Communicative Adaptations After Laryngectomy: Syntactic Complexity and Gesture Use
Marise Neijman, Bertus van Rooy, Roland Pfau, Rob J. J. H. van Son, Michiel W. M. van den Brekel

TL;DR
After losing their natural voice due to laryngectomy, patients use fewer speech fillers and more pauses, but their gestures remain as effective as those of healthy people.
Contribution
This study reveals that laryngectomy patients use fewer disfluencies and similar gestures compared to healthy controls during communication tasks.
Findings
TL patients used significantly fewer fillers and mazes but more short pauses than controls.
Syntactic complexity was largely similar between groups, except for words per C-unit.
Gesture use in TL patients was comparable to controls in frequency, type, and function.
Abstract
Total laryngectomy (TL) results in the loss of natural voice, requiring alternative speech rehabilitation strategies such as tracheoesophageal speech. While voice and intelligibility outcomes after TL are well studied, less is known about the complexity of spoken language production and the role of co‐speech gestures in this group. This study aimed to systematically investigate the complexity and function of spoken language, as well as the use of co‐speech gestures, in TL patients compared with matched controls. The key research question was whether TL patients differ from healthy controls in their syntactic structures and gesture use during structured communicative tasks. Forty‐two participants took part: 21 TL patients using tracheoesophageal speech and 21 gender‐, age‐, and education‐matched controls. Participants watched and retold two animated videos and described the “cookie…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
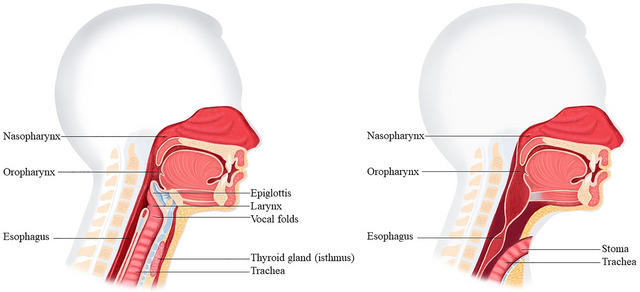 FIGURE 1
FIGURE 1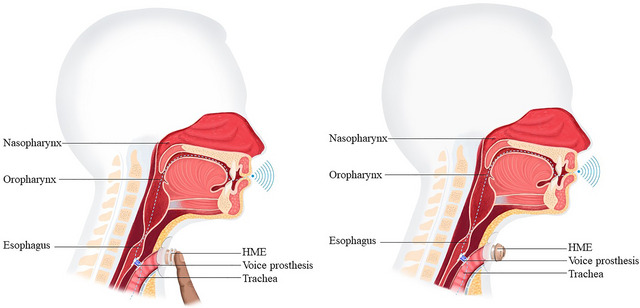 FIGURE 2
FIGURE 2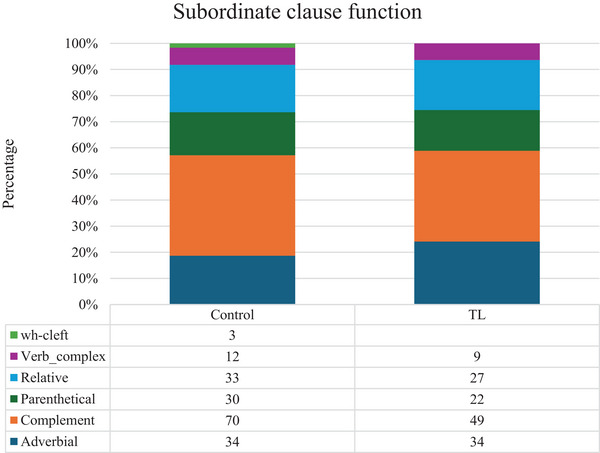 FIGURE 3
FIGURE 3| Category | Definition | Example |
|---|---|---|
|
|
|
(a) and I see further not [what there happened] “ |
|
|
(b) Weer de poes. again the cat “The cat again” | |
|
|
(c) Interviewer: Kunt u het scherm goed zien?
Participant:
| |
|
|
|
(a) En voor de rest <fill> eh </fill> <MAZE> de </MAZE> het ziet er leuk uit buiten, and for the rest <fill> eh </fill> <MAZE> the </MAZE> it looks there fine out outside if you look outside from the kitchen‐window ʻʻAnd the the rest, it looks fine outside, |
|
|
(b) Nou ik heb gezien now I have seen that a pussycat on the calculate was on a board ʻʻNow I have seen | |
|
|
(c) En Tweety pakt een bowlingbal <,> and Tweety takes a bowling‐ball that he through the gutter to below throws “And Tweety takes a bowling ball | |
|
|
(d) what I myself then further reminded is that he thus <fill> eh </fill> the street up went “ | |
|
|
(e) Die heeft he has think I the tap forgotten out to put “He has, | |
|
|
(f) en de kinderen zitten and the children sit slowly but surely the sweety‐jar empty to eat “And the children are busy | |
|
|
|
(a) Het kuikentje zit wel in een hokje the chicklet sits indeed in a cage “The little chicklet sits in a cate after all.” |
|
|
(b) Gebeurt er buiten nog iets? happens there outside still something “Is something still happening outside?” | |
|
|
(c) Hoe heet dat spel ook alweer? how is called that game also again “What is that game called again?” | |
|
|
(d) Oh kijk eens aan oh look even at “Oh, look at that.” | |
|
|
|
(a) en and with one bang hits he against the façade “And |
|
|
(b) alas it was incorrectly calculated “Alas, it was calculated incorrectly.” | |
|
|
(c) maar dat krukje dat heeft drie poten but that crutch. that has three legs “But that little crutch, it has three legs.” | |
|
|
|
(a) Zoonlief zit in keukenkast cookie pakken son‐love sits in kitchen‐cupboard cookie take “Sonny boy sits in cupboard taking cookie.” |
|
|
(b) Verkeerde liniaal gebruikt wrong ruler used “Used wrong ruler.” | |
|
|
|
maar <fill> eh </fill> Tweety die heeft daar een grote bowlingbal but <fill> eh </fill> Tweety he has there a large bowling‐ball “But, uh, Tweety, he has a large bowling ball there.” |
|
|
|
(a) en dat lukt hem maar niet <,> Want hij is aan het tekenen… and that succeeds him just not <,> because he is on the draw ʻʻAnd he just doesn't succeed <,> because he is still drawing. |
|
|
(b) die kukelt straks ook achterom <,,> Dat was mijn verhaal he tumbles soon also upside‐down <,,> that was my story ʻʻHe will soon tumble down. <,,> That was my story. |
| Gestures that … | ||
|---|---|---|
|
|
| model the shape of an object or motion characteristics of an action. |
|
| represent an abstract idea by means of a concrete shape or motion. | |
|
| point towards an object/person or a location in space. | |
|
| follow and accentuate the rhythm of speech. | |
| Emblems | are conventionalized and have (culture‐specific) standardized meanings. | |
|
| have either an ambiguous connection or lack a direct meaning in relation to the speech content. | |
|
|
| provide semantic information that adds to the speech content. |
|
| give same semantic content but might help listeners understand the message better, therefore enhancing the communicative intend of the speech. | |
|
| carry meaning that is not included in the speech content to the point where gesture might even take over speech. | |
|
| are synchronized with the pace of speech and reinforce the rhythm of speech. | |
|
| emphasize meaning | |
|
| are intended to aid lexical access. | |
|
| show a modification in sentence structure. | |
|
| do not conform to any of the above or do not seem to have a specific function that relates to surrounding speech. |
|
|
| ||||||||
|---|---|---|---|---|---|---|---|---|---|
| # | Gender | Age | Education | Months post‐TL | Speech rehab | # | Gender | Age | Education |
| 1 | Male | 61 | Higher | 72 | FreeHands | 22 | Male | 63 | Higher |
| 2 | Male | 57 | Lower | 10 | HME | 23 | Male | 64 | Secondary |
| 3 | Male | 88 | Higher | 41 | HME | 24 | Male | 90 | Vocational |
| 4 | Female | 72 | Secondary | 76 | HME | 25 | Female | 74 | Secondary |
| 5 | Male | 70 | Higher | 15 | HME | 26 | Male | 69 | Higher |
| 6 | Male | 65 | Vocational | 73 | HME | 27 | Male | 60 | Vocational |
| 7 | Male | 74 | Secondary | 67 | HME | 28 | Male | 82 | Secondary |
| 8 | Female | 79 | Secondary | 15 | HME | 29 | Female | 73 | Secondary |
| 9 | Male | 73 | Higher | 39 | HME | 30 | Male | 79 | Higher |
| 10 | Male | 53 | Vocational | 13 | HME | 31 | Male | 58 | Vocational |
| 11 | Male | 72 | Vocational | 94 | HME | 32 | Male | 75 | Vocational |
| 12 | Male | 71 | Vocational | 43 | HME | 33 | Male | 77 | Vocational |
| 13 | Male | 61 | Higher | 52 | HME | 34 | Female | 76 | Higher |
| 14 | Male | 78 | Vocational | 39 | HME | 35 | Male | 79 | Secondary |
| 15 | Male | 76 | Higher | 23 | HME | 36 | Male | 76 | Secondary |
| 16 | Female | 68 | Vocational | 29 | FreeHands | 37 | Female | 59 | Vocational |
| 17 | Male | 56 | Vocational | 23 | HME | 38 | Male | 55 | Vocational |
| 18 | Male | 66 | Vocational | 8 | HME | 39 | Female | 61 | Vocational |
| 19 | Male | 67 | Higher | 65 | FreeHands | 40 | Male | 66 | Higher |
| 20 | Female | 72 | Higher | 213 | HME | 41 | Female | 73 | Higher |
| 21 | Female | 73 | Higher | 12 | HME | 42 | Female | 63 | Vocational |
|
| Males: 16 | Mean 69.1 years | Lower: 1 | Mean 49 months | FreeHands: 3 | Males: 14 | Mean 69.2 years | Lower: 0 | |
| Females: 5 | (range 53–88) | Secondary: 3 | (range 8–213) | HME: 18 | Females: 7 | (range 55–90) | Secondary: 6 | ||
| Vocational: 8 | Vocational: 9 | ||||||||
| Higher: 9 | Higher: 6 | ||||||||
| Syntactic complexity | TL | Controls | Wilcoxon rank‐sum test | |||
|---|---|---|---|---|---|---|
| Median | Median |
|
| p.FDR | ||
|
|
| 187 | 255 | 135 |
| 0.154 |
|
| 156.5 | 168.7 | 161 | 0.134 | 0.319 | |
|
|
| 7.754 | 8.848 | 110 |
|
|
|
| 0.229 | 0.312 | 168 | 0.279 | 0.359 | |
|
|
| 0.248 | 0.245 | 215 | 0.906 | 0.906 |
|
| 0.236 | 0.250 | 197 | 0.741 | 0.834 | |
|
|
| 0.183 | 0.121 | 258 | 0.215 | 0.322 |
|
| 2.559 | 5.944 | 108 |
|
| |
|
| 0.523 | 1.250 | 109 |
|
| |
|
| 9.942 | 5.417 | 356 |
|
| |
|
| 1.011 | 0.500 | 260 | 0.200 | 0.322 | |
| Number of gestures produced | 0 | 1 | 2 | 3 | 4 | 5‐9 | 10‐14 | 15‐20 | 21+ | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Number of TL patients | 3 (14%) | 1 (5%) | 2 (10%) | 2 (10%) | 3 (14%) | 3 (14%) | 2 (10%) | 2 (10%) | 3 (14%) | 21 (100%) |
| Number of controls | 5 (24%) | 3 (14%) | 3 (14%) | 1 (5%) | 0 (0%) | 3 (14%) | 3 (14%) | 3 (14%) | 0 (0%) | 21 (100%) |
| Type of gesture | Iconic | Beat | Deictic | Metaphoric | Emblem | Total (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | TL | C | TL | C | TL | C | TL | C | TL | C | TL | C | |
|
|
| 46 | 29 | 1 | 0 | 22 | 6 | 3 | 0 | 0 | 0 |
|
|
|
| 25 | 23 | 0 | 0 | 7 | 2 | 0 | 0 | 0 | 0 |
|
| |
|
| 0 | 0 | 55 | 33 | 0 | 0 | 0 | 0 | 0 | 0 |
|
| |
|
| 2 | 3 | 1 | 6 | 3 | 2 | 0 | 1 | 0 | 0 |
|
| |
|
| 0 | 0 | 20 | 5 | 0 | 0 | 0 | 0 | 0 | 0 |
|
| |
|
| 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
|
| |
|
| 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
| Gestures | TL | Controls | Wilcoxon rank‐sum test | |||
|---|---|---|---|---|---|---|
| Median | Median |
|
| p.FDR | ||
|
|
| 4 | 2 | 309 |
| 0.116 |
|
|
| 2 | 2 | 256 | 0.372 | 0.527 |
|
| 2 | 1 | 277 | 0.147 | 0.278 | |
|
| 1 | 0 | 284 | 0.085 | 0.208 | |
|
| 0 | 0 | 232 | 0.535 | 0.596 | |
|
| 0 | 0 | 210 | 0.341 | 0.527 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVoice and Speech Disorders · Hearing Impairment and Communication · Temporomandibular Joint Disorders
Introduction
1
Effective communication often depends more on conveying the intended message than on grammatical complexity. Nevertheless, speakers frequently adapt their language and nonverbal behavior to facilitate interaction, especially when facing communicative challenges such as language barriers or speech impairments (Altmann and Troche 2011; Plexico et al. 2009). Communication is inherently multimodal, involving both verbal and nonverbal elements, with co‐speech gestures playing an important role in supporting speech, particularly when verbal abilities are compromised (Kendon 1997; Preisig et al. 2018; Sekine et al. 2013; Tetnowski et al. 2023).
Total Laryngectomy
1.1
A group experiencing primarily physical challenges in speech production are patients who have undergone TL, a surgical procedure removing the larynx, commonly performed to treat advanced laryngeal or hypopharyngeal cancer (Ward and van As‐Brooks 2014). The procedure involves removing the larynx including the vocal folds, permanently separating the upper and lower airways, and creating a tracheostoma at the front of the neck for breathing (see Figure 1). Post‐laryngectomy, patients must adapt to altered speech and breathing, and swallowing in order to communicate effectively (van Sluis et al. 2021).
Anatomy pre‐ and post‐laryngectomy. Left: healthy anatomy; Right: anatomy after total laryngectomy. These images are used with permission from ATOS Medical, Hörby, Sweden.
To rehabilitate oral speech, three primary methods are available: the electro‐larynx, esophageal speech, and tracheoesophageal speech (Ward and van As‐Brooks 2014). Tracheoesophageal speech is widely used in Western Europe and is often reported to deliver better acoustic and perceptual voice outcomes than other verbal options (van Sluis et al. 2018; van Weissenbruch et al. 1992; Ward and van As‐Brooks 2014). To achieve tracheoesophageal speech, a voice‐prosthesis (valve) is placed between the trachea and esophagus. When the patient occludes the tracheostoma, the airflow is redirected from the lungs, via the voice prosthesis into the esophagus and new pharynx (neopharynx). The airflow brings the pharyngo‐esophageal segment (PE‐Segment) in vibration, resulting in the new voice sound as seen in Figure 2.
Physiology of speaking with a voice prosthesis. Left: manually closing the tracheostoma using the Heat and Moisture Exchanger (HME), Right: speaking using a FreeHands HME. These images are used with permission from ATOS Medical, Hörby, Sweden.
Although tracheoesophageal speech is frequently regarded as the clinical gold standard for voice restoration after TL, it remains substantially different from the natural laryngeal voice in both acoustic properties and the effort required for phonation (Eadie & Doyle, 2005; Searl and Knollhoff 2018; Serra et al. 2015; Tienkamp et al. 2023; van Sluis et al. 2016). Surgical alterations to the anatomy, including the creation of a neoglottis and variations in pharyngo‐esophageal segment closure techniques (e.g., T/Y‐shaped or mucosal closure), affect airflow dynamics and phonation control (van Sluis et al. 2021). The new tracheoesophageal voice typically has a lower pitch, reduced dynamic range, shorter phonation time, and a moist or “bubbly” quality (for acoustic properties of tracheoesophageal speech, see Tienkamp et al. 2023). Speaking often requires considerable effort and coordination, and many patients experience vocal fatigue, particularly in noisy environments (Searl and Knollhoff 2018). Despite intensive speech therapy, voice quality and intelligibility outcomes vary widely, and not all patients regain effective functional communication (van Sluis et al. 2018).
During rehabilitation, patients are taught to adopt a neutral head and body posture, use abdominal breathing, and coordinate inhalation, stoma occlusion, and phonation (Perry 1997). They learn to slow their speech, reduce sentence length, and speak with relaxed neck and shoulder muscles to conserve energy and improve clarity. Two methods of stoma occlusion exist: manual closure of the Heat and Moisture Exchanger (HME) or hands‐free speech using a FreeHands HME (Lorenz et al. 2007), which incorporates a valve that automatically redirects air to the neopharynx. While hands‐free options offer increased convenience and gesture freedom, they also introduce new physical constraints such as increased airflow resistance, the need for precise posture and breathing control, and potential issues with stoma seal or valve responsiveness. Unfortunately, despite speech therapy, not every patient achieves a ‘good’ voice quality or intelligibility using tracheoesophageal speech after a TL (van Sluis et al. 2021).
In addition to physical and functional adjustments, patients who underwent TL face social and psychological challenges (Amechi et al. 2023; Babin et al. 2023; Leemans et al. 2020; Mukoyama et al. 2024; Perry et al. 2015; Sharpe et al. 2019; van Sluis et al. 2020; Wulff et al. 2022). Many feel self‐conscious or anxious about speaking publicly, especially during the early stages of rehabilitation. Concerns about how their new voice is perceived can lead to withdrawal from social interaction. Patients may also require more patience from others, as conversations can demand greater effort from both parties. Since communication is crucial in social relationships, their altered voice may significantly impact both their personal and professional lives.
Previous research on alaryngeal communication has highlighted the importance of both auditory and visual factors in speech perception and communication effectiveness. Listener perceptions vary depending on speech mode and the presence of visual cues (Bridges 1991; Evitts and Gallop 2011; Evitts et al. 2010, Evitts et al. 2021). Nonverbal behaviors such as hand movements and eye gaze also play important roles during face‐to‐face interactions with alaryngeal speakers (Evitts and Gallop 2011; Hartman and Dworkin 1982). These findings underscore that communication after TL is multimodal, involving adaptations in both speech and gestures.
Previous Research
1.2
Communication is multi‐modal. It consists of a combination of verbal and nonverbal elements, which makes it reasonable to assume that patients may adapt both their speech and body language to express themselves effectively and manage their communicative situations as successful as possible. To investigate if and how TL influences the use of verbal and nonverbal elements, a pilot study has been conducted (Neijman et al. 2022). In that pilot study, women who underwent a TL were found to use various verbal and non‐verbal techniques to compensate for their functional limitations. For instance, in the verbal aspect of communication, the women appeared to be more certain and careful in planning their utterances and reduced the syntactic complexity of their sentences. Within their non‐verbal communication, the women utilized co‐speech gestures to support their verbal communication, with beat gestures used most often.
Although the earlier pilot study yielded interesting results, caution is warranted when interpreting and generalizing its findings. The study was based on eight interviews focused on the quality of life of women who underwent a laryngectomy, and neither the interviews nor the study design was specifically intended to investigate communication adaptations. Moreover, since the study included only women, it remains unclear whether the findings apply to men, who represent a larger proportion of the TL population. While the interviews were structured, follow‐up questions introduced variability that limits direct comparability. Additionally, the functions of co‐speech gestures were not analyzed. This omission was deliberate, as research on co‐speech gestures in other patient groups, such as individuals with aphasia, indicates that examining gesture functions can provide valuable insights (Akhavan et al. 2018).
Another limitation of the pilot study includes the different control groups that were used, one group specifically for the grammar and another for the co‐speech gestures. For the grammar part, data drawn from existing dataset of recordings were used as the control group. One disadvantage of this dataset was that the speakers were not matched with the women in terms of age, gender or education. For the co‐speech gesture part, the control data consisted of annotated YouTube podcasts with semi‐public figures, who may have undergone media training that could have influenced their speech and gestures use. In other words, neither of the two control groups was directly comparable to the laryngectomized women.
The Current Study
1.3
To determine whether the findings of the pilot study are replicable, the current study systematically examines the syntactic complexity and disfluencies of spoken language and the use and function of co‐speech gestures in TL patients compared to a newly collected, matched control group. Unlike the pilot study, all data for patients and controls in the current investigation were generated specifically for this study, ensuring comparability across groups. This approach seeks to enhance the understanding of the impact of TL on adaptions within communication and provides valuable insights for speech therapy counseling and therapy. Understanding why and how TL patients adapt their communication, can help improve their communication possibilities by developing interventions that focuses on the use of gestures to enhance their communication skills and raise awareness of the impact of their disability on their language and grammar.
Analysis Framework
2
Before describing the methods in Section 3, it is important to provide an analysis framework for investigating the relevant aspects of verbal communication and co‐speech gestures. This study includes an overview of measures of syntactic complexity and disfluencies in verbal communication, as well as an understanding of how speech and gestures interact to convey meaning. In this context, “communicative adaptation” refers to the adjustments speakers make, both verbal and nonverbal, to facilitate effective communication in the face of physical or functional challenges. These adaptations may include simplifying syntactic structures, modifying lexical choices, or using co‐speech gestures to support or enhance spoken language. Clarifying this relationship provides a foundation for examining the communicative behavior observed in this study.
Syntactic Complexity in Verbal Communication
2.1
Syntactic complexity is a key component of verbal adaptation. It reflects both the number of syntactic elements combined within an utterance and the nature of the relationships among them, which together determine the cognitive resources required for production and comprehension (Bulté & Housen, 2012). Although TL constrains physical speech production, mental processing capacity remains intact. Nevertheless, the effort required to plan and produce speech may lead to shorter utterances and syntactic simplification, reflecting an adaptive strategy to convey meaning efficiently.
In this study, syntactic complexity was measured at both a global and a clause‐specific level. Global measures included the mean length per C‐unit, defined as an independent clause with its modifiers, including non‐clausal responses (see Table 1 and Appendix A), and the subordination index, which provide an omnibus indication of syntactic complexity in spoken language (Bulté & Housen, 2012; Hunt 1966). Clause‐level analyses examined the markedness of main clauses (canonical vs. non‐canonical word order) and the structural and functional properties of subordinate clauses (finite vs. non‐finite, adverbial, complement, relative, cleft, parenthetical, or non‐finite complements) (Biber et al. 1999; Hawkins 2007; Miller and Chomsky 1963). In addition, typical spoken language disfluencies, such as ellipsis, mazes, and filled and silent pauses, were analyzed to capture production effort and interactive adaptations in real‐time communication (Biber et al. 1999; Foster et al. 2000). Disfluencies are normal in spoken language, rather than an indication of production failure. Disfluencies support planning for speaking and also perform interactive roles, such as holding the floor while speaking. All measures were normalized per 100 words.
The syntactic patterns and spoken language disfluencies analyzed in this study, along with examples, are summarized in Table 1. For a full description of all measures, their definitions, and criteria for classification, see Appendix A.
Co‐Speech Gestures
2.2
In addition to verbal production, the participants’ co‐speech gestures were analyzed as part of their communicative adaptations. Gestures are movements of the hands and body that often occur alongside speech, and they can serve both addressee‐oriented and speaker‐oriented functions (Abner et al. 2015; Kendon, 2004; Özyürek, 2012). Following McNeill (1992), Neijman et al. (2022), and Özyürek (2012), gestures were classified into five types: Iconic, Metaphoric, Deictic, Beat, and Emblem. Iconic and Metaphoric gestures, grouped as Representational gestures, visually represent the content of speech, with Iconic gestures reflecting concrete referents or actions and Metaphoric gestures conveying abstract ideas or conceptual metaphors (Lakoff and Johnson 1980). Deictic gestures involve pointing to objects or abstract concepts, Beats are rhythmic movements aligned with speech prosody, and Emblems are conventionalized, culturally specific gestures that can convey meaning independently of speech (Kong et al. 2015; McNeill 1992).
Gestures were analyzed not only for their type but also for their functional role in communication. Some gestures enhance the message for the addressee (e.g., Representational gestures conveying semantic content), while others support the speaker's production processes, such as lexical retrieval or sentence structuring. Certain gestures, like Beats, may serve both the speaker and the addressee by reinforcing prosodic cues and structuring the speech flow. To ensure comprehensiveness, additional categories were included for gestures that could not be identified or for which no specific function could be deduced.
A detailed description of gesture types, functional classifications, and examples is provided in Appendix B, and an overview of types and functions used in this study is presented in Table 2.
Patients and Methods
3
Participants
3.1
Between April 2022 and March 2023, adults (≥ 18 years) who underwent TL were recruited from the institute. Eligible patients were at least six months post‐surgery and any additional treatment (such as (chemo‐) radiation therapy) used tracheoesophageal speech, and had Dutch as their first language. Participants used either manual HME closure or a hands‐free FreeHands HME for tracheoesophageal speech; the type of device was recorded for each participant, as hands‐free devices allow greater freedom for gestural movements. Patients with vision and hearing problems that prevented them from watching two animation videos and describing a picture were excluded.
In total, 21 laryngectomized patients (16 male, 5 female) and 21 matched healthy controls (14 male, 7 female) were included. Controls, matched for age, gender, education, and primarily included the patients' partners or individuals treated at the institute for other cancers. All controls underwent a brief screening/interview by a speech‐language pathologist to confirm they had no difficulties with speech, voice, hearing, or vision. See Table 3 for participant characteristics.
Procedure
3.2
Before starting the assessment, participants were instructed to sit upright with the HP Pavilion laptop (model 15‐cw1948nd) placed in front of them on the table. Behind the laptop, a SONY ZV‐E10 camera was positioned on a Rollei Mini M1 tripod to record video, focusing on the participant from the knees to the head. Additionally, a SONY IC Recorder ICD‐AX412F was placed next to the laptop to capture audio recordings in .mp3 format.
To ensure systematic data collection, each participant received the three same tasks in the same order. First, the participant was instructed to watch the short animation video “Bowling Ball” (Canary Row Series) and retell the video. The second task was to watch the short animation video “Swing” (Canary Row Series) and retell the video. The final task required participants to describe the Cookie Theft picture (Goodglass et al., 2001) in narrative form. All tasks were chosen to systematically evoke spontaneous speech. Moreover, the two Canary Row videos have been chosen, as they have been shown to be well‐suited for the elicitation of co‐speech gestures (Kita and Özyürek 2003).
Analysis
3.3
Verbal Communication
3.3.1
The analysis of verbal communication was performed by transcribing all audio‐recordings. The data collection was performed by the first author (MN), and a research assistant (MV) transcribed all recordings. MN checked all transcriptions for correctness and validity and annotated the fillers, short and long pauses, and reductions. A third researcher (BvR) annotated the communication units (C‐Units), Syntactic Constituents and Mazes, and performed the remainder of the syntactic analyzes (see Table 1 for examples). The analysis of the syntactic patterns was performed using the software program Wordsmith (Scott 2024). The annotated data were then compared between both groups, and a fourth researcher (RvS) conducted the statistical analysis.
Co‐Speech Gestures
3.3.2
The video recordings were collected by MN and annotated by a research assistant (DJ). For each participant, the onset of each co‐speech gesture was noted, and each gesture was classified by type and function according to Table 2. An individual study‐specific Excel scoring sheet was developed and used for each recording to document each gesture's onset time, as well as its type and function.
To classify gestures functionally as serving either as lexical support or prosodic aid, a conservative approach was applied: only gestures clearly serving a lexical function were labeled as such. In ambiguous cases, gestures were categorized as prosodic aids.
Prior to annotation, MN and DJ completed a practice session on a video outside the study database to ensure familiarity with the coding scheme and consistency. MN reviewed 10% of the annotations to assess interrater reliability, which showed excellent agreement (Cohen's κ = 0.87). The annotated data were then compared between both groups, with RvS performing the statistical analyses and RP assisting in interpretation and identifying gesture types and functions.
Statistical Analysis
3.4
Statistical analyses were conducted using R software (version 4.2.1). Descriptive statistics, including median and range, were calculated to summarize participant characteristics. For the verbal communication, difference in length of spoken text between participants was accounted for by normalizing frequency counts to 100 words. The data were normalized by scaling all measures to a standard of 100 words per participant, ensuring a fair comparison across groups regardless of differences in total word count. The study outcomes (syntactic complexity and co‐speech gestures) were analyzed using non‐parametric Wilcoxon Rank‐Sum test, with the False Discovery Rate (FDR) correction applied to account for multiple testing. Statistical significance was defined as a p‐value less than 0.05.
Results
4
All 42 participants completed the tasks. No statistically significant differences were found in the total number of words used or in the speech rate (words per minute) between the TL group and the control group (see Table 4).
Verbal Communication
4.1
Table 4 provides an overview of the outcomes for syntactic complexity and spoken‐language disfluencies. One of the two omnibus measures of syntactic complexity, the average length of the C‐unit, was significantly shorter for the TL group (W = 110, p = 0.019), but no significant difference was observed for the number of subordinate clauses per C‐unit. The more specific syntactic measures show no differences, with similar proportions of non‐canonical syntax in the main clauses and similar proportions of non‐finite clauses among the subordinate clauses. The functional distribution of the subordinate clause types is almost identical too, as Figure 3 shows.
Subordinate clause function. Abbreviations: TL, total laryngectomy; Wh‐Cleft, Wh‐cleft clauses; verb_complex, verb complex; relative, relative clause; parenthetical, parenthetical clause; complement, complement clause; adverbial, adverbial clause.
The differences between the groups were clearer when the typical disfluencies of spoken language are considered. The TL group used significantly fewer fillers (W = 108, p = 0.019) and had significantly fewer mazes than the control group (W = 109, p = 0.019). Conversely, the TL group had significantly more short pauses than the control group (W = 356, p = 0.001). Reduced clauses and long pauses did not differ significantly between the two groups, though.
Co‐Speech Gestures
4.2
Gesture production varied widely within both groups. Table 5 presents the number of used co‐speech gestures per group across the three tasks. The majority of participants in both groups produced less than 10 gestures in total. Three participants from the TL group used 21 or more gestures. Two of them used a non‐FreeHands HME, while one participant with a FreeHands HME was an outlier, producing a total of 41 gestures.
Table 6 presents the frequencies of the types and functions of co‐speech gestures per group across the three tasks. Regarding the types of co‐speech gestures, Iconic and Beat gestures were the most commonly used in both groups. Similarly, the function of co‐speech gestures was comparable between the groups, with both the TL group and the Control group using their co‐speech gestures primarily to enhance and reinforce intonation. No gestures were found to simultaneously serve both functions.
When normalizing the data to 100 words, no statistically significant differences were found in the total number or types of co‐speech gestures between the TL group and the control group (see Table 7).
Discussion
5
This study systematically explored the syntactic complexity of spoken language, along with the use and function of co‐speech gestures, in a selected group of patients who have undergone TL compared to a matched control group. Results revealed significant differences in a few dimensions of spoken language disfluencies and a single omnibus measure of syntactic complexity. No significant differences were found in the use or type of co‐speech gestures between both groups, meaning that the TL group use a comparable amount and the same type of co‐speech gestures, even though most of them could use only one hand to produce go‐gestures. Overall, the laryngectomy group produced fewer words in total on the tasks, slightly shorter C‐units, fewer verbal disfluencies and more short pauses (for breathing). These findings align with the hypothesis that laryngectomized individuals adapt their multimodal communication strategies, consciously or unconsciously, to their functional abilities. Such adaptation is consistent with broader theories of communicative accommodation and cognitive control, which suggest that speakers adjust their communicative behavior on situational demands and individual capacities (Green and Abutalebi 2013), even though these theories were originally developed in the context of bilingualism.
Verbal Communication
5.1
The analysis reveals that only a single omnibus syntactic measure, words per C‐unit, differs significantly between the TL and control group. However, none of the more refined syntactic measures, including the subordination index, reveals significant differences. It appears as if the TL group is simply a little more parsimonious in their word choices to yield slightly shorter C‐units, without making use of different degrees non‐canonical main‐clause syntax or non‐finite subordinate clauses, nor different types of subordination. The fact that their constraint is mainly physical and not cognitive appears to support their ability to use similar syntax than their counterparts in the control group.
A different picture emerges once one considers the typical disfluencies of spoken language. The TL group, possibly due to training during speech therapy, used more frequent short pauses to breathe, while they avoided other typical disfluencies such as filled pauses and mazes. They used silent pauses, which not only gives them opportunity to breathe, but also simultaneously some time to think and plan ahead (Bohnenkamp et al. 2011; Stajner‐Katusić et al. 2006; Stepp et al. 2008), which ties in with the finding that their speech shows significantly fewer disfluencies of the kind that were classified as mazes. Speech timing and pause patterns in the TL group reflect adaptations to altered respiratory and phonatory function after TL (Bohnenkamp 2008; Stepp et al. 2008). Moreover, the TL group also uses fewer filled pauses, which are typical of spoken language conversation, but do require more effortful production of airflow and phonation (Grolman et al. 2008; Searl 2020; Searl and Knollhoff 2018). The combination of more silent pauses and fewer filled pauses may therefore cause trouble for the TL group in regular conversation, since they are less able to signal their intent to hold the floor, while their silent pauses may invite other conversation partners to try to usurp their speech turns. In the context of the present experiment, with a helpful conversation partner that did not try to compete with the speakers for the floor, this eventually did not come to pass, though.
When everything is considered, the TL group is not syntactically constrained in comparison to the control group. They find the physical act of speaking more challenging, and deal with this challenge through pauses and slightly fewer words per C‐units, while compensating through more extensive planning. The resulting speech production is thus of similar diversity and complexity, in contrast to the findings of the pilot study. The differences pertain more to the management of speech turns, a social challenge, and not to the cognitive challenge of conveying the intended message clearly.
Co‐Speech Gestures
5.2
Despite producing fewer words overall, the TL group used a comparable number of co‐speech gestures to controls, consistent with prior research showing that gestures are tightly integrated with speech (Neijman et al. 2022). When speech production is less efficient, as in the case of TL patients, gestures may serve as a complementary strategy to support verbal communication. Multi‐modal language production support this by demonstrating the interdependence of speech and gesture during message formulation (Emmorey et al. 2008; Kita and Özyürek 2003; Özyürek, 2012).
Gesture production varied within both groups. Most TL participants (18/21) used a regular HME, leaving only one hand free for gesturing, highlighting their adaptability. Three TL participants used a FreeHands HME, allowing two‐handed gesturing, with one producing an unusually high number of gestures.
Contrary to expectations, TL participants did not rely more heavily on co‐speech gestures as a compensatory strategy, and differences in syntactic complexity were smaller than expected. Both groups primarily used Beat and Iconic gestures similarly, reinforcing speech rhythm and meaning, respectively. Neither group produced Emblems, likely due to the structured and non‐interactive nature of the tasks.
No gestures were found to simultaneously serve both functions (lexical support and prosodic aids). Prior to annotation, the annotators jointly practiced on data outside the study sample to ensure consistent application of decision rules. This approach may have led to an underestimation of lexical gestures but ensured reliable classification.
The equal use of gestures to reinforce intonation across groups was surprising, given the vocal changes in the TL group. This may indicate effective compensatory strategies, possibly relying on deliberate speech pacing or other methods to achieve similar prosodic reinforcement.
These findings align with prior work emphasizing the importance of visual cues in alaryngeal communication (Bridges 1991; Doyle et al. 2023; Evitts et al. 2010, 2011, Evitts et al. 2021; Hartman and Dworkin 1982). Unlike previous studies focusing on natural conversation or audiovisual presentations, our structured tasks show that co‐speech gesture use remains a stable and integrated communicative feature in TL speakers, despite their functional limitations.
Limitations
5.3
This study has several limitations that should be considered when interpreting and generalizing the results. Although the design of the study aimed to systematically stimulate spontaneous speech and the use of co‐speech gestures by having participants retell two animated videos and describe a picture, conversational contexts were excluded. This structured approach may limit the applicability of the findings to natural conversational settings.
Furthermore, the comparison in this study was between individuals. The use of syntactic complexity and co‐speech gestures is, however, personal. This study lacked of a pre‐measurement means that within‐subject comparisons before and after surgery were not possible, limiting the ability to assess individual changes in communication strategies over time. As a result, it remains unclear whether observed differences in nonverbal communication and gesture use are due to the effects of surgery or were already present beforehand. A pre‐operative baseline would have allowed for a more precise evaluation of how patients adapt their communication post‐surgery.
In addition, all participants completed the same three tasks in a fixed order: two short animated videos followed by a picture description. This fixed order was chosen to ensure systematic and consistent data collection across participants. Although this approach may raise concerns about potential order effects, such as fatigue or practice effects, the brief nature of the tasks (each video lasting approximately 30 seconds) makes such effects unlikely. Furthermore, since our analyses did not involve comparing performance across the different tasks, possible order effects are not expected to impact the main findings. Nevertheless, future studies could consider counterbalancing task order or employing a crossover design to further control for any order‐related influences.
Moreover, partners were included as control participants to match on age, gender, and education, which helped control for demographic variables. While this ensured demographic comparability, it may introduce potential relationship bias, as partners could share environmental or behavioral traits. This was considered during study design and is acknowledged as a limitation; therefore, results involving controls should be interpreted with due caution. Importantly, the participant and control groups were reasonably balanced for gender (16 M/5F in patients vs. 14 M/7F in controls) and age (mean 69.1 vs. 69.2 years), which reduces the likelihood of confounding effects. Due to the small sample size, statistical testing of potential gender differences in gesture use was not feasible. We acknowledge that previous research suggests that there may be differences in co‐speech gesture use between individuals assigned male versus female gender at birth (Briton et al. 1995; LaFrance 1981; Saucier and Elias 2001; Yang 2010); future studies with larger and more balanced samples could explore these potential gender differences. Additionally, no power analysis was conducted before the study, which may limit the ability to detect smaller effects and impact the reliability of the results. Future studies should include a power analysis to ensure adequate statistical power.
Future Research
5.4
Future research could investigate if the communicative adaptions found in this study also occur in a more dynamic and varied communicative settings, such as informal conversations or group discussions, to determine how syntactic complexity and gesture use may differ in less structured contexts. Furthermore, studies should consider incorporating pre‐ and post‐surgical assessments to better understand the communicative changes and their potential impact on daily communication. Developing informative materials for speech and language therapists, future patients undergoing TL, and their loved ones could provide valuable information and help manage expectations in preparation for the surgery. Additionally, speech and language therapists may benefit from the development of targeted therapies to support effective communication adaptations for individuals post‐TL.
Conclusion
6
In conclusion, this study demonstrates that, as observed in structured tasks, the TL patients adapt their use of spoken‐language disfluencies to buy time, resulting in minimal difference in syntactic complexity compared to a matched control group. Their use of co‐speech gestures, in both type and frequency, is similarly comparable to controls. Taken together, these findings suggest that although TL affects verbal fluency, gestures remain intact and can be used in rehabilitation and counseling, with training in both disfluencies and gestures helping to support more effective communication.
Funding
The authors received no financial support for this research.
Ethical Approval and Consent to Participate
The study was approved by the Institutional Review Board (IRBd21‐226), and all participants provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abner, N. , K. Cooperrider , and S. Goldin‐Meadow . 2015. “Gesture for Linguists: A Handy Primer.” Language and Linguistics Compass 9, no. 11: 437–449. 10.1111/lnc 3.12168.26807141 PMC 4721265 · doi ↗ · pubmed ↗
- 2Akhavan, N. , T. Göksun , and N. Nozari . 2018. “Integrity and Function of Gestures in Aphasia.” Aphasiology 32, no. 11: 1310–1335. 10.1080/02687038.2017.1396573. · doi ↗
- 3Altmann, L. J. P. , and M. S. Troche . 2011. “High‐Level Language Production in Parkinson's Disease: A Review.” Parkinson's Disease 2011: Article 238956. 10.4061/2011/238956.PMC 315391821860777 · doi ↗ · pubmed ↗
- 4Amechi, C. , L. Ottenstein , A. Lang , et al. 2023. “Quality of Life and Decisional Regret After Total Glossectomy With Laryngectomy: A Single‐Institution Case Series.” Oral Oncology 142: 106434. 10.1016/j.oraloncology.2023.106434.37220704 · doi ↗ · pubmed ↗
- 5Babin, E. , N. Heutte , M. Humbert , and O. Laccourreye . 2023. “Sex‐Related Quality of Life After Total Laryngectomy for Cancer.” European Annals of Otorhinolaryngology, Head and Neck Diseases 140, no. 3: 121–126. 10.1016/j.anorl.2023.04.001.37142505 · doi ↗ · pubmed ↗
- 6Biber, D. , et al. 1999. Longman Grammar of Spoken and Written English. Pearson Education Ltd.
- 7Bohnenkamp, T. A. 2008. “The Effects of a Total Laryngectomy on Speech Breathing.” Current Opinion in Otolaryngology & Head and Neck Surgery 16, no. 3: 200–204. 10.1097/MOO.0b 013e 3282 fe 96ac.18475071 · doi ↗ · pubmed ↗
- 8Bohnenkamp, T. A. , K. M. Forrest , B. K. Klaben , and J. M. Stager . 2011. “Lung Volumes Used During Speech Breathing in Tracheoesophageal Speakers.” The Annals of Otology, Rhinology, and Laryngology 120, no. 8: 550–558. 10.1177/000348941112000811.21922981 · doi ↗ · pubmed ↗