Prevalence of anxiety and associated risk factors among maternal and child health hospital female attenders: a cross-sectional multicenter study
Cheng Song, Jia Tang, Zhixin Shi, Shiru Tang, Zirui Wang, Guanlin Zhang, Siyuan Liu, Xu Chen, Yueping Song

TL;DR
This study found that 30.5% of women at maternal and child health hospitals in Henan Province had anxiety, with risk factors including hospital type and low health knowledge.
Contribution
The study identifies specific risk factors for anxiety among MCH hospital attendees in China, emphasizing the role of hospital grade and maternal health literacy.
Findings
Anxiety prevalence was 30.5% among MCH hospital attendees in Henan Province.
Women in Grade A tertiary hospitals had higher anxiety compared to those in other hospitals.
Lower maternal health knowledge and self-efficacy in healthcare access were linked to increased anxiety.
Abstract
Maternal anxiety represents a substantial public health concern, particularly among women who are attending Maternal and Child Health (MCH) hospitals. This study investigated anxiety prevalence and risk factors among MCH hospital female attenders in Henan Province, a region demographically representative of national trends, during the peak winter medical demand of December 2024. A cross-sectional study using convenience sampling was implemented to recruit 745 maternal participants from 5 MCH hospitals (comprising three Grade A tertiary hospitals and two other hospitals) in Henan Province of China during December 2024. Maternal anxiety was assessed using the Generalized Anxiety Disorder 7-item scale (GAD-7). Knowledge regarding maternal and child healthcare and self-efficacy in accessing healthcare services were evaluated using the self-developed Maternal and Child Health Knowledge…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
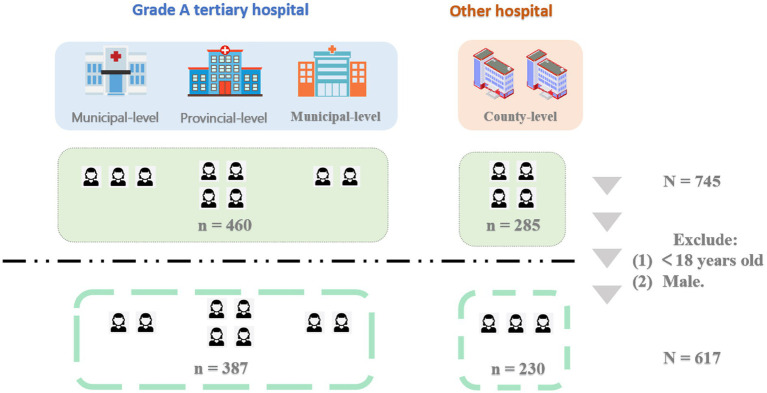 Figure 1
Figure 1| Characteristics | Number (%) |
|---|---|
| Age (years) | |
| 18–44 | 529 (85.7) |
| ≥45 | 88 (14.3) |
| Marital status | |
| Married | 525 (85.10) |
| Unmarried/divorced/widowed | 92 (14.90) |
| Ethnic groups | |
| Han | 613 (99.4) |
| Other | 4 (0.6) |
| Education level | |
| Senior high school or below | 279 (45.2) |
| Above senior high school | 338 (54.8) |
| Occupational status | |
| Unemployed | 165 (26.7) |
| Retired | 17 (2.8) |
| Employed | 435 (70.5) |
| Self-reported health status | |
| Unhealth | 100 (16.2) |
| Health | 517 (83.8) |
| Hospitalization in the past year | |
| No hospitalization | 511 (82.9) |
| Hospitalized | 106 (17.1) |
| Hospital level | |
| Other hospital | 230 (37.3) |
| Grade A tertiary hospital | 387 (62.7) |
| Specific departments | |
| Maternity healthcare department | 157 (25.4) |
| Pediatric healthcare department | 148 (24.0) |
| Gynecological healthcare department | 158 (25.6) |
| Reproductive health services department | 154 (25.0) |
| Variable | Number (%) | Mean (SD) | Range |
|---|---|---|---|
| Anxiety | |||
| Yes | 188 (30.5) | ||
| No | 429 (69.5) | ||
| Anxiety | |||
| Total score | 3.14 (3.71) | 0–21 | |
| Knowledge | |||
| Total score | 20.13 (6.95) | 6–30 | |
| SEHA | |||
| Total score | 31.46 (4.23) | 7–35 | |
| Characteristics | Anxiety | |
|---|---|---|
| OR (95%CI) | ||
| Age (years) | ||
| 18–44 | 0.929 (0.572–1.510) | 0.767 |
| ≥45 | 1 | |
| Marital status | ||
| Married | 0.890 (0.554–1.429) | 0.629 |
| Unmarried/divorced/widowed | 1 | |
| Ethnic group | ||
| Han | 1.317 (0.136–12.743) | 0.812 |
| Other | 1 | |
| Education level | ||
| Senior high school or below | 0.780 (0.551–1.103) | 0.160 |
| Above senior high school | 1 | |
| Occupational status | ||
| Unemployed | 0.758 (0.509–1.130) | 0.174 |
| Retired | 0.447 (0.126–1.580) | 0.211 |
| Employed | 1 | |
| Self-reported health status | ||
| Unhealth | 0.843 (0.505–1.407) | 0.514 |
| Health | 1 | |
| Hospitalization in the past year | ||
| No hospitalization | 0.790 (0.491–1.272) | 0.332 |
| Hospitalized | 1 | |
| Hospital level | ||
| Grade A tertiary hospital | 2.318 (1.580–3.402) | 0.001* |
| Other hospital | 1 | |
| Specific departments | ||
| Maternity healthcare department | 0.531 (0.326–0.864) | 0.011* |
| Reproductive health services department | 0.601 (0.371–0.974) | 0.039* |
| Gynecological healthcare department | 0.657 (0.409–1.056) | 0.083 |
| Pediatric healthcare department | 1 | |
| Knowledge | 0.956 (0.932–0.980) | 0.001* |
| SEHA | 0.947 (0.910–0.985) | 0.007* |
| Characteristics | Anxiety | |
|---|---|---|
| AOR (95%CI) | ||
| Education level | ||
| Senior high school or below | 0.968 (0.639–1.467) | 0.878 |
| Above senior high school | 1 | |
| Occupational status | ||
| Unemployed | 0.788 (0.494–1.257) | 0.317 |
| Retired | 0.331 (0.088–1.249) | 0.103 |
| Employed | 1 | |
| Hospital level | ||
| Grade A tertiary hospital | 2.278 (1.515–3.425) | 0.001* |
| Other hospital | 1 | |
| Specific departments | ||
| Maternity healthcare department | 0.501 (0.302–0.830) | 0.007* |
| Reproductive health services department | 0.584 (0.355–0.961) | 0.034* |
| Gynecological healthcare department | 0.683 (0.417–1.118) | 0.129 |
| Pediatric healthcare department | 1 | |
| Knowledge | 0.967 (0.940–0.995) | 0.021* |
| SEHA | 0.954 (0.913–0.997) | 0.037* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Music Therapy and Health · Family and Patient Care in Intensive Care Units
Introduction
1
Maternal anxiety is a significant complication that extends well beyond the perinatal period, impacting women across multiple stages of reproductive and child-rearing life. Multiple independent studies indicated that anxiety during the perinatal period can adversely affect maternal wellbeing and is increasingly linked to suboptimal child health outcomes including an elevated risk of neurodevelopmental disorders (Zhang et al., 2021; Zhang et al., 2023). While research has extensively documented anxiety among perinatal women in obstetric settings (Zhong et al., 2025; Nisar et al., 2025; Yang et al., 2025), far less is known about anxiety among women who utilize Maternal and Child Health (MCH) services beyond perinatal care.
In China, the MCH system functions as a comprehensive healthcare gateway, providing not only perinatal services but also routine gynecological examinations, fertility treatments, and pediatric care for children. Each of these clinical contexts introduces distinct stressors, whether related to diagnostic uncertainty, fertility pressures, or the ongoing management of a child’s health, all of which may initiate or amplify anxiety (Ahorsu et al., 2022; Lu et al., 2021; Zhu et al., 2021; Li et al., 2022). Nevertheless, mental health screening and support within MCH settings remain narrowly focused on the perinatal period, leaving a critical gap in understanding and addressing anxiety among the broader population of MCH service users. This gap is particularly salient in China, where systemic surveys of anxiety in non-perinatal MCH attendees are scarce, and associated social determinants are poorly understood (Zhu et al., 2025; Yang and Yu, 2023). The unaddressed anxiety can undermine both maternal mental health and the effectiveness of other health interventions, thereby affecting overall maternal and child wellbeing. Furthermore, anxiety within these complex medical environments is often exacerbated by a sense of unfamiliarity and helplessness. Limited health literacy and low self-efficacy in navigating the healthcare system can impair a woman’s ability to access information and manage care effectively, thereby acting as significant psychological drivers of anxiety. To address this, our study aims to characterize the anxiety level within this critical population in Henan province, China.
Methods
2
Ethical consideration and funding
2.1
This study was approved by the Ethics Review Committee of the School of Population and Health, Renmin University of China (approval date: 2024-11-28). All participants provided written informed consent prior to their inclusion. This work was supported by the Big Data and Responsible Artificial Intelligence for National Governance and Center for Population and Development Studies, Renmin University of China. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Study design and participants
2.2
We conducted a cross-sectional study in Henan province, one of China’s most populous provinces with a demographic profile that closely mirrors the national average in terms of age-sex distribution, urban–rural composition, and socioeconomic gradients. Its healthcare system encompasses well-developed tertiary hospitals in urban centers as well as secondary and primary institutions in rural areas, representing the tiered structure of China’s MCH service network. Therefore, findings from Henan can offer insights with strong external validity for central China and provide a valuable reference for similar settings nationwide. Participants were recruited using a convenience sampling strategy from five MCH hospitals, stratified to represent different tiers of the healthcare system: one provincial-level, two municipal-level, and two county-level hospitals. Given the high outpatient volume during the peak winter season and limited onsite resources, convenience sampling was selected as the most feasible approach to ensure efficient data collection without disrupting clinical operations.
The inclusion criteria were defined as follows: (1) Biological females aged ≥18 years; (2) Current utilization of outpatient services in one of four designated departments: Maternity Healthcare (pregnant/postpartum women), Pediatric Healthcare (mothers or female guardians accompanying children), Gynecological Healthcare, or Reproductive Health Services; (3) Ability to communicate in Chinese and complete the questionnaire independently. A total of 745 participants completed the questionnaire. The following participants were excluded: (1) those who are under 18 years old, (2) male population. Ultimately, 617 participants were included in the final analysis of this study based on the above criteria (Figure 1).
Flowchart of participant inclusion.
Assessment tools
2.3
Anxiety
2.3.1
Anxiety symptoms were assessed using the 7-item Generalized Anxiety Disorder scale (GAD-7) (Spitzer et al., 2006; Shih et al., 2022). Each item is rated on a 4-point Likert scale, from 0 (“not at all”) to 3 (“nearly every day”), with total scores ranging from 0 to 21. A score of ≥5 was used as the cutoff to indicate clinically significant anxiety symptoms, a threshold widely validated for screening purposes. In the present study, the GAD-7 demonstrated excellent internal consistency (Cronbach’s α = 0.945).
Level of knowledge regarding maternal and child healthcare (knowledge)
2.3.2
The level of knowledge was measured by 6 items.
Attending community-based lectures on maternal and child healthcare within my residential neighborhood.Participating in maternal and child healthcare seminars at hospitals or community health service centers.Reviewing educational materials on maternal and child health distributed by the neighborhood committee.Utilizing community- or street-level maternal and child health consultation services.Examining maternal and child healthcare leaflets provided by hospitals or community health service centers.Accessing and reading promotional materials on maternal and child health via online platforms (e.g., official websites, WeChat public accounts).
Each item was rated on a 5-point Likert scale, ranging from 1 (“never”) to 5 (“often”). A total score was calculated by summing the responses to all six items, with a possible range of 6 to 30. Higher scores indicate a greater frequency of proactive health information-seeking behavior. In the present study, this scale demonstrated excellent internal consistency (Cronbach’s α = 0.932).
Self-efficacy in healthcare access (self-efficacy)
2.3.3
The level of Self-Efficacy in Healthcare Access (SEHA) was measured by 7 items.
I am knowledgeable about how to schedule prenatal examinations or book other MCH services.I can comprehend the recommendations and guidance provided by healthcare professionals.I am aware of which MCH services are reimbursable under my medical insurance.Even when faced with certain challenges (e.g., time constraints, transportation barriers), I am capable of arranging appointments for MCH services.With the support of physicians, I am confident in my ability to effectively address my health issues and attain the desired health outcomes.I am able to adhere strictly to the follow-up schedules and health-management recommendations prescribed by my physician.When selecting an MCH services provider, I proactively gather information and make the choice that best suits my needs.
Responses were captured on a 5-point Likert scale, from 1 (“Strongly disagree”) to 5 (“Strongly agree”). The total score was computed by summing the ratings for all seven items, yielding a potential range of 7 to 35. Higher scores reflect a stronger sense of self-efficacy in accessing and managing healthcare. This scale demonstrated excellent internal consistency in this sample (Cronbach’s α = 0.964).
Covariates
2.3.4
We collected data on several demographic and clinical variables. Sociodemographic information include age (categorized as 18–44 vs. ≥45 years), marital status (married vs. unmarried/divorced/widowed), ethnicity (Han vs. other), education level (senior high school or below vs. above senior high school), and occupational status (employed vs. unemployed/retired).
Clinical and healthcare-related characteristics included self-reported health status (healthy vs. unhealthy) and hospitalization in the past year (yes vs. no). Information on the hospital level (tertiary vs. secondary) and the specific department visited (Maternity Healthcare, Pediatric Healthcare, Gynecological Healthcare, or Reproductive Health Services) was obtained from administrative records at the time of recruitment.
Statistical analysis
2.4
Descriptive statistics (frequencies, percentages, means, and standard deviations) were used to summarize participant characteristics. The primary outcome, anxiety, was treated as a binary variable (GAD-7 score ≥5 vs. <5).
We employed a two-step logistic regression modeling strategy. First, univariate logistic regression analyses were conducted to examine the unadjusted association between each potential predictor and anxiety. To avoid prematurely excluding potentially important variables, all factors with a p-value < 0.20 in the univariate analyses were selected as candidate variables for the multivariate model.
Second, a multivariate logistic regression model was built to identify independent factors associated with anxiety. The final model included the candidate variables identified in the first step. Results are presented as Odds Ratios (ORs) for univariate analyses and Adjusted Odds Ratios (AORs) for the multivariate analysis, both with 95% Confidence Intervals (CIs). A two-tailed p-value < 0.05 was considered statistically significant. All analyses were performed using R 4.2.1.
Results
3
Demographic characteristics of participants
3.1
Among 617 participants, 85.1% were married and 99.4% were identified as Han ethnicity. More than half of participants (54.8%) had received education beyond senior high school. Regarding employment status, 70.5% were currently employed, while 26.7% were unemployed and 2.8% were retired. In terms of health status, 83.8% of participants self-reported being in good health, and 17.1% had experienced hospitalization in the past year. Most participants (62.7%) received care at tertiary-level MCH hospitals, with the remaining 18.1% attending secondary-level hospitals. Participants were evenly distributed across four key departments: Maternity Healthcare (25.4%), Pediatric Healthcare (24.0%), Gynecological Healthcare (25.6%), and Reproductive Health Services (25.0%). This distribution reflects the diverse clinical services utilized by MCH services users within the MCH system. These demographic characteristics provide essential context for understanding the variability in anxiety levels and related risk factors observed in subsequent analyses (Tables 1, 2).
Univariate analysis of demographic and anxiety in participants
3.2
The results of univariate analysis of anxiety were shown in Table 3. The factors associated with anxiety among participants were: hospital level (Grade A tertiary hospital, OR = 2.318, 95% CI = 0.294–0.633), specific departments (maternity healthcare department, OR = 0.531 95% CI = 0.326–0.864; reproductive health services department, OR = 0.601, 95% CI = 0.371–0.974), knowledge (OR = 0.956, 95% CI = 0.932–0.980) and self-efficacy (OR = 0.947, 95% CI = 0.910–0.985).
Multivariate analysis of demographic and anxiety in participants
3.3
The results of univariate analysis of anxiety were shown in Table 3. Service users in Tertiary Class A hospitals showed higher vulnerability to anxiety symptoms than their counterparts in other tertiary hospitals (AOR = 0.439 for other tertiary hospitals; 95% CI = 0.292–0.660). Additionally, being in the Paediatric Department was a stronger risk factor than being in the Maternity Department (AOR = 0.501) or reproductive services (AOR = 0.584). Higher knowledge (AOR = 0.967, 95% CI = 0.940–0.995) and self-efficacy (AOR = 0.954, 95% CI = 0.913–0.997) showed the protective factor to anxiety symptoms (Table 4).
Discussion
4
This study provides a unique insight into the prevalence and determinants of anxiety symptom among women utilizing MCH services in Henan, China. By moving beyond the traditional focus on the perinatal period, our findings provide a reference for the mental health landscape of women across various stages of reproductive and maternal life. We identified a substantial prevalence of anxiety symptom and, more importantly, uncovered key modifiable factors related to both healthcare system structure and individual patient behaviors that are associated with this burden. Existing research has predominantly focused on specific populations such as pregnant and postpartum women, with a notable dearth of studies investigating the clinically significant group of MCH services users in MCH hospital (Lähdepuro et al., 2024; Nolvi et al., 2019; Nath et al., 2019). Our research effectively bridges this gap, intending to offer valuable insight for clinical practice.
Our findings reveal a considerable anxiety symptom prevalence rate of 30.5% (95% CI: 26.8–34.1%) among MCH services users who attended medical consultations at MCH hospitals in Henan province, underscoring a substantial mental health concern within this population. Given that previous studies have primarily focused on perinatal anxiety rather than the broader MCH population, direct comparisons are challenging. However, this 30.5% prevalence rate suggests that the mental health burden in this mixed clinical setting—which encompasses not only pregnancy-related stress but also the anxiety associated with pediatric illness and gynecological conditions—is substantial and warrants urgent attention.
A key finding of our research is the significant variation in anxiety symptom levels across different level MCHs. Women attending grade A tertiary hospitals reported significantly higher anxiety symptom than those at other hospitals. This may reflect the differences in caseload complexity, patients’ expectation, or the institutional environment itself among grade A tertiary hospitals and other hospitals. Grade A tertiary hospitals often manage more severe or complex cases, which can create a more stressful atmosphere for patients. In China, these top-tier facilities are frequently characterized by overcrowding and intricate referral bureaucracies. Patients often endure long queues only to receive brief consultation sessions, leading to a rushed and impersonal care experience. This result suggests that strengthening mental health support at the tertiary level, where the clinical and psychological stakes are often highest, is a critical priority.
Furthermore, our data revealed that women visiting the pediatric department experienced the highest levels of anxiety symptom. This finding is consistent with literature underscoring the profound psychological toll that a child’s health issues can exert on a mother (Ueki et al., 2015). The acute, often uncontrollable, nature of pediatric health concerns appears to be a more potent driver of anxiety symptom than the challenges faced in maternity or reproductive health settings. This powerfully argues for embedding maternal mental health support directly within pediatric care models, recognizing that a mother’s wellbeing is inextricably linked to that of her child (Avan et al., 2023; Ueki et al., 2014).
Perhaps our most actionable finding relates to the individual-level protective factors we identified. We found that more frequent engagement in health information-seeking behaviors and higher self-efficacy in accessing healthcare were both independently associated with a lower likelihood of anxiety symptom. This moves beyond the simplistic notion that merely “knowing more” reduces anxiety symptom. Instead, it suggests that the proactive process of seeking information is a key component of an adaptive coping strategy. By actively engaging with health resources, women may enhance their sense of control, improve their ability to navigate complex healthcare systems, and build confidence in their decision-making—all of which are potent buffers against anxiety symptom (Zhu et al., 2025). Specifically, improving ‘navigational’ self-efficacy can reduce the ‘learned helplessness’ often felt in large hospitals. This finding has direct implications for intervention design: efforts should not only focus on disseminating information but also on empowering women by lowering barriers to access and cultivating the skills and confidence needed to become active participants in their own healthcare (Liu et al., 2023; Shephard et al., 2019).
The distinct patterns of anxiety symptom identified across different clinical settings and individual characteristics underscore the urgent need for a more integrated approach to mental health within routine MCH care. Our findings strongly suggest that, despite considerable progress in China’s healthcare coverage and accessibility, maternal mental health services remain insufficiently developed and underutilized. Previous studies conducted in high-income countries have consistently demonstrated the benefits of early detection and treatment of maternal anxiety, emphasizing that anxiety management during the antenatal and postnatal periods is crucial in improving both maternal and infant health outcomes (Laurenzi et al., 2020). Evidence from longitudinal studies highlights that untreated maternal anxiety can lead to complications such as preterm birth, low birth weight, postpartum depression, and developmental impairments in children (Galler et al., 2004; Padovani et al., 2011). Our findings reinforce these observations, emphasizing the need for systematic screening programs within antenatal care frameworks to proactively identify and manage anxiety.
Several limitations of this study should be acknowledged when interpreting the findings. First, the cross-sectional design inherently precludes the establishment of causal relationships; while we identified strong associations, we cannot determine whether, for instance, lower self-efficacy leads to anxiety symptom or if anxiety symptom erodes an individual’s self-efficacy over time. Future research should employ longitudinal or prospective cohort designs to delineate these temporal and potentially bidirectional pathways. Second, our reliance on a convenience sampling strategy, although geographically stratified across different hospital tiers, may limit the generalizability of our prevalence estimates to the entire population of Henan province. Future studies using probability-based sampling methods would provide more robust population-level estimates. Third, all key measures, including the primary outcome of anxiety symptom, were based on self-report questionnaires, which are susceptible to social desirability and recall biases. While the GAD-7 is a well-validated tool, it does not replace a formal clinical diagnosis. The inclusion of objective clinical assessments or a two-stage screening design in future research could yield more precise diagnostic information. Fourth, our self-developed scales for information-seeking behavior and self-efficacy, while demonstrating excellent internal consistency, have not yet undergone formal external validation or test–retest reliability analysis. Further psychometric evaluation of these instruments in diverse populations is warranted. Finally, while our multivariate model adjusted for several key demographic and clinical factors, the possibility of residual confounding from unmeasured variables, such as socioeconomic status, social support, or personal psychiatric history, cannot be entirely ruled out. Future investigations should aim to incorporate a more comprehensive set of potential confounders to provide a more nuanced understanding of the determinants of maternal anxiety symptom.
Conclusion
5
In conclusion, this study highlights that anxiety symptom is a significant public health concern among the diverse population of women served by MCH hospitals in China, particularly within Pediatric Departments and Grade A tertiary hospitals. The identification of key modifiable risk factors, including the hospital level, clinical department, and individual factors such as woman’s confidence and proactivity in engaging with the healthcare system. Our findings strongly advocate for the integration of accessible mental health services within existing frameworks, specifically recommending that maternal anxiety screening be conducted during pediatric consultations. Additionally, increasing support for hospital navigation is essential to boost women’s confidence. By addressing these identified risk factors through evidence-based policy interventions and refined clinical practices, guided by both our findings and global best practices, there is immense potential to improve maternal mental health outcomes and, consequently, enhance overall maternal wellbeing across the region and beyond.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahorsu D. K. Imani V. Lin C. Y. Timpka T. Broström A. Updegraff J. A. . (2022). Associations between fear of COVID-19, mental health, and preventive behaviours across pregnant women and husbands: an actor-partner interdependence modelling. Int. J. Ment. Heal. Addict. 20, 68–82. doi: 10.1007/s 11469-020-00340-x, 32837427 PMC 7289236 · doi ↗ · pubmed ↗
- 2Avan B. I. Hameed W. Khan B. Asim M. Saleem S. Siddiqi S. (2023). Promoting supportive and respectful maternity care in public health facilities in Sindh, Pakistan: a theory-informed health system intervention. Glob. Health Sci. Pract. 11:e 2200513. doi: 10.9745/ghsp-d-22-00513, 37348940 PMC 10285721 · doi ↗ · pubmed ↗
- 3Galler J. R. Ramsey F. C. Harrison R. H. Taylor J. Cumberbatch G. Forde V. (2004). Postpartum maternal moods and infant size predict performance on a national high school entrance examination. J. Child Psychol. Psychiatry 45, 1064–1075. doi: 10.1111/j.1469-7610.2004.t 01-1-00299.x, 15257663 · doi ↗ · pubmed ↗
- 4Lähdepuro A. Räikkönen K. Pham H. Thompson-Felix T. Eid R. S. O'Connor T. G. . (2024). Maternal social support during and after pregnancy and child cognitive ability: examining timing effects in two cohorts. Psychol. Med. 54, 1661–1670. doi: 10.1017/s 0033291723003550, 38087866 · doi ↗ · pubmed ↗
- 5Laurenzi C. A. Gordon S. Abrahams N. du Toit S. Bradshaw M. Brand A. . (2020). Psychosocial interventions targeting mental health in pregnant adolescents and adolescent parents: a systematic review. Reprod. Health 17:65. doi: 10.1186/s 12978-020-00913-y, 32410710 PMC 7227359 · doi ↗ · pubmed ↗
- 6Li S. Liu S. Zhang P. . (2022). Suicidal ideation in the general population in China after the COVID-19 pandemic was initially controlled. J. Affect. Disord. 323, 834–840. doi: 10.1016/j.jad.2022.12.03636529410 PMC 9754752 · doi ↗ · pubmed ↗
- 7Liu S. J. Yen W. J. Chang Y. Z. Ku M. S. (2023). Impact of educational videos on maternal anxiety caused by children's heart surgery. Nurs. Crit. Care 28, 1106–1114. doi: 10.1111/nicc.12786, 35686512 · doi ↗ · pubmed ↗
- 8Lu M. Y. Ahorsu D. K. Kukreti S. Strong C. Lin Y. H. Kuo Y. J. . (2021). The prevalence of post-traumatic stress disorder symptoms, sleep problems, and psychological distress among COVID-19 frontline healthcare Workers in Taiwan. Front. Psych. 12:705657. doi: 10.3389/fpsyt.2021.705657, 34322044 PMC 8312888 · doi ↗ · pubmed ↗