelitis with a short interval <2 months | Multianalysis |
| Maillefert et al., 1999
| Rheumatoid arthritis, systemic lupus erythematosus, polyarthralgia, myalgia, vasculitis, miscellaneous with mixed presentations | Original article |
| Ronch etal., 1998
| Immune thrombocytopenic in infants within 1 month | Case series |
| Neau et al., 1998
| Immune thrombocytopenic in children | Case series |
| Berkun et al., 2005
| Pemphigus | Case reports |
| Chave et al., 2003
| Henoch shonlein purpura | Case report |
| Khamaisi et al., 2004
| Guillain-Barré syndrome | Case reports |
| Girard et al., 2004
| Multiple sclerosis, chronic fatigue syndrome | Review |
| Wise et al., 1997
| Alopecia | Case Series |
| Avci et al., 2013
| Hemolytic uremic syndrome | Case report |
| Author, year, reference | Events | Type of study |
|---|---|---|
| Shoenfeld et al., 2011
| Macrophagic myofasciitis syndrome (MMF) Gulf War Syndrome | Review |
| Zafrir et al., 2012
| Neuro-psychiatric symptoms, fatigue, mucocutaneous, musculoskeletal, and gastrointestinal complaints. Elevated titers of autoantibodies | Original |
| Boretti et al., 2021
| Autism | Review |
| Shaw, et al., 2013
| Autoimmune/inflammatory syndrome, autism spectrum disorders | Review |
| Graham Ewing, 2009
| Autism | Review |
| Tomljenovic et al., 2011
| Autoimmunity, long-term brain inflammation, and associated neurological complications | Review |
| Borba, 2020
| Sarcoidosis, Sjögren’s syndrome, undifferentiated connective tissue disease | Review |
| Author, year, reference | Events | Type of study |
|---|---|---|
| Jain et al., 2022
| Phlyctenular conjunctivitis, scleritis, sclerokeratitis, retinal periphlebitis, iridocyclitis, choroiditis, uveitis, keratitis | Review |
| Khalili et al., 2021
| Chronic granulomatous disease | Case reports |
| Dahl et al., 2020
| Increased risk of hip fracture | Cohort |
| Tsujioka et al., 2022
| Osteomyelitis | Cohort |
| Wang et al., 2022
| Lymphadenitis | Cohort |
| Sellami et al., 2018
| Disseminated bacillus Calmette-Guérin | Cohort |
| Modrzejewska et al., 2006
| Detachment of retina | Case reports |
| Salmon et al., 2019
| Hodgkin’s lymphoma (HL) | Cohort |
| Shoenfeld et al., 2001
| Reiter’s syndrome | Case reports |
| Schuchmann et al., 2001
| Juvenile chronic arthritis | Case reports |
| Anis et al., 2023
| Reactive arthritis, psoriasis, Myasthenia gravis, ocular manifestations | Review |
| Sharan et al., 2005
| Autoimmune retinopathy | Case reports |
| Nakagawa et al., 2018
| Reiter’s syndrome | Case series |
| Genereau et al,. 1996
| Polymyalgia rheumatica | Case reports |
| Thepot et al., 1995
| Acute polyarthritis | Case reports |
| Granel et al., 2004
| Cryoglobulinemic vasculitis | Case reports |
| Tsuchiya et al., 2021
| Intestinal ulcers | Case reports |
| Parent et al., 2018
| Primary angiitis of the central nervous system (PACNS) | Review |
| Beisland et al., 2004
| Vitiligo | Case reports |
| Shoenfeld, 2001
| Inflammatory arthritis | Case series |
| Bernini, et al., 2015
| Kawasaki, arthritis | Review |
| Vittori, et al., 1996
| Tuberculosis lupus | Case reports |
| Izumi, 1982
| Lupus vulgaris | Case reports |
| Noishiki et al., 2023
| Keloid | Review |
| Abid et al., 2021
| Acute hepatitis with granulomatous steatohepatitis and portal fibrosis | Case reports |
| Yamazaki-Nakashimada et al., 2019
| Endophthalmitis, uycotic aneurysms, Takayasu arteritis, Kawasaki disease, Reiter syndrome, and Guillain-Barré syndrome | Review |
| Sumida, et al., 2003
| Autoimmune pancreatitis | Case report |
| Foucard, et al., 1971
| Osteoarthritis | Case series |
| Author, year, reference | Events | Type of study |
|---|---|---|
| Zawar et al., 2017
| Gianotti-Crosti syndrome | Cohort |
| Gao et al., 2021
| Immune thrombocytopenic purpura (ITP), vaccine-associated paralytic poliomyelitis (VAPP) | Cohort |
| Akbayram et al., 2015
| Immune thrombocytopenic purpura (ITP) | Cohort |
| Elkhayat et al., 2020
| Childhood acute disseminated encephalomyelitis | Case series |
| Kelly et al., 2006
| Transverse myelitis | Review |
| Hughes et al., 2020
| Central nervous system demyelination | Cohort |
| Agmon-Levin et al., 2009
| Transverse myelitis with a short interval <2 months | Multi-analysis |
| Chambrun et al., 2015
| Crohn’s, ulcerative colitis | Review |
| Plat et al., 2014
| Paralytic poliomyelitis (VAPP) | Review |
| Ami Schattner et al., 2005
| Neurologic (encephalitis, Guillain–Barré syndrome) | Review |
| Rheumatic (acute arthritis) | ||
| Hematologic (thrombocytopenia, immune hemolytic anemia) | ||
| Dhiman et al., 2018
| Acute flaccid paralysis | Original |
| Author, year, reference | Vaccinated vs. unvaccinated | Type of study |
|---|---|---|
| Hooker et al., 2020
| Developmental delays (OR = 2.18), asthma (OR = 4.49), and otitis media (OR = 2.13). | Comparative study |
| Hooker et al., 2021
| Severe allergies (OR=4.31), autism (OR=5.03), gastrointestinal disorders (OR=13.8), asthma (OR=17.6), ADHD (OR=20.8), Chronic ear infections (OR=27.8) | Comparative study |
| Mawson et al., 2017
| Neurodevelopmental delay, pneumonia, otitis media, allergies | Comparative study |
| Author, year, reference | Vaccine | Efficacy (%) | Time measurement |
|---|---|---|---|
| Soulié et al.,1991
| HBV | 50 | 4 weeks |
| Strandmark et al., 2022
| HBV | 18 | 4 weeks |
| Martinez et al., 2022
| BCG | 42 | <3 years |
| Roy et al., 2014
| BCG | 32 | <5 years |
| Waggie et al., 2011
| OPV | 41 | 4 weeks |
| Sutter et al., 2010
| OPV | 15 | 4 weeks |
| El-Sayed et al., 2008
| OPV | 37 | 4 weeks |
| Bhaskaram et al.,1997
| OPV | 4 | 6 weeks |
| Jain et al., 1997
| OPV | 13 | 6 weeks |
| Khare et al., 1993
| OPV | 38 | 6 weeks |
| Dong et al., 1986
| OPV | 37 | 4 weeks |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsImmune responses and vaccinations · Bacterial Infections and Vaccines · Vaccine Coverage and Hesitancy
What’s Known
- The World Health Organization (WHO) recommends universal administration of birth dose vaccines, including hepatitis B (HBV), oral polio vaccine (OPV), and bacillus Calmette-Guérin (BCG), to prevent early-life infectious diseases. These vaccines are generally considered safe, with reported side effects being predominantly mild and transient, such as low-grade fever, local swelling, or irritability.
What’s New
- This review critically examined unexplored dimensions of neonatal vaccination, including immune immaturity, the potential epigenetic implications of early immune activation, and possible autoimmune and neurological consequences. It also addressed challenges of limited immunogenicity and the effectiveness of targeted vaccination strategies. The authors proposed an “As Low and Late As Reasonably Achievable” (ALLARA) based strategy to optimize safety, efficacy, and long-term outcomes of early-life immunization.
Introduction
At birth, both the immune system and the brain of a newborn are functionally immature, possessing only basic capabilities that evolve rapidly during the first 2 years of life. ^ 1 ^ This period is characterized by extensive neurodevelopment, including structural growth, myelination, and connectivity, alongside cognitive, motor, and sensory maturation, all of which influence lifelong behavior. ^ 2
- 5 ^ Simultaneously, the neonatal immune system is underdeveloped, with reduced functionality in key components, such as monocytes, neutrophils, dendritic cells, natural killer (NK) cells, and T-cells. ^ 6 ^ Early immunity primarily relies on maternal antibodies transferred via the placenta and breast milk. ^ 7 ^ Accordingly, studies suggested that immune hyperactivity during fetal and early infancy stages could shape lifelong brain and immune function, potentially increasing disease susceptibility. ^ 8
- 12 ^ This concept—that early immune events can have permanent developmental consequences—raises the concern that neonatal exposure to multiple vaccine antigens could alter neuroimmune developmental programs and induce long-term changes in gene expression through epigenetic mechanisms such as DNA methylation or histone modification.
Vaccination represents one of the most effective public health interventions, preventing the spread of infectious diseases and significantly reducing associated morbidity and mortality. Its goal is to elicit a long-lasting, pathogen-specific immune response, while minimizing adverse reactions. It is therefore imperative that vaccine-mediated protection during early life is both safe and efficient. To this end, the World Health Organization (WHO) recommends the administration of specific vaccines, namely the hepatitis B virus (HBV), bacillus Calmette-Guérin (BCG), and oral polio (OPV) vaccine, within the first 24 hours of life. These are referred to as birth-dose vaccines. ^ 13
- 15 ^
In this review, we examined neonatal vaccination from a neuroimmune perspective, focusing on its potential epigenetic impacts, safety challenges, efficacy, and current strategies. Special attention was paid to how early immune activation might influence the developing nervous system and long-term health outcomes. This study aimed to provide healthcare professionals and policymakers with evidence-based insights to help guide neonatal vaccination strategies that carefully balance robust immunological protection with neurodevelopmental safety.
Early Life Experience and Lifelong Health
The immune and nervous systems undergo critical, coordinated development during early life, and their interplay significantly affects lifelong health. A growing body of evidence indicate that early life adversity (ELA) could induce long-lasting changes in the immune function, increasing susceptibility to chronic diseases later in life. ^ 16
- 18 ^ The immune system is integral to normal brain development, behavior, and neural function, ^ 18 ^ and immune dysregulation during sensitive developmental windows may contribute to neurological and psychiatric disorders. ^ 19 ^ Postnatal immune activity has been directly linked to neurological impairments and an increased risk of autoimmune diseases. ^ 19 , 20 ^
ELA refers to a wide range of adverse exposures—including trauma, stress, infections, and environmental toxins—that can shape immune system development through epigenetic reprogramming. ^ 21 ^ Such early-life programming may increase the risk of chronic diseases, including cardiovascular, pulmonary, autoimmune, and neurological disorders. ^ 22
- 27 ^ Given that neonatal vaccines are administered during these sensitive developmental periods, it is crucial to investigate their potential epigenetic impacts on the neuroimmune axis (figure 1).
The figure illustrates how early-life exposures, such as stress, trauma, infection, and toxins, can dysregulate the neonatal immune system, contributing to disease in adulthood. It also raises the question of whether neonatal vaccination, as another form of immune-activating factor, could exert similar long-term neuroimmune effects.
Studies suggested that ELA could lead to heightened innate immune responsiveness and chronic low-grade inflammation, characterized by elevated pro-inflammatory cytokines, such as interleukin-6 (IL-6) and C-reactive protein (CRP). ^ 28
- 30 ^ A prominent example is fetal inflammatory response syndrome (FIRS), marked by elevated fetal plasma IL-6 levels in utero, which is associated with an increased risk of neurodevelopmental, psychiatric, autoimmune, cardiovascular, and pulmonary diseases. ^ 31
- 33 ^ Similarly, the BCG vaccine—administered at birth in many countries—induces the production of IL-6, interferon gamma (IFN-γ), and tumor necrosis factor alpha (TNF-α), a process known as trained immunity that involves epigenetic reprogramming of innate immunity and monocytes’ function. ^ 34
- 37 ^ IL-6 levels have been reported to remain elevated for up to a year following BCG vaccination, ^ 37 ^ raising concerns about whether this sustained immune activation could represent a form of maladaptive epigenetic reprogramming.
IL-6 is a key cytokine that regulates immune activation, acute phase responses, and tissue repair. However, its chronic elevation is implicated in the pathogenesis of autoimmune disorders, chronic inflammatory diseases, and certain cancers. Consequently, IL-6 blockade has shown therapeutic benefits in experimental models of inflammatory bowel disease, diabetes, multiple sclerosis, asthma, rheumatoid arthritis, and inflammation-related cancers. ^ 38 ^ Elevated IL-6 also facilitates infiltration of dendritic cells and macrophages into the brain, disrupting neuronal excitability and neurotransmission, which can result in long-term impairments in synaptogenesis and neurogenesis. ^ 39 , 40 ^
In parallel, the colonization of infant gut microbiota has been widely recognized for its role in brain development and establishing an early life imprint on the immune system. ^ 41 ^ However, alterations to the commensal gut microbiota during this period might increase the risk of inflammatory or allergic diseases later in life. Enterovirus colonization in early infancy, for instance, could restructure the gut microbiome and potentially trigger autoimmunity. ^ 42 ^ Given this established pathway of virus-induced dysbiosis, an important question arises: could the administration of live attenuated poliovirus via neonatal vaccination contribute to microbiome dysbiosis and an increased risk of autoimmunity?
Newborns possess a uniquely tolerant immunological state, characterized by abundant T regulatory (Treg) cells. These cells are essential for maintaining a balanced and controlled immune system and for preventing inappropriate immune activation. Tregs are key players in controlling inflammation, preventing autoimmunity, and ensuring immune responses are appropriately scaled. ^ 43 ^ However, because Tregs can dampen vaccine-induced immunity, adjuvants are often used to suppress Treg activity and enhance immunogenicity. ^ 44 , 45 ^ While this approach supports vaccine efficacy, it may also transiently reduce Treg function in infants. This raises a challenging question: could this early-life reduction in Treg-mediated suppression impact the establishment of lifelong self-tolerance, thereby increasing susceptibility to autoimmunity and future dysregulated immune responses?
Autoimmune and Neurological Adverse Events Following Immunization
A significant body of evidence, including case reports, original articles, reviews, and comparative studies, documented the association between HBV, BCG, and polio vaccines—as well as HBV vaccine adjuvants—and the subsequent development of autoimmune and neurological disorders. However, establishing a causal relationship is challenging. Some of these challenges are discussed in this section.
Vaccine safety surveillance data suggested that most vaccine side effects are usually mild and transient, lasting 1-2 days. However, concerns have been raised regarding the potential for later adverse events. ^ 46 , 47 ^ Furthermore, the durations of pre- and post-license clinical trials are often insufficient for evaluation of long-term side effects. While many studies indicated that harmful exposures during early life could heighten vulnerability to chronic diseases later in life, ^ 16
- 18 , 48 , 49 ^ scientific literature described several pathways by which vaccines, similar to viruses and other microorganisms, could trigger autoimmune reactions. These include molecular mimicry, cross-reactivity, bystander activation, epitope spreading, and antigen persistence. ^ 50
- 56 ^ For instance, HBV vaccine epitopes were reported in the context of synergistic autoimmune competence. ^ 57 ^ Additionally, components of the HBV vaccine demonstrated sequence homology and molecular mimicry with human proteins: with the hair follicle protein solute carrier family 45 member 2 (SLC45A2), and with myelin basic protein and myelin oligodendrocyte glycoprotein. These are proposed as plausible biological mechanisms for alopecia areata and multiple sclerosis, respectively. ^ 58 , 59 ^
We have reviewed studies reporting adverse effects to highlight the potential of these vaccines to contribute to autoimmune and neurological diseases. The cited studies often support a causal link based on a short temporal relationship—typically less than 2 months—between vaccine administration and the appearance of autoimmunity. These adverse effects are not confined to childhood, underscoring the potential for these vaccines to contribute to such conditions across different age groups.
HBV Vaccine Adverse Events
Multiple case reports and case series highlighted a connection between the HBV vaccine and various autoimmune and neurological diseases, including arthritis/polyarthralgia, lupus erythematosus, multiple sclerosis, optic neuritis, vasculitis, alopecia areata, erythema nodosum, polyarteritis nodosa (PAN), thrombocytopenic purpura, evans syndrome, Guillain-Barré Syndrome (GBS), glomerulonephritis, uveitis, polymyositis, dermatomyositis, Takayasu’s arteritis, Hashimoto’s thyroiditis, Graves’ disease, childhood bullous pemphigoid, chronic fatigue syndrome, cutaneous pseudo lymphoma, vitiligo, lichen planus. A comprehensive list is presented in table 1.
In addition to the side effects associated with HBV vaccine epitopes, HBV vaccines contain aluminum adjuvants as boosters of immune response. The adjuvants are substances added to vaccines to enhance the immunogenicity of the vaccine antigens. ^ 97
- 99 ^ Studies indicated that aluminum-based adjuvants in the HBV vaccine are associated with neuro-psychiatric symptoms, fatigue, mucocutaneous, musculoskeletal, and gastrointestinal complaints. They have also been linked to autoimmune/inflammatory syndrome induced by adjuvants (ASIA) syndrome, autism spectrum disorder, sarcoidosis, Sjogren’s syndrome, elevated titers of autoantibodies, and undifferentiated connective tissue diseases, as summarized in table 2. Aluminum compounds can persist in the human body for many years post-vaccination. ^ 100 ^
Moreover, aluminum has demonstrated a detrimental impact on the blood-brain barrier (BBB) and is connected to microglia-triggered pro-inflammatory cytokine release. Due to its high reactivity, the aluminum ion (Al^3+^) can interfere with several biological functions in the developing brain, including enzymatic activities of key metabolic pathways. In the context of infancy, a significant correlation has been reported between pediatric vaccines containing aluminum adjuvants and the incidence of autism spectrum disorders. Infants receiving these vaccines have a notably higher incidence of autism spectrum disorder (ASD), suggesting a potential association between these vaccine components and developmental sequelae. ^ 101 ^
BCG Vaccine Adverse Events
Previous studies reported autoimmune and neurological disorders following BCG vaccination. A portion of the evidence regarding BCG adverse events is derived from studies utilizing intravesical BCG (iBCG) for cancer immunotherapy. Reported side effects include juvenile idiopathic arthritis (JIA), juvenile dermatomyositis, Takayasu arteritis, autoimmune pancreatitis, GBS, optic neuritis, meningitis, vasculitis, psoriasis, endophthalmitis, uveitis, autoimmune retinopathies, Hodgkin’s lymphoma, lymphadenitis, osteomyelitis, osteitis, and disseminated disease (BCGosis), as illustrated in table 3.
Besides, BCG vaccination has presented a significantly high rate of complications in patients with severe combined immunodeficiency (SCID), leading to substantial morbidity and mortality. An analysis of BCG-vaccinated patients with SCID from 28 centers across 17 countries revealed that early vaccination (≤1 month) was associated with a higher prevalence of BCG-related complications and death. ^ 108 ^
OPV Vaccine Adverse Events
Although adverse events related to the oral polio vaccine (OPV) are generally considered rare, cases of autoimmune effects following colonization of the gut by the attenuated polioviruses, a serotype of enterovirus C within the picornaviridae family, have been reported. Autoimmune events associated with OPV include multiple sclerosis, childhood acute disseminated encephalomyelitis, vaccine-associated paralytic poliomyelitis (VAPP), acute flaccid paralysis, immune thrombocytopenia (ITP), Gianotti-Crosti syndrome (GCS), transverse myelitis, ulcerative colitis (UC), and Crohn’s disease (CD), as detailed in table 4.
Challenges of Discovering Adverse Events Post-Vaccination
The WHO provides a comprehensive guideline for assessing causality in adverse events following immunization (AEFI), emphasizing well-defined clinical documentation, a temporal association with vaccination, biological plausibility, and the exclusion of alternative causes. ^ 144 ^ This framework prioritizes identifying strong alternative explanations—such as genetic or pre-existing conditions—before attributing events to vaccines. While this method ensures scientific rigor, it may overlook the complex, multifactorial nature of autoimmune and neurologic diseases, particularly when vaccines act as contributing factors rather than single causes. Moreover, although biological plausibility and timing are central to the WHO’s approach, vaccines can affect the developing immune and nervous systems—especially in early life—with clinical manifestations potentially appearing years later. This underscores the critical need for long-term monitoring. Finally, emerging research is essential to reveal pathophysiological mechanisms that are not yet fully understood.
The WHO guideline also depends heavily on existing literature to assess and often exclude causal links. However, the current literature is often derived from passively gathered data, such as that in the vaccine adverse event reporting system (VAERS), which has inherent methodological limitations. These include a lack of systematic follow-up, significant underreporting, and a failure to capture delayed onset conditions, particularly autoimmune or chronic diseases that manifest long after vaccination. Furthermore, there is no clear guidance on appropriate time windows for monitoring such delayed-onset diseases. It is therefore inappropriate to assume that autoimmune side effects are rare in the absence of robust and comprehensive documentation. Overlapping symptoms and intensive infant vaccination schedules further complicate the identification of specific causal relationships.
To enhance causality assessment, a robust, multidisciplinary approach involving epidemiologists, clinicians, immunologists, and basic scientists is essential. Such collaboration can help elucidate the nuanced relationships between vaccination and long-term immunological or neurological outcomes, thereby informing evidence-based public health strategies.
Another avenue for exploring causal relationships and potential side effects is to compare health outcomes between vaccinated versus unvaccinated populations. Although such studies are often not feasible due to high vaccination coverage in many countries, a limited number of observational surveys exist (table 5). These studies reported higher prevalence of developmental delays, severe allergies, attention-deficit hyperactivity disorder (ADHD), autism spectrum disorders, and even infections (e.g., pneumonia and otitis media) in vaccinated cohorts. Future studies with a two-group design are required to provide further insights.
Efficacy of Neonatal Vaccines
The neonatal immune system is characterized by a state of immune tolerance. At this stage of life, all circulating antibodies are of maternal origin, providing passive immunity until the newborn’s own antibody production becomes robust around 3 months after birth. ^ 7 , 148
- 150 ^ These maternal antibodies are highly effective against most infections. ^ 7 ^ Due to the inherent immaturity of the immune system, neonatal innate immunity relies on distinctive mechanisms. In response to pathogens, the innate immune system serves as the first line of defense. However, neonatal monocytes and dendritic cells (DCs) produce less TNF, IL-12, and IFN-γ, while increasing the production of IL-6, IL-10, and IL-23. ^ 151 , 152 ^ Neutrophils exhibit quantitative and qualitative differences compared to those in older children. ^ 153 ^ NK cells display diminished cytotoxic capability and impaired release of destructive substances against infected cells. ^ 154 ^ Furthermore, neonatal NK cells release less IFN-γ, and their adhesion is compromised due to decreased expression of specific adhesion molecules. ^ 155 ^ This immunological bias renders newborns prone to low inflammatory responses and impairs their responses to many vaccines. ^ 156 ^ In this section, we examine the efficacy of BCG, HBV, and OPV vaccines during the neonatal period. The results are summarized in table 6.
HBV Vaccine Efficacy
Hepatitis B surface antibodies (anti-HBs) are produced by the immune system in response to the hepatitis B surface antigen and serve as a marker for immunity. ^ 168
- 170 ^ Vaccine efficacy, an anti-HBs level >10 IU/L after vaccination, provides complete protection against acute and chronic hepatitis B. ^ 15 , 171 ^ The HBV vaccine is highly effective in infants, with over 95% of healthy recipients developing seroprotective anti-HBs levels within 1 month after the final dose. ^ 172 , 173 ^ However, few studies have evaluated the seroprotective rate of the HBV vaccine specifically in the neonatal period. These studies reported seroconversion rates of only 18% to 50%, 1 month after receiving the birth dose, without accounting for the potential interference of maternal antibodies (table 6). ^ 157 , 174 ^ Moreover, several studies indicated that individuals with a low antibody response exhibited reduced T-cell proliferation and cytokine production. ^ 158 , 175
- 177 ^ Research also showed that the immune response was enhanced when the first vaccination dose was administered at 2 months of age. ^ 174 , 178
- 180 ^ This improvement could be attributed to the maturation of the infant’s immune system. ^ 181
- 183 ^ A large review in Africa demonstrated that children born to HBsAg-negative mothers, the risk of infection remained minimal even when vaccination began at 2 months, suggesting no clear additional benefits from the HBV birth dose. ^ 184 ^
BCG Vaccine Efficacy
The BCG vaccine has stood as the exclusive vaccine against tuberculosis (TB) for decades. ^ 146 ^ We did not identify any studies specifically reporting the efficacy of BCG vaccination in the early neonatal period. However, a study reported 42% efficacy in children under 5 years of age, ^ 160 ^ while another showed 32% efficacy in children under 3 against all forms of tuberculosis. ^ 159 ^
A limited number of studies explored the immune responses following neonatal BCG vaccination. These investigations have identified CD4-positive (CD4+) and CD8-positive (CD8+)T lymphocytes as the predominant responding cell populations. ^ 36 , 185 ^ The CD4+ T-cells notably upregulate IFN-γ, TNF-α, IL-2, and IL-6, whereas CD8+ T-cells demonstrate minimal to undetectable production of IFN-γ, TNF-α, and IL-2. ^ 35 , 36 , 186 ^ However, the reliability of BCG-specific CD4+ and CD8+ T-cell cytokine expression as a correlate of protection against childhood TB has been questioned. ^ 35 , 187 ^ The limited efficacy of vaccination confirms this theory. ^ 188 ^
Furthermore, investigations revealed that Th1 immune responses become detectable approximately 2-3 months post-vaccination. ^ 187 , 189 ^ Studies have also indicated that immunogenicity is enhanced when BCG administration is postponed until 10 weeks of age. ^ 186 ^
OPV Vaccine Efficacy
Multiple studies have evaluated the effectiveness of the birth dose of the live attenuated oral poliovirus vaccine (OPV). The observed seroconversion rates revealed a range of responses across the different poliovirus serotypes. For type 1, seroconversion rates spanned from 6% to 42% (mean=28%), for type 2, the rates ranged from 2% to 63% (mean=36%), and for type 3, the seroconversion rates varied between 2% and 35% (mean=16%). ^ 161
- 167 ^ This considerable variability underscored the limited and unpredictable immune response triggered by the OPV birth dose in the neonatal period. A more robust immune response is observed with increasing age, highlighting the critical importance of timing and subsequent booster doses for achieving reliable protection against poliovirus infection.
Current Neonatal Vaccination Strategies
The Expanded Program on Immunization (EPI) was established by the WHO in 1974 with the initial goal of protecting children against six major diseases: tuberculosis, polio, diphtheria, tetanus, pertussis, and measles. The program has since expanded its scope to include additional vaccines and immunization coverage goals. A key component of the EPI is the “birth dose”— the administration of a vaccine shortly after birth to provide early protection against diseases that pose an immediate risk to newborns. This strategy is critical for preventing mother-to-child or early environmental transmission of specific infections.
According to WHO guidelines, the birth dose includes specific vaccines to be given within the first 24 hours of life: the BCG vaccine, the zero dose of OPV, and the HBV vaccine. ^ 13
- 15 ^ However, the specific vaccines included and their exact timing can vary based on national health policies and local disease prevalence.
Globally, two primary vaccination strategies are typically implemented for newborns: the ‘general recommendation’ strategy and the ‘recommendation to at-risk groups’ strategy. A general recommendation strategy for neonates involves compulsory administration of essential vaccines to all newborns to establish early protection against preventable diseases. In contrast, the ‘recommendation for at-risk groups’, also known as the selective or targeted strategy, focuses on identifying and prioritizing neonates who face a higher likelihood of exposure to specific infectious diseases or an increased risk of complications due to underlying health conditions or environmental factors.
Nations worldwide implement distinct childhood immunization strategies to protect infants from infectious diseases. While some countries adopt a universal approach, vaccinating all newborns irrespective of their risk factors, others employ a targeted strategy, focusing on specific at-risk groups. Several countries, including Austria, Belgium, the Czech Republic, Denmark, Germany, Iceland, Italy, the Netherlands, Slovakia, and Spain, have discontinued universal BCG vaccination, removing it from their routine schedules. Others, such as Cyprus, Finland, France, Norway, Slovenia, Sweden, and the United Kingdom, currently recommend it exclusively for specific at-risk categories of children. This approach notably includes those with parents from high-TB-prevalence countries or with a family history of TB. The rationale for this targeted approach in low-endemic countries is based on the low infection risk, a high number needed to vaccinate (NNV), i.e., the number of healthy individuals who must be vaccinated to prevent one case of TB, and a high rate of adverse events per prevented TB case.
A similar pattern is seen with the HBV birth dose. Some countries, including Austria, Cameroon, Finland, Germany, Greece, Hungary, Iceland, and Ireland, have not included it in their routine immunization schedules. In contrast, several countries, such as Canada, Belgium, Czechia, Denmark, Estonia, France, Italy, Japan, Latvia, Luxembourg, the Netherlands, New Zealand, Norway, San Marino, Slovakia, Spain, Sweden, Switzerland, and the United Kingdom, recommend HBV birth dose for at-risk groups. This selective recommendation reflects a targeted public health approach, likely considering factors, such as regional prevalence, disease severity, and available resources. Furthermore, OPV is administered in many countries from 2 months of age. Such diverse approaches highlight the adaptability of immunization strategies to individual country requirements and health priorities.
Neonate Vaccination: Future Directions
Neonatal vaccination plays a critical role in preventing early-life infectious diseases, yet it presents unique challenges due to the immaturity of the infant’s immune system. The limited immunogenic responses in neonates can reduce vaccine efficacy and raise concerns regarding the long-term impact of early immune activation. As the immune system matures with age, a more robust and balanced response can be achieved, supporting the consideration of delayed or staged immunization schedules.
Recent concerns have focused on the potential neuroimmune effects of immune stimulation during sensitive developmental windows. Emerging evidence suggested that early-life immune activation might influence epigenetic programming and increase the risk of autoimmune and neurodevelopmental disorders later in life. In response, several countries have begun adopting selective neonatal vaccination strategies, prioritizing high-risk infants and integrating early screening programs. This shift offers valuable opportunities to evaluate long-term outcomes between vaccinated and unvaccinated populations and to tailor immunization strategies more precisely. Figure 2 conceptually outlines these four key considerations—epigenetic impacts, safety challenges, efficacy, and current strategies—guiding a more cautious and evidence-based reevaluation of neonatal vaccination policy.
This roadmap illustrates how critical assessment of four key factors—epigenetic impacts, safety challenges, efficacy, and current strategies—highlights the potential influence of early-life immune activation on long-term health. This integrated analysis supports a shift toward more cautious and evidence-based vaccination approaches.
Conclusion
Vaccination remains a cornerstone of pediatric health. However, its application in the neonatal period requires careful consideration. The balance between providing early protection against infectious diseases and the potential risks of overstimulating the developing immune system must be guided by rigorous scientific evidence. A growing body of research highlight that neonatal immune responses differ significantly from those in older children, necessitating an individualized, developmentally informed approach to vaccine scheduling and administration.
As technologies such as artificial intelligence and precision medicine advance, they offer unprecedented opportunities to design personalized vaccine schedules based on an infant’s genetic predispositions and environmental risk factors. Adopting a flexible, risk-based framework—aligned with the ALLARA principle—can help optimize both safety and efficacy of early-life immunization. Ultimately, neonatal vaccination policies must prioritize long-term neurological and immunological well-being, ensuring that each administered vaccine is both necessary and appropriate for the individual infant.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bateson P Barker D Clutton-Brock T Deb DD’Udine B Foley R Aetal Developmental plasticity and human health Nature 20044304192110.1038/nature 0272515269759 · doi ↗ · pubmed ↗
- 2Dekaban AS Changes in brain weights during the span of human life: relation of brain weights to body heights and body weights Ann Neurol 197843455610.1002/ana.410040410727739 · doi ↗ · pubmed ↗
- 3Richards JE Conte S Brain Development in Infants: Structure and Experience The Cambridge Handbook of Infant Development: Brain, Behavior, and Cultural Context. Cambridge Handbooks in Psychology 2020 Cambridge Cambridge University Press 94127
- 4Gilmore JH Knickmeyer RC Gao W Imaging structural and functional brain development in early childhood Nat Rev Neurosci 20181912337[ PMC Free Article ]10.1038/nrn.2018.129449712 PMC 5987539 · doi ↗ · pubmed ↗
- 5Tierney AL Nelson CA 3rd Brain Development and the Role of Experience in the Early Years Zero Three 200930913[ PMC Free Article ]23894221 PMC 3722610 · pubmed ↗
- 6Georgountzou A Papadopoulos NG Postnatal Innate Immune Development: From Birth to Adulthood Front Immunol 20178957[ PMC Free Article ]10.3389/fimmu.2017.0095728848557 PMC 5554489 · doi ↗ · pubmed ↗
- 7Cinicola B Conti MG Terrin G Sgrulletti M Elfeky R Carsetti Retal The Protective Role of Maternal Immunization in Early Life Front Pediatr 20219638871[ PMC Free Article ]10.3389/fped.2021.63887133996688 PMC 8113393 · doi ↗ · pubmed ↗
- 8Danese ASJL Psychoneuroimmunology of Early-Life Stress: The Hidden Wounds of Childhood Trauma? Neuropsychopharmacology 20174299114[ PMC Free Article ]10.1038/npp.2016.19827629365 PMC 5143500 · doi ↗ · pubmed ↗