Hydroxychloroquine therapy for women with both recurrent pregnancy loss and autoimmune disease: association with pregnancy outcomes and maternal-fetal complications
Mengyang Du, Ruixiu Zhang, Yu Na, Liying Peng, Shihua Bao

TL;DR
This study examines whether hydroxychloroquine improves pregnancy outcomes in women with a history of miscarriage and autoimmune disease, finding no significant benefit but a possible trend toward reduced preterm births.
Contribution
The study provides new insights into HCQ's potential role in preventing preterm birth in high-risk pregnancies, though without statistical significance.
Findings
Hydroxychloroquine use was not significantly associated with improved pregnancy outcomes or fewer maternal-fetal complications.
A potential protective trend against preterm birth was observed but did not reach statistical significance.
Subgroup analyses by autoimmune diagnosis showed no significant differences in outcomes.
Abstract
To evaluate the impact of hydroxychloroquine (HCQ) on pregnancy outcomes and maternal and fetal complications in women with a history of recurrent pregnancy loss (RPL) and autoimmune disease. The medical records of pregnant women with a history of RPL and autoimmune disease attending the Shanghai First Maternity and Infant Hospital between January 2017 and December 2019 were retrospectively reviewed. Primary outcomes were gestational week at delivery (term: ≥ 37 weeks; preterm: < 37 weeks). Secondary outcomes were mid-to-late pregnancy loss and maternal and fetal complications, defined in accordance with national and international guidelines. 103 (20.9%) patients were exposed to HCQ (0.1g twice daily), 389 (79.1%) were not. There were 436 full-term births, 48 preterm births, 5 late-term miscarriages, 2 stillbirths, and 1 fetal malformation-induced abortion. Univariable/multivariable…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
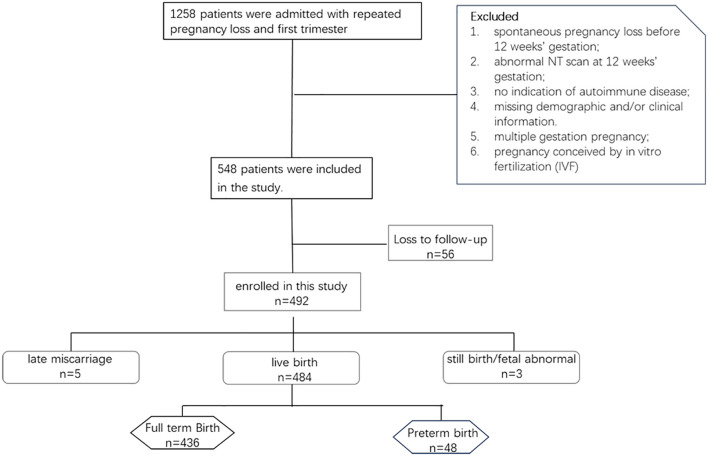 Figure 1
Figure 1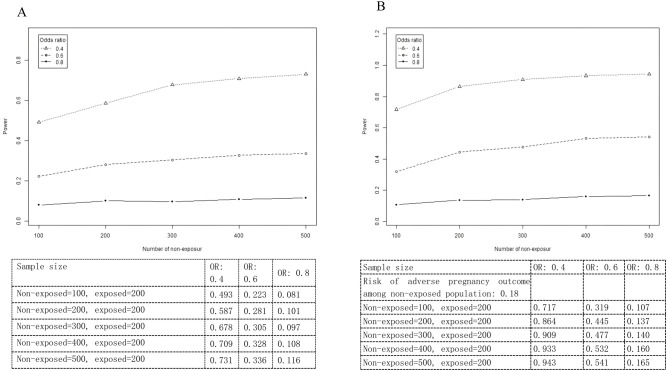 Figure 2
Figure 2| Characteristic | HCQ non-exposure | HCQ exposure | |
|---|---|---|---|
| N | 389 | 103 | |
| Age, mean ± SD (years) | 30.45 ± 3.65 | 31.13 ± 3.71 | 0.097 |
| BMI, mean ± SD (kg/m2) | 21.49 ± 2.66 | 21.80 ± 2.70 | 0.301 |
| History of recurrent spontaneous abortion, n (%) | 0.881 | ||
| No | 62 (15.94%) | 17 (16.50%) | |
| Yes | 327 (84.06%) | 86 (83.50%) | |
| History of recurrent implantation failure, n (%) | 0.497 | ||
| No | 345 (88.69%) | 89 (86.41%) | |
| Yes | 44 (11.31%) | 14 (13.59%) | |
| Previous miscarriages, n (%) | 0.216 | ||
| 2 | 190 (48.84%) | 41 (39.81%) | |
| 3 | 155 (39.85%) | 46 (44.66%) | |
| >3 | 44 (11.31%) | 16 (15.53%) | |
| Previous implantation failures, n (%) |
| ||
| 2 | 359 (92.29%) | 92 (89.32%) | |
| 3 | 14 (3.60%) | 1 (0.97%) | |
| >3 | 16 (4.11%) | 10 (9.71%) | |
| Antiphospholipid antibody positive (anticardiolipin antibody, anti-β2-glycoprotein I antibody, lupus anticoagulant), n (%) | 0.091 | ||
| No | 164 (42.16%) | 53 (51.46%) | |
| Yes | 225 (57.84%) | 50 (48.54%) | |
| Undifferentiated connective tissue disease, n (%) | 0.440 | ||
| No | 233 (59.90%) | 66 (64.08%) | |
| Yes | 156 (40.10%) | 37 (35.92%) | |
| Sjögren's syndrome, n (%) |
| ||
| No | 384 (98.71%) | 98 (95.15%) | |
| Yes | 5 (1.29%) | 5 (4.85%) | |
| Serological testing, mean ± SD | |||
| Homocysteine (µmol/l) | 8.23 ± 3.66 | 8.18 ± 1.98 | 0.902 |
| D-dimer (mg/l) | 0.30 ± 1.25 | 0.27 ± 0.26 | 0.814 |
| Platelet aggregation test (PAGT) (%) | 66.46 ± 11.43 | 65.98 ± 11.96 | 0.715 |
| Fasting glucose (mmol/l) | 4.96 ± 0.41 | 4.93 ± 0.39 | 0.592 |
| Postprandial glucose at 2 hours (mmol/l) | 6.12 ± 1.34 | 6.36 ± 1.53 | 0.135 |
| Fasting insulin (μIU/mL) | 8.13 ± 4.39 | 7.78 ± 4.03 | 0.475 |
| Postprandial insulin at 2 hours (μIU/mL) | 56.68 ± 42.22 | 57.70 ± 45.21 | 0.836 |
| Thyroid stimulating hormone (mIU/L) | 2.18 ± 1.09 | 2.29 ± 1.49 | 0.402 |
| Free thyroxine (T4) (pmol/L) | 17.18 ± 2.81 | 16.25 ± 3.55 | 0.055 |
| Folate (ng/ml) | 16.71 ± 34.71 | 14.94 ± 5.39 | 0.617 |
| Vitamin B12 (pg/ml) | 460.98 ± 195.90 | 486.40 ± 213.86 | 0.266 |
| 25-hydroxyvitamin D (nmol/l) | 43.84 ± 20.89 | 46.68 ± 32.74 | 0.299 |
| Triglycerides (mmol/l) | 1.64 ± 2.41 | 1.21 ± 0.97 | 0.135 |
| Cholesterol (mmol/l) | 4.16 ± 1.58 | 4.23 ± 1.02 | 0.709 |
| Outcome | HCQ non-exposure | HCQ exposure | |
|---|---|---|---|
| Livebirth, n (%) | 0.554 | ||
| No | 7 (1.80%) | 1 (0.97%) | |
| Yes | 382 (98.20%) | 102 (99.03%) | |
| Preterm birth, n (%) | 0.701 | ||
| No | 351 (90.00%) | 94 (91.26%) | |
| Yes | 39 (10.00%) | 9 (8.74%) | |
| Late abortion, n (%) | 0.961 | ||
| No | 386 (98.97%) | 102 (99.03%) | |
| Yes | 4 (1.03%) | 1 (0.97%) | |
| Stillbirth, n (%) | 0.466 | ||
| No | 388 (99.49%) | 103 (100.00%) | |
| Yes | 2 (0.51%) | 0 (0.00%) | |
| Fetal abnormality, n (%) | 0.607 | ||
| No | 389 (99.74%) | 103 (100.00%) | |
| Yes | 1 (0.26%) | 0 (0.00%) |
| Characteristic | OR | 95 L | 95 H | P value |
|---|---|---|---|---|
| BMI, mean ± SD (kg/m2) | 0.98 | 0.87 | 1.1 | 0.687 |
| Age, mean ± SD (years) | 1.01 | 0.93 | 1.1 | 0.754 |
| Homocysteine (µmol/l) | 0.96 | 0.83 | 1.11 | 0.57 |
| D-dimer (mg/l) | 0.97 | 0.68 | 1.39 | 0.878 |
| Platelet aggregation test (PAGT) (%) | 1.01 | 0.98 | 1.04 | 0.434 |
| Fasting glucose (mmol/l) | 1.17 | 0.55 | 2.49 | 0.685 |
| Postprandial glucose at 2 hours (mmol/l) |
|
|
|
|
| Fasting insulin (μIU/mL) | 1.04 | 0.97 | 1.11 | 0.246 |
| Postprandial insulin at 2 hours (μIU/mL) | 1 | 0.99 | 1.01 | 0.818 |
| Vitamin B12 (pg/ml) | 1 | 1 | 1 | 0.845 |
| 25-hydroxyvitamin D (nmol/l) | 1 | 0.99 | 1.01 | 0.856 |
| Acetylsalicylic acid-Yes | 0.6 | 0.33 | 1.09 | 0.094 |
| Prednisone-Yes | 0.8 | 0.44 | 1.45 | 0.453 |
| Low molecular weight heparin(LMWH)-Yes | 0.77 | 0.43 | 1.4 | 0.399 |
| Intravenous immunoglobulin(IVIG)-Yes | 1.87 | 0.21 | 16.37 | 0.571 |
| Hydroxychloroquine (HCQ)-Yes | 0.86 | 0.4 | 1.84 | 0.701 |
| Exposure | Unadjusted | Model 1(Unmatched) | Model 2 (Unmatched) | Model 2 (PSM-matched) |
|---|---|---|---|---|
| HCQ | ||||
| No | 1.0 | 1.0 | 1.0 | 1.0 |
| Yes | 0.86 (0.40, 1.84) | 0.59 (0.19, 1.84) | 0.41 (0.11, 1.51) | 0.45 (0.12-1.71) |
| Subgroup | OR | 95 L | 95 H | P value |
|---|---|---|---|---|
| Antiphospholipid Syndrome (APS) | 0.78 | 0.28 | 2.22 | 0.64 |
| Undifferentiated Connective Tissue Disease (UCTD) | 0.52 | 0.15 | 1.81 | 0.3 |
| Sjögren's Syndrome (SS) | 1.03 | 0.12 | 8.87 | 0.98 |
| A. Incidence of preterm birth | |||
|---|---|---|---|
| Preterm birth | No | Yes | |
| HCQ | 0.852 | ||
| No | 350 (78.83%) | 39 (81.25%) | |
| Yes | 94 (21.17%) | 9 (18.75%) | |
| PRED | 0.537 | ||
| No | 180 (40.22%) | 22 (45.83%) | |
| Yes | 266 (59.78%) | 26 (54.17%) | |
| B. Interaction test | |||
| Exposure | PRED | N | Crude |
| HCQ | |||
| No | No | 185 | Ref. |
| Yes | No | 16 | 0.86 (0.40, 1.84); P = 0.701 |
| No | Yes | 204 | 0.84 (0.43, 1.63); P = 0.612 |
| Yes | Yes | 87 | 0.72 (0.29, 1.78); P = 0.479 |
| P interaction | 0.732 | ||
| Characteristic | HCQ non-exposure | HCQ exposure | |
|---|---|---|---|
| N | 365 | 96 | |
| Fetal weight, mean ± SD (g) | 3226.96 ± 500.01 | 3215.46 ± 459.21 | 0.839 |
| Apgar score, mean ± SD | 9.50 ± 0.64 | 9.35 ± 0.74 | 0.172 |
| Gestational diabetes, n (%) | 0.832 | ||
| No | 299 (84.23%) | 80 (83.33%) | |
| Yes | 56 (15.77%) | 16 (16.67%) | |
| Premature rupture of membranes, n (%) | 0.459 | ||
| No | 339 (92.88%) | 87(90.63%) | |
| Yes | 26 (7.12%) | 9 (9.37%) | |
| Pregnancy-induced hypertension, n (%) | 0.104 | ||
| No | 348 (95.34%) | 95 (98.96%) | |
| Yes | 17 (4.66%) | 1 (1.04%) | |
| Placenta previa, n (%) | 0.854 | ||
| No | 344 (94.25%) | 90 (93.75%) | |
| Yes | 21 (5.75%) | 6 (6.25%) | |
| Thyroid disease, n (%) | 0.368 | ||
| No | 285 (78.08%) | 79 (82.29%) | |
| Yes | 80 (21.92%) | 17 (17.71%) | |
| Amniotic fluid reduction, n (%) | 0.055 | ||
| No | 349 (95.62%) | 87 (90.63%) | |
| Yes | 16 (4.38%) | 9 (9.37%) | |
| Umbilical cord abnormality, n (%) | 0.332 | ||
| No | 355 (97.26%) | 95 (98.96%) | |
| Yes | 10 (2.74%) | 1 (1.04%) | |
| Fetal growth restriction/intrauterine growth restriction | 0.351 | ||
| No | 359 (98.36%) | 93 (96.88%) | |
| Yes | 6 (1.64%) | 3 (3.13%) | |
| Fetal malformation, n (%) | 0.608 | ||
| No | 364 (99.73%) | 96 (100.00%) | |
| Yes | 1 (0.27%) | 0 (0.00%) | |
| Placental complications, n (%) | 0.917 | ||
| No | 358 (98.08%) | 94 (97.92%) | |
| Yes | 7 (1.92%) | 2 (2.08%) | |
| Fetal distress, n (%) | 0.200 | ||
| No | 341 (93.42%) | 93 (96.88%) | |
| Yes | 24 (6.58%) | 3 (3.12%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and Medication Impact · Reproductive System and Pregnancy · Systemic Lupus Erythematosus Research
Introduction
Recurrent pregnancy loss (RPL), defined as the occurrence of ≥ 2 miscarriages, affects an estimated 2% of fertile couples worldwide (1). The etiology of RPL is multifactorial and may be unexplained in approximately 75% of patients (2). Autoimmune factors may contribute to an estimated 20% of RPL cases (3), with autoimmune diseases such as antiphospholipid syndrome (APS), Sjogren’s syndrome (SS), and undifferentiated connective tissue disease (UCTD) being associated with RPL (4–7). These diseases generate autoantibodies that cause coagulation and immune dysfunction, ultimately resulting in pregnancy failure.
An optimal treatment strategy for managing RPL in women with autoimmune disease has yet to be established (4, 8, 9). Currently, anticoagulants (e.g., low molecular weight heparin [LMWH] or unfractionated heparin [UFH]), nonsteroidal anti-inflammatory drugs (e.g. aspirin), immunotherapies (e.g., prednisone, cyclosporine-A), hydroxychloroquine (HCQ), and supplements (e.g., folic acid, calcium, Vitamin D) may be used to manage pregnant women with autoimmune disease (10, 11). These therapies are used to treat maternal disease and may prevent pregnancy losses (12).
Hydroxychloroquine (HCQ) is an antimalarial medication widely used in the treatment of systemic lupus erythematosus (SLE), and other rheumatic disorders, and beyond its approved indications in other autoimmune diseases such as SS (13). HCQ exerts an immunosuppressive effect through the inhibition of antigen presentation and Toll-like receptor activity, reduces thrombosis, and alleviates inflammatory reactions (13, 14). During pregnancy, HCQ is effective for mitigating the activity of autoimmune disease, while the immunomodulatory, anti-thrombotic, vascular-protective and anti-infectious properties of HCQ may protect against RPL (15). Evidence suggests that HCQ can improve pregnancy outcomes in patients with refractory obstetric APS and can reduce placental inflammation and improve trophoblast function, thereby decreasing placental insufficiency and enhancing maternal-fetal health in high-risk pregnancies (16–18).
Since HCQ is widely used for autoimmune diseases in women of childbearing age, including during pregnancy, and can cross the placental barrier with similar concentrations in umbilical blood and maternal blood, concerns have been raised about potential teratogenic effects of HCQ on the fetus and the risk of adverse pregnancy outcomes (19). Although most studies have shown that HCQ is safe in pregnant women with autoimmune diseases, conclusions can vary (20, 21). Recently, a population-based cohort study of HCQ-exposed or non-exposed pregnancies in the United States reported an increased risk for major congenital malformations associated with first-trimester HCQ use (22). In contrast, a population-based cohort study of all singleton births (2006–2021) among individuals with prevalent SLE or rheumatoid arthritis (RA) in Sweden reported no teratogenic effects of HCQ exposure during the 3 months preceding pregnancy and the first trimester (23).
As most previous studies were underpowered or focused solely on APS (20, 21, 24), there remains an unmet need for more research to fully understand the impact that HCQ may have on pregnancy outcomes among women with autoimmune diseases. In particular, studies reporting the effects of HCQ on fetal development and pregnancy outcomes in patients with RPL and various autoimmune diseases in China are limited, and there are a lack of analyses clarifying the safety of HCQ by type of autoimmune disease. The objective of this study was to evaluate the impact of HCQ on mid-late pregnancy outcomes and maternal and fetal complications in patients with a history of RPL and autoimmune disease in Shanghai.
Methods
Study population
Pregnant women with a history of RPL and autoimmune disease attending the Shanghai First Maternity and Infant Hospital between January 2017 and December 2019 were eligible for this retrospective single-center cohort study.
Inclusion criteria were: 1) singleton pregnancy (spontaneous conception); 2) normal nuchal translucency (NT) scan at 12 weeks’ gestation; 3) history of RPL (≥2 consecutive spontaneous miscarriages); and 4) autoimmune disease (APS, UCTD, SS) diagnosed according to international criteria (e.g., APS: Sydney criteria 2006; SS: ACR/EULAR criteria 2016) combining clinical symptoms and serological biomarkers (e.g., antiphospholipid antibodies, antinuclear antibodies).
Exclusion criteria were: 1) spontaneous pregnancy loss before 12 weeks’ gestation; 2) abnormal NT scan at 12 weeks’ gestation; 3) no indication of autoimmune disease; 4) missing demographic and/or clinical information; 5) multiple gestation pregnancy; or 6) pregnancy conceived by in vitro fertilization (IVF).
Data collection
Medical records of included patients were reviewed, and relevant data were collected. Baseline demographic and clinical characteristics included age, pre-pregnancy body mass index (BMI), pre-pregnancy serology test results, history of and number of prior miscarriages, history of and number of previous IVF failures, and type of autoimmune disease. Pregnancy outcomes included pregnancy loss in mid-to-late pregnancy, gestational age at delivery, birth weight, and Apgar score. Maternal and fetal complications were recorded for singleton pregnancies. Medication utilization during pregnancy included HCQ use, determined from prescription records indicating HCQ dispensing at any point during gestation, and use of other immunosuppressive agents (prednisone, cyclosporin A), replacement therapy (intravenous immunoglobulin [IVIG]), anticoagulants (LMWH), anti-inflammatory agents (acetylsalicylic acid [ASA; aspirin]), supplements (folic acid, Vitamin E, calcium), and other agents (human chorionic gonadotropin).
This study did not specifically collect data on maternal adverse events potentially related to HCQ (e.g., gastrointestinal symptoms, skin reactions, ophthalmic abnormalities); such information was only recorded incidentally in electronic medical records (e.g., patient complaints during routine prenatal visits) without systematic screening or classification.
Exposure definition
Hydroxychloroquine (HCQ) exposure was defined as any oral administration of HCQ during pregnancy, based on prescription records from the hospital’s electronic medical system and patient follow-up interviews. Detailed exposure information included: time of initiation, defined as gestational week when HCQ treatment started (recorded as the first prescription date after confirmation of pregnancy); duration of use, defined as total number of weeks of HCQ administration during pregnancy (calculated as the interval between the first and last prescription dates, adjusted for missed doses reported by patients); dose (standard prescribed dose was 0.1 g twice daily [total 0.2 g/day]), and adherence, assessed by prescription refill rates and patient self-reports, with a rate of ≥80% (actual medication days/prescribed medication days) defined as “good adherence”.
Patients who initiated HCQ before pregnancy and continued use during pregnancy were classified as HCQ-exposed, while those with no HCQ prescription records or adherence <50% were classified as HCQ non-exposed.
Outcomes
Primary outcomes were gestational week at delivery, with births at ≥ 37 weeks defined as term and births at < 37 weeks defined as preterm. Secondary outcomes included mid-to-late pregnancy loss and maternal and fetal complications, defined in accordance with national and international guidelines. Causes of mid-to-late pregnancy loss included late-term miscarriage, stillbirth, and fetal malformation. Maternal and fetal complications included gestational diabetes (diagnosed via oral glucose tolerance test with ≥1 abnormal value), premature rupture of membranes (rupture before 37 weeks of gestation), pregnancy-induced hypertension (PIH, systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg after 20 weeks of gestation), placenta previa, thyroid disease, amniotic fluid reduction (maximum vertical pocket <2 cm or amniotic fluid index <5 cm). placental complications (defined as placental structural and functional abnormalities, such as placental abruption, placental infarction, placental insufficiency, and placental adhesion/implantation), umbilical cord abnormalities, fetal growth restriction/intrauterine growth retardation (FGR/IUGR, estimated fetal weight <10th percentile for gestational age), fetal malformation, and fetal distress (abnormal fetal heart rate pattern or fetal scalp blood pH <7.20).
Statistical analysis
Statistical analyses were performed using R v 3.6.1 (R Project for Statistical Computing) with the MatchIt and tableone packages for propensity score matching (PSM) and baseline balance assessment. Normally distributed data were presented as means ± standard deviations (SDs), non-normally distributed data as medians [Q25, Q75], and categorical data as counts and percentages. Data were compared using Student’s t-tests, Kruskal-Wallis analysis of variance (ANOVA), Wilcoxon signed-rank tests, or χ² tests, as appropriate.
Univariable and multivariable logistic regression analyses were conducted to identify predictors of pregnancy outcomes. Several models (unadjusted, Model 1 [M1], Model 2 [M2]) were developed with different sets of covariables for adjustment, defined a priori based on clinical experience and a literature search. Results were reported as odds ratios (ORs) with 95% confidence intervals (CIs).
The unadjusted model only analyzed the crude association between HCQ exposure and outcomes. Model 1 was adjusted for “basic confounders”, defined as variables with established clinical relevance to pregnancy outcomes in RPL-related studies (age, BMI, recurrent spontaneous abortion, recurrent implantation failure, presence of antiphospholipid antibodies, UCTD or SS, and serological markers [homocysteine, D-dimer, platelet aggregation test (PAGT), fasting glucose, fasting insulin, folate, Vitamin B12, 25-hydroxyvitamin D, triglycerides and cholesterol (15, 25). The biochemical variables (PAGT, homocysteine, Vitamin B12) were selected based on their established relevance to the pathophysiology of RPL, the defining feature of our study cohort. Specifically, PAGT is a marker of platelet activation, which plays a critical role in thrombotic placental complications that are major contributors to RPL. Homocysteine elevation and Vitamin B12 deficiency are associated with impaired endothelial function and abnormal fetal-placental perfusion, both of which are well-documented risk factors for RPL and poor pregnancy outcomes in women with autoimmune diseases (26–29). These biochemical parameters may independently influence pregnancy outcomes (26–29). Therefore, adjusting for these variables was essential to exclude their potential confounding effects and to more accurately evaluate the independent association between HCQ use and the pregnancy outcomes of interest. Model 2 was adjusted for the same covariables and medication utilization (LMWH, IVIG, prednisone, and aspirin). These medications are commonly used in pregnant women with autoimmune diseases and may interact with HCQ or independently affect preterm birth risk (30, 31).
As a sensitivity analysis to strengthen the robustness and interpretability of our findings, the main outcome (preterm birth) and key secondary outcomes (maternal-fetal complications) were re-analyzed in a matched cohort using the same univariable and multivariable logistic regression models as the unmatched cohort. To address baseline imbalances (e.g., higher rate of >3 previous implantation failures in patients exposed to HCQ, p=0.034), 1:1 nearest-neighbor PSM was conducted with a caliper width of 0.2 SDs of the propensity score. Matching variables included age, pre-pregnancy BMI, number of previous miscarriages, autoimmune disease type (APS/UCTD/SS), antiphospholipid antibody status, and use of LMWH/prednisone. Post-matching balance was assessed via standardized differences (SD < 0.1 indicated adequate balance).
Subgroup analysis was pre-specified to explore potential heterogeneity in the effect of HCQ on pregnancy outcomes (focusing on preterm birth, the primary outcome, and key secondary outcomes including maternal-fetal complications) across different types of autoimmune disease (APS, UCTD, SS). These diseases exhibit distinct pathophysiological mechanisms (e.g., APS is characterized by antiphospholipid antibody-mediated coagulation disorders, UCTD presents with incomplete manifestations of connective tissue disease, and SS is associated with exocrine gland inflammation) and clinical management differs, which may lead to variations in patients’ response to HCQ. As these diseases are extremely common in outpatient clinics, this subgroup analysis should provide targeted references for treatment decision-making. For each subgroup (APS, UCTD, SS), the same univariable and multivariable logistic regression models (unadjusted, M1, M2) used in the overall analysis were applied to estimate the ORs and 95% CIs of the association between HCQ exposure and pregnancy outcomes. Heterogeneity across subgroups was assessed using Cochran’s Q test, with a two-sided p > 0.05 indicating no significant difference in HCQ’s effect across disease type.
Interaction analysis was performed to assess the impact of combining HCQ with prednisone on pregnancy outcomes.
A sensitivity analysis, varying sample size and statistical power, was performed to further assess the robustness of the findings.
p <.05 was considered statistically significant.
Results
Study population
Of 548 eligible patients, 56 were excluded due to loss to follow-up. Reasons included 1) lack of contact (27 cases, 48.2%): 19 cases due to relocation or transfer to other hospitals (without providing new contact information) and 8 cases due to invalid contact details or family refusal to cooperate; 2) voluntary withdrawal (15 cases, 26.8%): 9 cases due to intolerance to the frequency of serological testing and 6 cases due to concerns about privacy; 3) missing information on outcomes (14 cases, 25.0%): 10 cases of delivery at other hospitals without knowledge of outcomes and 4 cases of pregnancy termination (induced abortion or late miscarriage).
Finally, 492 patients were included in the study cohort, and relevant data were extracted from electronic medical records for subsequent analysis; of these, 103 (20.9%) patients were exposed to HCQ, and 389 (79.1%) patients were not. The prescribed treatment regimen consisted of an oral administration of 0.1 g HCQ twice daily. The study flow chart of patient selection is shown in Figure 1.
Study cohort.
Patient baseline demographic and clinical characteristics stratified by HCQ exposure are presented in Table 1. HCQ-exposed patients had a significantly higher number of > 3 previous implantation failures and were significantly more likely to have positive serology for SS vs. HCQ non-exposed patients. There were no significant differences in other demographic or clinical characteristics between HCQ-exposed vs. non-exposed patients.
Pregnancy outcomes
Pregnancy outcomes stratified by HCQ exposure are presented in Table 2. There were 436 full-term births, 48 preterm births (28-36^+6^weeks), 5 late-term miscarriages (12-27^+6^weeks), 2 stillbirths (≥20 weeks), and 1 case of induced abortion due to fetal malformation. There were no significant differences in pregnancy outcomes between HCQ-exposed vs non-exposed patients.
As there are few studies on the relationship between HCQ exposure and preterm birth, and preterm birth is a major concern for obstetricians, the effect of HCQ on preterm birth was investigated. Univariable analysis of patients baseline demographic and clinical characteristics showed an association between postprandial glucose at 2 hours and preterm birth (OR 0.76 [95% CI 0.58, 0.99], p = 0.04), but no associations between patient age, pre-pregnancy BMI, other pre-pregnancy serology test results or medication utilization (Table 3).
Univariable and multivariable analyses showed a potential trend toward a protective effect of HCQ exposure on preterm birth, but no significant association (unadjusted multivariable model: OR 0.86 [95% CI 0.40, 1.84], p = 0.70; M1: OR 0.59 [95% CI 0.19, 1.84], p = 0.37; M2: OR 0.41 [95% CI 0.11, 1.51], p = 0.18) (Table 4A).The wide confidence intervals in the adjusted models reflect the limited statistical power to confirm this trend.
HCQ and prednisone are commonly used in patients with autoimmune disease; therefore, the effectof HCQ plus prednisone on preterm birth was investigated. Univariable and multivariable analyses showed no significant differences in the incidence of preterm birth between prednisone-exposed (n=26 [54.17%]) vs. non-exposed (n=22 [43.85%]) patients (p = 0.537), and no significant associations between prednisone exposure (OR 0.84 [95%CI 0.43, 1.63], p = 0.612) or HCQ plus prednisone exposure (OR 0.72 [95% CI 0.29, 1.78], p = 0.479) and preterm birth (Table 5). Interaction analysis was performed to assess the impact of combining HCQ with prednisone on pregnancy outcomes. The p-value of the interaction analysis was 0.732, indicating that the analysis was underpowered (small sample size of combined medication users) and the results are not conclusive and should be interpreted with caution.
Subgroup analysis stratified by major autoimmune diagnosis (APS, UCTD, SS), showed no significanteffect of HCQ on pregnancy outcomes between patients with APS (n=124) or UCTD (n=193) (p heterogeneity = 0.82). Due to the extremely small sample size (n=10) and only one preterm birth in patients with SS, statistical power was insufficient to determine the role of HCQ in patients with SS. No conclusions regarding the effect of HCQ in patients with SS can be drawn from this subgroup, and the results of this subgroup were not included in the overall heterogeneity assessment (Table 4B).
Maternal and fetal complications
Fetal weight and maternal and fetal complications stratified by HCQ exposure are presented inTable 6. There were no significant differences in fetal weight or the incidence of maternal and fetal complications between HCQ-exposed vs non-exposed patients.
Sensitivity analysis: propensity score-matched cohort
To address baseline imbalances (e.g., higher rate of >3 previous implantation failures and SS seropositivity in HCQ-exposed patients), 1:1 PSM was performed. Post-matching baseline characteristics of HCQ-exposed and non-exposed patients are presented in Supplementary Table S1. After matching, all variables showed standardized differences < 0.1, indicating adequate balance between the two patient groups. Specifically, the difference in the rate of >3 previous implantation failures (from 0.21 pre-matching to 0.07 post-matching) and SS seropositivity (from 0.15 pre-matching to 0.08 post-matching) were eliminated. Demographic characteristics, autoimmune disease distribution, serological markers, and medication use were also well-balanced, ensuring that the sensitivity analysis of pregnancy outcomes and maternal and fetal complications were not confounded by differences at baseline.
After 1:1 PSM, 206 patients (103 HCQ-exposed vs. 103 non-exposed) were included in the sensitivity analysis. Consistent with the unmatched cohort, multivariable logistic regression in the matched cohort showed no statistically significant association between HCQ exposure and preterm birth (OR 0.52 [95% CI 0.16, 1.68], p=0.27; Model 2 adjusted for medications: OR 0.45 [95% CI 0.12, 1.71], p=0.24), retaining the potential protective trend observed in the main analysis.
For secondary outcomes, no significant differences were found in fetal weight (3208.7 ± 462.3 g vs. 3231.2 ± 498.5 g, p=0.81) or maternal-fetal complication rates (e.g., gestational diabetes: 8.7% vs. 10.7%, p=0.68; pregnancy-induced hypertension: 1.0% vs. 3.9%, p=0.32) between HCQ-exposed vs non-exposed patients in the matched cohort. These results confirm that the primary findings were not confounded by baseline imbalances, supporting the robustness of the study conclusions (Table 4A, Supplementary Table S1).
Sensitivity analysis: sample size and statistical power
Sensitivity analysis was also conducted to explore the effect of power and sample size on study results. Findings showed that even when the sample size of non-exposed patients increased, the association between HCQ exposure and adverse pregnancy outcomes did not reach significance, suggesting the results of this study are robust (Figure 2). Combined with the consistent results from the PSM-matched cohort analysis, these findings further confirm the robustness of the study conclusions.
Sensitivity analysis. (A) Risk of adverse pregnancy outcomes among the non-exposed population: 0.1. (B) Risk of adverse pregnancy outcomes among the non-exposed population: 0.18.
Discussion
This study explored the effects of HCQ on pregnancy outcomes in women with a history of RPL and autoimmune disease, with a particular focus on gestational age at delivery and maternal and fetal complications. Findings showed that HCQ was not associated with an increased risk of preterm birth, late abortion, stillbirth, or maternal or fetal complications (including gestational diabetes, PIH, placenta previa, placental complications, FGR/IUGR, fetal malformation and fetal distress). A potential protective trend against preterm birth was observed, but this association did not reach statistical significance. These results support the safety of HCQ in this high-risk population, while the observed protective trend requires confirmation in larger studies.
To the authors’ knowledge, this is the first study to focus on the effects of HCQ on pregnancy outcomes in women with a history of RPL and various autoimmune diseases, including in China. Most previous studies have focused on the effects of HCQ in patients with APS, a leading cause of RPL (25), and some have characterized pregnancy complications and treatment in obstetric APS in China (32, 33).
Consistent with the multivariable analysis results (Model 2 OR 0.41, p=0.18), the potential protective trend of HCQ on preterm birth may be related to its anti-inflammatory and vascular-protective effects [inhibiting placental inflammation and improving trophoblast function (18)]. Notably, the median gestational week of HCQ initiation in our study was 12 weeks (second trimester), when placental development is already established. This timing may allow HCQ to target placental inflammation without interfering with early embryonic development, which could explain why our results differ from studies reporting teratogenic risks with first-trimester HCQ exposure. These observations need to be confirmed by larger sample studies.
Pregnancies in patients with autoimmune disease are challenging to manage due to autoimmune disease activity, the presence of some autoantibodies, pharmacological therapy, comorbidities, and the potential for adverse maternal and fetal outcomes (34). Pregnancy may increase disease activity in patients with some autoimmune diseases, and exacerbation of disease could be detrimental to both mother and fetus. While teratogenic drugs should be discontinued before conception in patients with autoimmune disease planning pregnancy, evidence suggests that it is beneficial to continue HCQ throughout gestation (34).
HCQ has dual immunomodulating and vascular protective effects. Specifically, HCQ inhibits antigen processing and presentation, subsequent T-cell activation, and the production of pro-inflammatory cytokines. It has vascular protective effects through the reduction of endothelial dysfunction and hypercoagulability, particularly through the inhibition of antiphospholipid antibody binding and platelet aggregation.
While there is consensus HCQ should be maintained throughout pregnancy in women with autoimmune disease, the safety of HCQ is still debated. Previous studies showed that first-trimester exposure to HCQ among individuals with SLE or RA was not associated with a significantly increased risk of major congenital malformations (23, 35) and there were no differences in live birth rates, preterm birth rates, or adverse pregnancy outcomes such as miscarriage, premature rupture of membranes or neonatal morbidity in women with various connective tissue diseases (36) or SLE (37, 38) exposed to vs. not exposed to HCQ during pregnancy. However, in one meta‐analysis HCQ exposure was associated with an increased rate of spontaneous abortion in women with autoimmune disease. The present study adds to this body of evidence showing that HCQ did not increase the risk of preterm birth, late abortion, stillbirth, or maternal or fetal complications in women with a history of RPL and autoimmune disease. Notably, our study focused on women with both RPL and autoimmune disease, a population at higher pregnancy risk than those with autoimmune disease alone. The safety of HCQ in this specific population further supports its clinical application.
In the context of RPL, the immunomodulatory, anti-thrombotic, vascular-protective, and anti-infectious effects of HCQ may be protective. Dysregulation of the maternal immune system is an underlying mechanism of RPL, as the balance between immune activation and tolerance within the endometrium is essential for successful pregnancy. HCQ may prevent an overactive pro-inflammatory response at the maternal–fetal interface and promote the vascular remodeling of spiral arteries essential for placentation (15). A systematic review showed HCQ in addition to aspirin and heparin had a significant benefit for mitigating the risk of antiphospholipid antibody-mediated obstetrical complications (39) (live birth rate, pregnancy loss, maternal complications, neonatal complications) in patients with APS. A double-blind placebo-controlled trial investigating the effect of HCQ on pregnancy outcomes in unexplained RPL showed the prevalence of abortion in individuals exposed to HCQ was four times lower than in individuals exposed to placebo, however, this difference was not statistically significant (40). In the present study, there was no significant difference in the number of live births in women with a history of RPL and autoimmune disease exposed to vs. not exposed to HCQ implying HCQ had limited impact on the mechanisms underlying RPL in this patient population.
While our study focused on pregnancy and fetal outcomes, it is important to acknowledge that we did not systematically assess HCQ-related maternal adverse events. Previous studies have reported mild, transient side effects of HCQ in pregnant women (e.g., gastrointestinal symptoms, skin reactions) that rarely require treatment discontinuation (35, 36). Given the lack of systematic screening in our study, we cannot rule out the possibility of underreported mild maternal adverse effects; however, no severe adverse events (e.g., retinal toxicity, severe hematological abnormalities) were incidentally recorded in medical records, which is consistent with the overall favorable safety profile of HCQ reported elsewhere (41–44).
Notably, treatment options for pregnant women with autoimmune diseases are evolving. One study showed that HCQ combined with low-dose aspirin was associated with a higher proportion of full-term pregnancies and a significantly lower proportion of hypertension, prematurity, and pregnancy loss than HCQ alone in women with SLE. A multicenter study exploring the effects of additional treatments combined with conventional therapies in pregnant patients with high-risk APS suggests that preconception HCQ therapy significantly reduces the risk of fetal death in cases previously refractory to low-dose aspirin and heparin alone, offering a promising strategy for improving pregnancy outcomes in high-risk patients with APS (45). Future studies should focus on the dosage of HCQ, its duration of use, and its safety when used in combination with other immunosuppressive medications in pregnant women with autoimmune diseases.
Limitations
Although this study provides important clinical evidence for the use of HCQ in women with a history of RPL and autoimmune diseases, it has certain limitations that should be acknowledged when interpreting the results. First, the sample size of this study was relatively small, which may affect the external validity of the results. Second, the study primarily focused on mid-to-late pregnancy outcomes and lacked observations on the effect of HCQ use during the early stages of pregnancy. Third, the effects of HCQ may differ for pregnant women with different types of autoimmune diseases, and future research should involve more detailed subgroup analyses based on specific diseases. Fifth, the timing of HCQ initiation varied considerably among participants in our cohort, which may introduce residual confounding given that the potential effects of HCQ on pregnancy outcomes could be time-dependent. Sixth, HCQ adherence was assessed based on medical record documentation and patient self-report rather than objective measures (e.g., serum drug concentration testing or electronic medication monitoring). This subjective assessment method may lead to misclassification of adherence status, which could bias the observed associations between HCQ use and study outcomes. Seventh, multiple comparisons were conducted across various pregnancy outcomes, subgroup analyses, and interaction analyses in this study. Without formal statistical correction for multiple testing, the risk of type I error may be elevated, particularly for exploratory findings. Eighth, this study did not systematically collect data on HCQ-related maternal adverse events, which is a key consideration for drug safety evaluation in long-term use. Mild or asymptomatic maternal side effects (e.g., mild nausea, transient pruritus, subclinical ophthalmic changes) may have been overlooked during routine prenatal visits, as maternal adverse event screening was not a predefined study objective. Routine ophthalmic examinations (e.g., optical coherence tomography) targeting HCQ-related retinal toxicity were not performed for all exposed patients, further increasing the risk of under detecting subclinical maternal adverse effects. Last, the single-center observational design of this study prevents the establishment of causal relationships between HCQ use and pregnancy outcomes.
These limitations highlight the need for future studies to fully evaluate the use of HCQ in pregnant women with a history of RPL and autoimmune diseases.
Conclusions
This study suggests that HCQ use in pregnant women with a history of RPL and autoimmune diseases is not associated with an increased risk of preterm birth, or maternal or fetal complications, and may offer a protective effect. HCQ appears to be safe for maternal and fetal health during pregnancy, providing positive clinical evidence for managing pregnancies in high-risk patients. Due to the small sample size and retrospective design, the potential protective effect of HCQ on preterm birth needs to be confirmed by prospective multicenter studies with larger samples. Future research should also focus on long-term neonatal safety and the role of HCQ in different types of autoimmune disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boedeker D Mahdy H . Recurrent Pregnancy Loss. In: Stat Pearls. Stat Pearls Publishing, Treasure Island (FL (2025). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK 554460/. 32119347 · pubmed ↗
- 2Turesheva A Aimagambetova G Ukybassova T Marat A Kanabekova P Kaldygulova L . Recurrent pregnancy loss etiology, risk factors, diagnosis, and management. Fresh look into a full box. J Clin Med. (2023) 12:4074. doi: 10.3390/jcm 12124074, PMID: 37373766 PMC 10298962 · doi ↗ · pubmed ↗
- 3Laijawala RA . Recurrent Pregnancy Loss: Immunological aetiologies and associations with mental health. Brain Behav Immun Health. (2024) 41:100868. doi: 10.1016/j.bbih.2024.100868, PMID: 39391794 PMC 11466561 · doi ↗ · pubmed ↗
- 4Gao R Zeng X Qin L . Systemic autoimmune diseases and recurrent pregnancy loss: research progress in diagnosis and treatment. Chin Med J (Engl). (2021) 134:2140–2. doi: 10.1097/cm 9.0000000000001691, PMID: 34432653 PMC 8439985 · doi ↗ · pubmed ↗
- 5Geng B Zhang K Huang X Chen Y . A meta-analysis of the effect of Sjögren's syndrome on adverse pregnancy outcomes. Clinics (Sao Paulo). (2022) 77:100140. doi: 10.1016/j.clinsp.2022.100140, PMID: 36403428 PMC 9678673 · doi ↗ · pubmed ↗
- 6Guo D Diao Z Wang K Pang C . Causal association between rheumatoid arthritis and pregnancy loss and intrauterine growth retardation: A bidirectional two-sample Mendelian randomization study. Med (Baltimore). (2024) 103:e 36873. doi: 10.1097/md.0000000000036873, PMID: 38215086 PMC 10783369 · doi ↗ · pubmed ↗
- 7Barilaro G Castellanos A Gomez-Ferreira I LledóGM Della Rocca C Fernandez-Blanco L . Systemic sclerosis and pregnancy outcomes: a retrospective study from a single center. Arthritis Res Ther. (2022) 24:91. doi: 10.1186/s 13075-022-02783-0, PMID: 35477585 PMC 9044598 · doi ↗ · pubmed ↗
- 8Odendaal J Quenby S Sammaritano L Macklon N Branch DW Rosenwaks Z . Immunologic and rheumatologic causes and treatment of recurrent pregnancy loss: what is the evidence? Fertil Steril. (2019) 112:1002–12. doi: 10.1016/j.fertnstert.2019.10.002, PMID: 31843070 · doi ↗ · pubmed ↗