APOE genotypes are associated with the level of naturally occurring antibodies to amyloid-β in patients with Alzheimer’s disease
Janardan P. Pandey, Aryan M. Namboodiri, Franca Rosa Guerini, Elisabetta Bolognesi, Milena Zanzottera, Roberta Mancuso, Simone Agostini

TL;DR
People with a specific APOE gene variant have higher levels of antibodies to a protein linked to Alzheimer's disease.
Contribution
This study is the first to show a link between APOEε4 and naturally occurring anti-amyloid-beta antibodies in Alzheimer's patients.
Findings
APOEε4 carriers had significantly higher anti-Aβ antibody levels than non-carriers.
Regression analysis showed a marginal association between APOEε4 and anti-Aβ antibodies after adjusting for other factors.
Abstract
Apolipoprotein E ε4 (APOEε4) allele is the strongest known genetic risk factor for Alzheimer’s disease (AD). Mechanisms underlying this association are incompletely understood. We aimed to determine whether APOE genotypes influenced the level of naturally occurring antibodies to amyloid-β (Aβ), a hallmark of AD, and whether anti-Aβ antibodies contributed to neurodegeneration, as measured by mini-mental state examination (MMSE) score. The study population consisted of 93 Italian AD patients. Results showed that APOEε4-carriers had significantly higher levels of anti-Aβ antibodies than non-carriers (p = 0.018). After adjusting for age, sex, Aβ levels in serum, and the MMSE scores, regression analyses showed marginal association between APOEε4 carrier status and the levels of anti-Aβ antibodies (p = 0.050). This is the first report of its kind and needs to be confirmed in a large…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
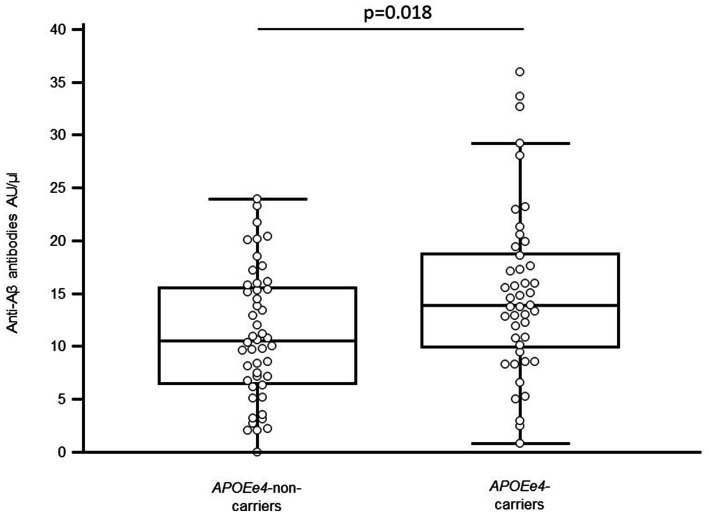 Figure 1
Figure 1| Parameters | ||||
|---|---|---|---|---|
|
| 48 | 45 | --- | |
| Gender (M: F) | 16:32 | 19:26 | ||
| Age (years, mean ± SD) | 77.28 ± 6.78 | 75.87 ± 5.68 | ||
| MMSE (adj, median and IQR) | 20; 19.00–21.35 | 19; 18.33–22.12 | ||
| Educational level (years, mean ± SD) | 8.05 ± 2.75 | 8.31 ± 3.93 | ||
| 2/2 | 1 (2.1) | 0 (0.0) | --- | |
| 2/3 | 4 (8.3) | 0 (0.0) | ||
| 2/4 | 0 (0.0) | 1 (2.2) | ||
| 3/3 | 43 (89.6) | 0 (0.0) | ||
| 3/4 | 0 (0.0) | 38 (84.4) | ||
| 4/4 | 0 (0.0) | 6 (13.3) | ||
| Serum Aβ1-42 oligomer (pg/mL, median and IQR) | 0.01 (0.01–0.01) | 0.01 (0.01–1.55) | ||
| Serum anti-Aβ antibodies (AU/μL, median and IQR) | 10.52 (6.52–15.57) | 14.25 (9.82–19.00) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAlzheimer's disease research and treatments · Dementia and Cognitive Impairment Research · Parkinson's Disease Mechanisms and Treatments
Introduction
The apolipoprotein E (APOE) gene, located on chromosome 19q33, is characterized by the segregation of three alleles—ε2, ε3, and ε4. APOEε4 increases the risk of developing late-onset Alzheimer’s disease (AD), while APOEε2 is protective, compared to the most common APOEe3 allele. One mechanism through which APOEε4 increases the risk of AD is by promoting aggregation and deposition of amyloid-β (Aβ), a hallmark of AD (Jackson et al., 2024). AD patients generate anti-Aβ autoantibodies, which have been shown to contribute to the reduction of Aβ plaque burden (Kellner et al., 2009). There are significant interindividual differences in the level of naturally occurring anti-Aβ autoantibodies, but no host genetic factors that might contribute to these differences have been identified. Identification and understanding of the host factors that influence naturally occurring immune responses to Aβ is an important prerequisite to successfully designing Aβ-based immunotherapeutic approaches against AD. Although monoclonal anti-Aβ antibodies approved for AD therapy have shown evidence of slowed clinical decline, they are associated with serious side effects, underscoring the need for a better understanding of the immunobiology of Aβ, which could lead to more efficacious alternative therapies (Jucker and Walker, 2023).
The aim of the present investigation was to determine whether the APOE genotypes influenced the level of naturally occurring antibodies to Aβ in AD patients, and whether anti-Aβ antibodies contributed to neurodegeneration, as measured by mini-mental state examination (MMSE) score.
Materials and methods
Patients
In total, DNA and sera were available from 93 AD patients, recruited by the Rehabilitative Neurology Unit of the IRCCS Fondazione Don Carlo Gnocchi, Milan, Italy. Patients were diagnosed as probable AD according to the NINCDS-ADRDA criteria (Mckhann et al., 2011). Patients were excluded if they suffered from malnutrition or vitamin deficiency syndromes, and recent introduction or dose modification of the following pharmacological treatments: cholinesterase inhibitor, memantine, antidepressant or antipsychotic drugs. Demographic and clinical data of the enrolled patients are presented in Table 1.
APOE genotyping
APOE genotyping for the three major isoforms (ε2, ε3, and ε4) was done by RT-PCR, using pre-designed TaqMan™ probes (Thermo Fisher Scientific, Waltham, MA, USA)—C_904973 (rs7412) and C_3084793 (rs429358).
Measurement of Aβ1-42
Aβ_1-42_ was measured in serum of all the enrolled subjects by using a commercial enzyme-linked immunosorbent assay (ELISA), according to the manufacturer’s instructions (cat. JP27719, IBL International, Hamburg, German). Briefly, 100 μL of serum samples diluted (1:50) with sample diluent were transferred into the pre-coated microwells and the plates were incubated overnight at 4 °C. After washing steps with washing buffer, 100 μL of labeled antibody were added to each well and incubated for 60 min at 4 °C. After re-washing step, 100 μL of chromogen solution were added to each well and incubated at room temperature for 30 min. Finally, 100 μL of stop solution were added to each well and the reaction stopped. The wells were read on a plate reader (Sunrise, Tecan, Mannedorf, Switzerland) and optical densities (OD) of wells were determined at 450 nm. Aβ_1-42_ concentration was expressed as pg/mL (sensitivity: 0.29 pg/mL).
Measurement of anti-Aβ antibodies
Antibodies to Aβ_1-42_ oligomer were also measured by ELISA, using sera from AD patients. Aβ antigen was purchased from StressMarq Biosciences (Victoria, British Columbia). Ninety-six well microtiter plates were coated with Aβ antigen, 1 μg/mL in 100 μL phosphate-buffered saline (PBS), pH 7.4 overnight at 4 °C. Plates were washed with PBS containing 0.05% tween 20 (PBS-T) and blocked with PBS-T containing 5% bovine serum albumin (BSA) for 1 h at 37 °C. Plates were then washed and incubated with suitably diluted patient plasma (1:200) in duplicate wells. Plates were further washed and incubated with antihuman IgG HRP conjugate for 30 min. Finally, plates were washed and incubated with HRP substrate hydrogen peroxide along with 3,3′,5,5′-Tetramethylbenzidine as chromogenic substrate in citrate phosphate buffer (pH 5.5). Reaction was stopped after 20 min by the addition of 100 μL of 2 N HCl and the absorbance values at 450 nm were monitored in a BioTek ELISA reader. Wells containing plasma diluent buffer alone were used as blank. Absorbance values of blank wells were subtracted from the sample wells. Antibodies to Aβ were expressed as arbitrary units per microliter (AU/μL), after multiplying with the dilution factor.
Statistical analyses
Statistical analyses were performed using the commercial MedCalc Statistical Software package (Version 11.5.0.0; Ostend, Belgium) and R. Due to relatively small sample size, genotypes were binarized based on the presence/absence of APOEε4. Age and educational level were normally distributed and they were summarized as mean ± standard deviation. The student’s t-test was used to compare these data between the carriers and non-carriers of APOEε4 allele. MMSE, Aβ_1-42_ oligomer and anti-Aβ antibody levels were not normally distributed, and they were summarized as median and interquartile range (IQR: 25_th_-75_th_ percentile). The Mann–Whitney test was used to compare MMSE, Aβ_1-42_ oligomer and anti-Aβ antibody levels between the carriers and non-carriers of APOEε4 allele. The statistical power of the study was estimated for comparing the two independent groups using a two-sided t-test. Fisher’s exact test was used to compare gender between the carriers and non-carriers of APOEε4 allele. A general linear regression model was applied to correlate anti-Aβ antibody levels and APOEε4 carrier status, adjusting for age, sex, serum amyloid beta levels, and the MMSE scores. Spearman’s correlation coefficient was used determine the association between MMSE scores and anti-Aβ antibody levels. For all analyses, p < 0.05 was considered statistically significant.
Results
APOE genotypes and the level of anti-aβ antibodies
The MMSE score of the 93 AD patients enrolled in the study (35 males and 58 females, age: 76.71 ± 6.30 years) was 18.99 ± 3.79 (educational level: 8.16 ± 3.36 years). The median value of Aβ1-42 oligomer was 0.01 (0.01–1.07) pg/mL.
Among the 93 AD subjects enrolled in the study, there were 45 (48%) APOEε4-carriers, defined by the presence of at least one ε4 allele—either in the heterozygous state (ε2/ε4: 1; ε3/ε4: 38) or homozygous state (ε4/ε4: 6). The remaining 48 subjects (52%) were non-carriers (ε2/ε2: 1; ε2/ε3: 4; ε3/ε3: 43). These results are summarized in Table 1. As shown in Figure 1, APOEe4-carriers had significantly higher ELISA reactivity to Aβ_1-42_ oligomer (14.25 AU/μL; 9.82–19.00) than non-carriers (10.52 AU/μL; 6.52–15.57; Mann–Whitney test, p = 0.018), with a statistical power of 78%. After adjusting for age, sex, Aβ levels in serum, and the MMSE scores, regression analyses showed marginally significant association between APOEε4 carrier status and levels of anti-Aβ antibodies (p = 0.050, R^2^ = 0.15). These results should be interpreted cautiously.
APOEε4-non-carriers among AD patients.
MMSE scores, anti-aβ levels, and APOE genotypes
MMSE scores were not associated with the levels of naturally occurring anti-Aβ antibodies (Spearman’s correlation test, p = 0.127; 95% confidence interval: −0.132–0.781; correlation coefficient: 0.428), or with the APOEε4 carrier status (Mann–Whitney test, p = 0.846; APOEε4-carriers: median MMSE score: 19; APOEε4-non-carriers: median MMSE score: 20). These results are summarized in Table 1. No correlation was found between anti-Aβ antibodies and Aβ_1-42_ oligomer (Spearman’s correlation test, p = 0.100; 95% confidence interval: −0.0347–0.374; correlation coefficient: 0.177).
Discussion
The results presented here show a distinct association between the presence of APOEε4 allele and higher levels of naturally occurring anti-Aβ antibodies. There are at least two possible explanations for the observed associations. The APOEε4 allele could itself somehow affect anti-Aβ antibody responsiveness. Alternatively, linkage disequilibrium between the APOEε4 allele and an allele of another as-yet-unidentified immune response gene on chromosome 19 may give rise to the associations observed.
To our knowledge, no studies have reported the influence of APOE genotypes on the level of naturally occurring anti-Aβ antibodies. However, APOEε4 allele has been shown to be associated with increased APOE expression (Griswold et al., 2021), which is positively associated with anti-Aβ antibody titer in patients immunized with Aβ_1-42_ (van Olst et al., 2025). Thus_,_ it follows that the APOEε4 allele could influence the level of naturally occurring anti-Aβ antibodies observed in this investigation—assuming immunological mechanisms underpinning the generation of naturally occurring anti-Aβ antibodies and those generated after immunization with Aβ are similar.
At first glance, the results reported here appear to be counterintuitive. Since APOEe4 is the strongest known genetic risk factor for AD, and naturally occurring anti-Aβ antibodies reduce Aβ plaque burden (Kellner et al., 2009), one would expect APOEε4 carriers to be associated with lower levels of antibodies compared to non-carriers. On the other hand, APOEε4-spurred aggregation and deposition of Aβ (Jackson et al., 2024) would increase the Aβ antigenic load, leading to the generation of higher levels of anti-Aβ antibodies.
This study has a few limitations. The cross-sectional design used in the study measures association between APOE genotypes and anti-Aβ antibodies, but does not prove causation. Since we did not have PET or CSF data, we cannot rule out that higher antibody levels reflect higher Aβ antigenic load in the brain. The anti-Aβ IgG levels were not normalized to total IgG levels. Thus, higher anti-Aβ IgG levels in the APOEε4 group could reflect the possible association of the ε4 allele with higher total IgG levels.
This is the first report documenting the involvement of APOE genotypes in humoral immunity to Aβ. Owing to significant racial/ethnic differences in the magnitude of APOEε4-related risk of AD (Jackson et al., 2024), a study involving a large multiethnic study population is needed to conclusively determine the role of the APOEε4 determinant in the generation of naturally occurring anti-Aβ antibodies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Griswold A. J. Celis K. Bussies P. L. Rajabli F. Whitehead P. L. Hamilton-Nelson K. L. . (2021). Increased APOE ε4 expression is associated with the difference in Alzheimer's disease risk from diverse ancestral backgrounds. Alzheimers Dement. 17, 1179–1188. doi: 10.1002/alz.12287, 33522086 PMC 8843031 · doi ↗ · pubmed ↗
- 2Jackson R. J. Hyman B. T. Serrano-Pozo A. (2024). Multifaceted roles of APOE in Alzheimer disease. Nat. Rev. Neurol. 20, 457–474. doi: 10.1038/s 41582-024-00988-2, 38906999 PMC 12185264 · doi ↗ · pubmed ↗
- 3Jucker M. Walker L. C. (2023). Alzheimer's disease: from immunotherapy to immunoprevention. Cell 186, 4260–4270. doi: 10.1016/j.cell.2023.08.021, 37729908 PMC 10578497 · doi ↗ · pubmed ↗
- 4Kellner A. Matschke J. Bernreuther C. Moch H. Ferrer I. Glatzel M. . (2009). Autoantibodies against β-amyloid are common in Alzheimer's disease and help control plaque burden. Ann. Neurol. 65, 24–31. doi: 10.1002/ana.2147519194878 · doi ↗ · pubmed ↗
- 5Mc Khann G. M. Knopman D. S. Chertkow H. Hyman B. T. Jack C. R.Jr. Kawas C. H. . (2011). The diagnosis of dementia due to Alzheimer’s disease: reccomendations from the National Institute on Aging-Alzheimer’s association workgroup on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7, 263–269. doi: 10.1016/j.jalz.2011.03.00521514250 PMC 3312024 · doi ↗ · pubmed ↗
- 6van Olst L. Simonton B. Edwards A. J. Forsyth A. V. Boles J. Jamshidi P. . (2025). Microglial mechanisms drive amyloid-β clearance in immunized patients with Alzheimer's disease. Nat. Med. 31, 1604–1616. doi: 10.1038/s 41591-025-03574-1, 40050704 PMC 12092304 · doi ↗ · pubmed ↗