Immunomodulators in Graves’ ophthalmopathy: a systematic review
Antoinette Yeung, Mohammed Saqlain Siddiqui, Neginsadat Mirtorabi, Umnia Nasir Ahmed, Emma Watts, Neil Sharma, Reena Kumari, Kristien Boelaert, Jameel Muzaffar, Hannah Nieto

TL;DR
This systematic review evaluates immunomodulatory drugs for treating Graves’ ophthalmopathy, comparing their effectiveness and safety.
Contribution
The study provides a comprehensive evaluation of newer immunomodulatory therapies for Graves’ ophthalmopathy.
Findings
Teprotumumab and tocilizumab reduced Clinical Activity Score and proptosis.
Rituximab's effectiveness was inconclusive.
Steroid-sparing agents may be more effective than steroids for reducing Clinical Activity Score.
Abstract
Graves’ Ophthalmopathy (GO), or thyroid eye disease, is an extrathyroidal complication of Graves’ disease, causing a significant impact on patients’ quality of life. There are consensus statements from both the American Thyroid Association (ATA) and the European Group on Graves’ Orbitopathy (EUGOGO) which provide guidance in management. However, there remain areas of ongoing debate and evolution in treatment approaches. This systematic review aims to evaluate immunomodulatory drugs in the treatment of GO. The following databases were searched: Cochrane (CENTRAL), Embase, MEDLINE, ProQuest, PubMed, SCOPUS, and Web of Science. The last date of searching for each database was 10th October 2025. All primary studies on human patients with GO, treated with newer, targeted immunomodulatory therapies, in particular biologics and/or disease-modifying antirheumatic drugs, were included. Studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
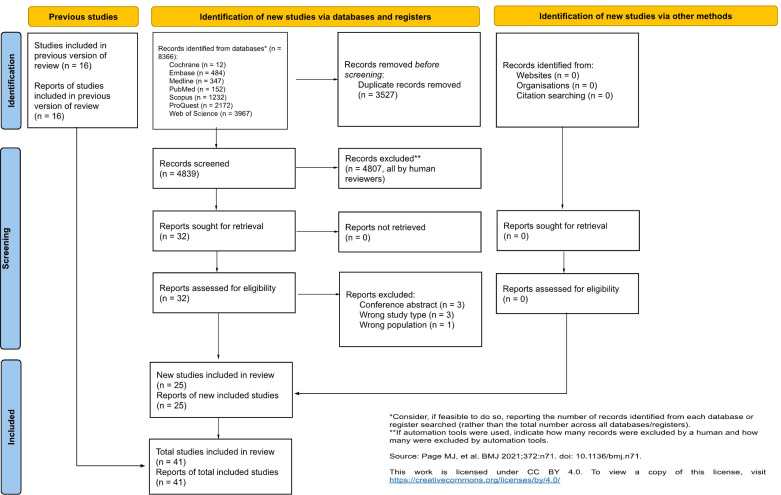 Figure 1
Figure 1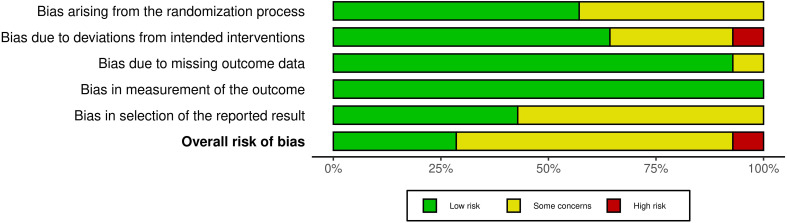 Figure 2
Figure 2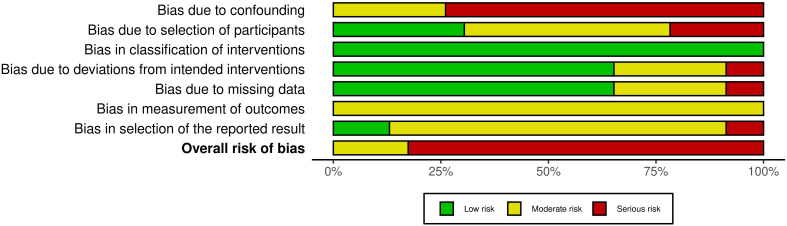 Figure 3
Figure 3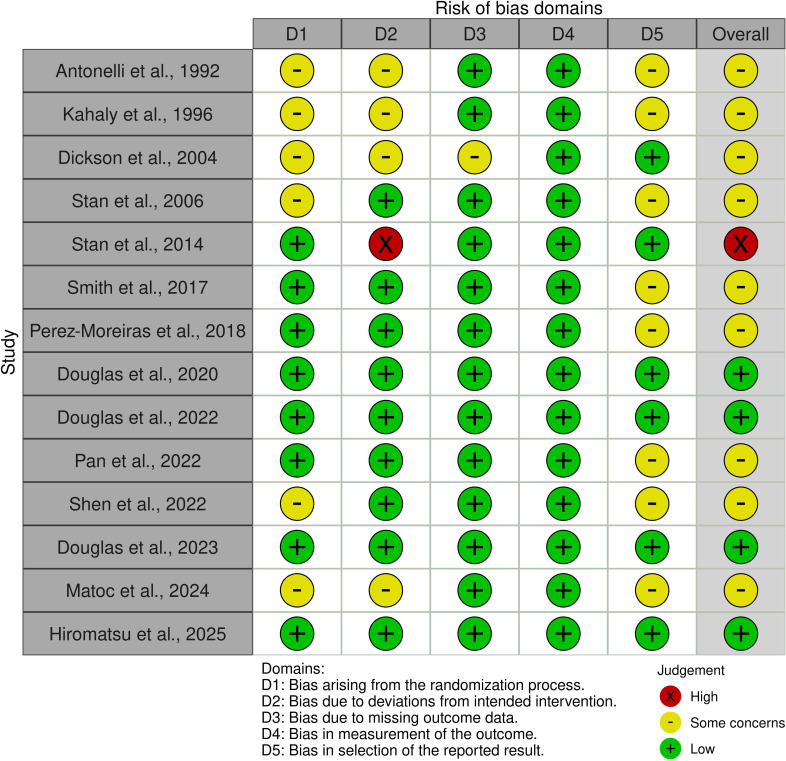 Figure 4
Figure 4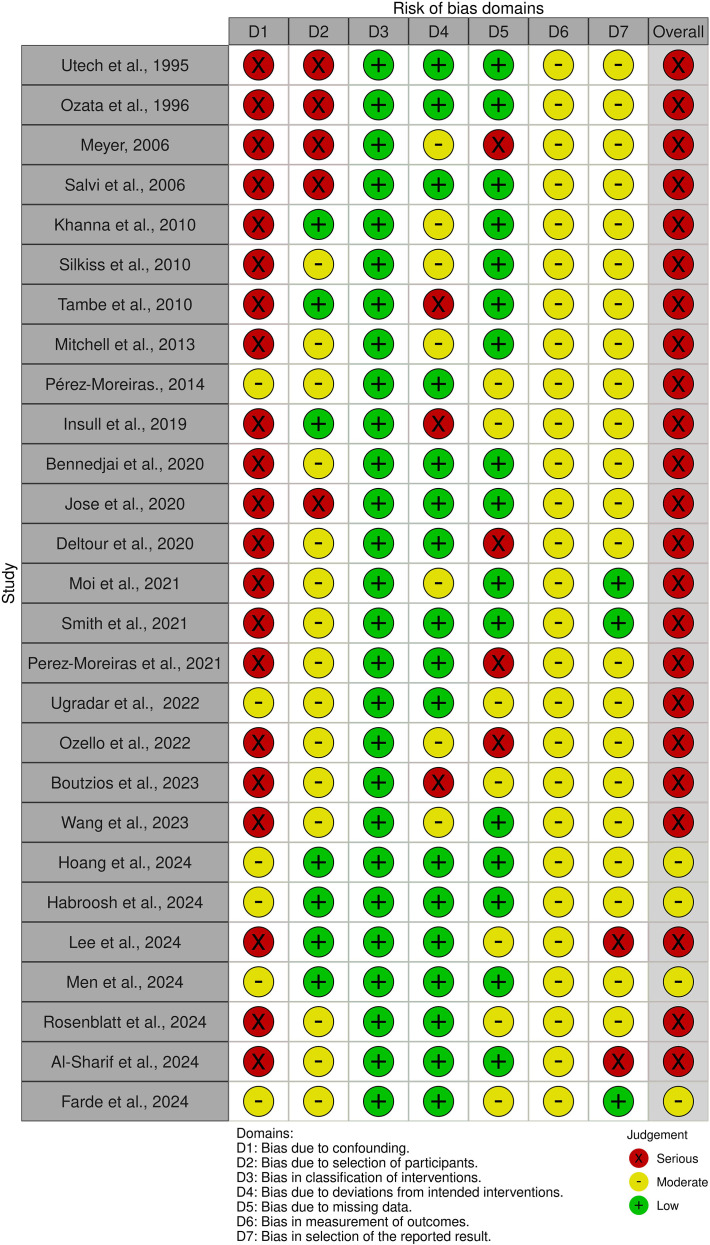 Figure 5
Figure 5| For initial CAS score items 1-7 |
|---|
| 1) Spontaneous orbital pain |
| 2) Gaze evoked orbital pain |
| 3) Eyelid swelling that is considered to be due to active GO |
| 4) Eyelid erythema |
| 5) Conjunctival redness considered due to active GO |
| 6) Chemosis |
| 7) Inflammation of caruncle or plica |
| Population | Adults (≥18 years) with GO |
| Interventions | Targeted immunomodulatory therapies (especially biologics ± DMARDS) |
| Comparator | Current treatments for GO |
| Outcomes | Primary Outcome: Clinical Activity Score |
| Study reference | Type of Study | No. of patients | Intervention | Dosage of drug(s) | Dosage time frame | Main outcome | Secondary outcome | Mean follow-up (months) |
|---|---|---|---|---|---|---|---|---|
| Antonelli et al., 1992 ( | RCT | 26 | Group 1: IVIG + OR | IVIG: 400mg/kg | 5 days repeated 3x every 3 weeks | Ophthalmopathy index | – | 6 |
| Group 2: IVIG | MP: 80mg | 2 weeks | ||||||
| Group 3: MP + OR | OR: 200cGy | 2 weeks | ||||||
| Utech et al., 1995 ( | Prospective case series | 39 | Cyclosporine | 2.5mg/kg | Mean 27 weeks | MRI T2 relaxation time | Muscle thickness IOP | 12, 36, 72 |
| Prednisolone | 60mg | 3 months | ||||||
| Kahaly et al., 1996 ( | RCT | 40 | IVIG | 1g/kg | 2 days repeated 6x every 3 weeks | Proptosis | – | 4.6 |
| Prednisolone | 100mg/day | |||||||
| Ozata et al., 1996 ( | Prospective case series | 10 | Octreotide | 100mcg | 3 months | sICAM-1 | Proptosis Ophthalmopathy index | 3 |
| Dickinson et al., 2004 ( | RCT | 50 | Octreotide Long Acting Repeatable (LAR-LAR) | 30mg every 4 weeks | 32 weeks | Ophthalmopathy Index (OI) score | CAS | 13 |
| Placebo-LAR | 0.9% sodium chloride then 30mg every 4 weeks | 16 weeks then 16 weeks | ||||||
| Meyer, 2006 ( | Retrospective case series | 14 | IVMP | 10mg/kg | 3x every 2 days | Visual acuity | AEs | 36 |
| Prednisolone | 30mg | 2 years | ||||||
| Cyclosporine | 2mg/kg | 2x for 2 days | ||||||
| Stan et al., 2006 ( | RCT | 25 | Octreotide Long Acting Repeatable (LAR) | 20mg every 4 weeks | 4 months | CAS | Retrobulbar tissue volume | 4 |
| Placebo | 0.9% saline | 4 months | ||||||
| Salvi et al., 2008 ( | Prospective cohort study | 29 | IV RTX | 2x 1g | 2 weeks apart | CAS | Thyroid function B cell count | 12 |
| IVGC | 500mg | 16 weeks | ||||||
| Khanna et al., 2010 ( | Retrospective case series | 6 | RTX | 2x 1g | 2 weeks apart | CAS | – | 6.2 |
| Silkiss et al., 2010 ( | Prospective case series | 12 | RTX | 2x 1g | 2 weeks apart | CAS | B cell count, TSI, TSH | 12 |
| Tambe et al., 2010 ( | Retrospective case series | 36 | IVMP | 1g | 3 days | Efficacy of IVMP | Proptosis | 0.92 |
| Mitchell et al., 2013 ( | Retrospective case series | 9 | RTX | 3 pts - 2x 2g | 2 weeks apart | CAS | – | 12 |
| 6 pts - 2x 1g | 2 weeks apart | |||||||
| Perez-Moreiras et al., 2014 ( | Prospective interventional non- randomised study | 18 | Tocilizumab | 8mg/kg once a month | Until CAS <1 or TSI negative | CAS | Ocular motility | 9 |
| Stan et al., 2015 ( | RCT | 21 | RTX | 2x 1g | 2 weeks apart | CAS | Proptosis | 12 |
| Placebo | 0.9% sodium chloride | |||||||
| Smith et al., 2017 ( | RCT | 88 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | CAS | QOL | 11 |
| Placebo | 0.9% sodium chloride | |||||||
| Perez-Moreiras et al., 2018 ( | RCT | 32 | Tocilizumab | 8mg/kg once a month | 4 months | CAS | QOL | 10 |
| Placebo | 0.9% sodium chloride | |||||||
| Deltour et al., 2018 ( | Retrospective cohort study | 40 | RTX | 2x 1g | 2 weeks apart | CAS | Proptosis | 6 |
| Insull et al., 2019 ( | Retrospective case series | 12 | RTX | 100mg | 1 hour | CAS | VISA | 6.3 |
| Douglas et al., 2020 ( | RCT | 83 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | Overall response (CAS + proptosis) | 6 |
| Placebo | – | |||||||
| Ceballos-Macias et al., 2020 ( | Retrospective case series | 8 | Tocilizumab | 8mg/kg once a month | 6 months | CAS | – | 6 |
| Perez-Moreiras et al., 2021 ( | Retrospective Longitudinal Study | 54 | Tocilizumab | 8mg/kg once a month | 4 months | CAS | 22 | |
| Smith et al., 2021 ( | Retrospective case series | 9 | Tocilizumab | 8mg/kg once a month | 4 months | CAS | TAOS | 24 |
| Moi et al., 2021 ( | Retrospective cohort study | 10 | Tocilizumab | 6 months: 8mg/kg once a month | 18 months | CAS | – | 6 |
| Ugradar et al., 2022 ( | Retrospective cohort study | 31 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | Diplopia | 6 |
| Ozello et al., 2022 ( | Retrospective case series | 9 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | Adverse events | 17 |
| Douglas et al., 2022 ( | RCT | 51 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | CAS | 11 |
| Bennedjai et al., 2022 ( | Comparative Retrospective Cohort Study | 21 | Tocilizumab | 8mg/kg once a month | 4 months | CAS | Proptosis | 11 |
| Rituximab | 2x 100mg | 2 weeks apart | 16 | |||||
| Pan et al., 2022 ( | RCT | 100 | Doxycycline | 50mg | 12 weeks | Eyelid aperture QOL | CAS | 2.8 |
| Placebo | Starch | 12 weeks | ||||||
| Shen et al., 2022 ( | RCT | 90 | Group 1: MP | MP=IV 0.5g/week | 6 weeks | CAS | Proptosis | 2.8 |
| Group 2: Reduced MP + MTX | Reduced MP = IV, 0.25g/week | 12 weeks | ||||||
| Group 3: full-dose MP | MTX = oral 10mg/week | 2 weeks | ||||||
| Douglas et al., 2023 ( | RCT | 62 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | GO-QOL | 6 |
| Placebo | - | |||||||
| Boutzios et al., 2023 ( | Retrospective observational study | 12 | Tocilizumab | 8mg/kg once a month | 4 months | CAS | TSI levels | 5.5 |
| Wang et al., 2023 ( | Retrospective Case Series | 6 | Rituximab | 125mg/m2 body surface area | Once per week for 4 weeks | CAS | B-cell depletion | 56 |
| Men et al., 2024 ( | Retrospective cohort study | 66 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | – | 8 |
| Hoang et al., 2024 ( | Retrospective non comparative study | 26 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | TFTs | 24 |
| Rosenblatt et al., 2024 ( | Retrospective cohort study | 119 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | CAS | 10.5 |
| Matoc et al., 2024 ( | RCT | 82 | Doxycycline | 50mg OD | 12 weeks | CAS | MRD1 and 2 | 12 |
| No treatment | – | |||||||
| Habroosh et al., 2024 ( | Prospect Longitudinal Cohort study | 13 | Tocilizumab | 8mg/kg once a month | 4 months | CAS | – | 20.5 |
| Lee et al., 2024 ( | Prospective Cohort study | 19 | Tocilizumab | 8mg/kg once a month | 4 months | CAS | TRAb | 22.8 |
| Al-Sharif et al., 2024 ( | Retrospective Cohort study | 91 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Reduction in eyelid retraction | – | 9 |
| Farde et al., 2025 ( | Retrospective Cohort study | 23 | Tocilizumab | 8mg/kg once a month | 4 Months | ≥2 mm Hertel reduction | Improvement in CAS ≥ 2 points | 10 |
| Hiromatsu et al., 2025 ( | RCT | 54 | Teprotumumab | 8 infusions: 10mg/kg then 20mg/kg | 24 weeks | Proptosis | – | 6 |
| Placebo | – | 24 weeks |
| Reference | Treatment | Mean CAS Before Treatment (SD) | Follow Up (weeks) | Mean CAS After Treatment (SD) | P-value |
|---|---|---|---|---|---|
| Dickinson et al., 2004 ( | Octreotide (LAR) | 5.39 (1.56) | 24 | 17/23d | <0.001 |
| Placebo | 5.85 (1.51) | 22/27d | |||
| Stan et al., 2006 ( | Octreotide (LAR) | 6b | 16 | 12/14d | <0.001 |
| Placebo | 5b | 4/11d | |||
| Salvi et al., 2008 ( | RTX | 4.70 (0.50) | 104 | 1.80 (0.80) | <0.0001 |
| Khanna et al., 2010 ( | RTX | 5.30 (1.0) | 8 | 1.30 (0.50) | 0.0001 |
| Silkiss et al., 2010 ( | RTX | 5.5 (1.2) | 4, 8, 16, 24, 36, 52 | 2.3-4.7a | <0.01 |
| Mitchell et al., 2013 ( | RTX | 6 (1–8) b | 12 | 2 (1-6)b | 0.018 |
| Perez-Moreiras et al., 2014 ( | Tocilizumab | 6.5 (1.29) | 54 | 0.61 (0.85) | <0.001 |
| Stan et al., 2015 ( | Rituximab | 4.9 (1) | 24, 52 | 2.0 (1.7) | 0.64 |
| Placebo | 5.1(1) | 2.9 (2.3) | |||
| Smith et al., 2017 ( | Teprotumumab | 5.1 (0.97) | 48 | -3.43a | <0.001 |
| Placebo | 5.2 (0.74) | -1.85a | |||
| Perez-Moreiras et al., 2018 ( | Tocilizumab | 5.0 | 16, 40 | 13/15e | – |
| Placebo | 5.0 | 10/17e | |||
| Deltour et al., 2018 ( | RTX | 3.29 (1.16) | 24 | 1.59 (1.12) | <0.001 |
| Insull et al., 2019 ( | RTX | 5.08 (1.98) | 27.4 | 1.58 (1.16) | <0.001 |
| Douglas et al., 2020 ( | Teprotumumab | 5.1 (0.9) | 24 | 24/41c | 0.001 |
| Placebo | 5.3 (1.0) | 9/42c | |||
| Ceballos-Macias et al., 2020 ( | Tocilizumab | 4.1 (0.3) | 24 | 1.1 (0.6) | 0.001 |
| Perez-Moreiras et al., 2021 ( | Tocilizumab | 6.7 (1.5) | 20 | 0.4 (0.7) | <0.001 |
| Smith et al., 2021 ( | Tocilizumab | 6.78 (1.09) | 104 | 0.44 (0.53) | <0.001 |
| Moi et al., 2021 ( | Tocilizumab | 4.8 (1.13) | 24 | 0.7 (0.82) | – |
| Ugradar et al., 2022 ( | Teprotumumab | 2.3 (0.9) | 24 | 0.5 (0.7) | 0.01 |
| Douglas et al., 2022 ( | Teprotumumab | 3.5 (1.6) | 24 | 4/7c | – |
| Placebo | 3.6 (1.7) | 24 | 21/32c | ||
| Bennedjai et al., 2022 ( | Tocilizumab | 5.0 (0.5) | 44 | 1.2 (0.9) | <0.05 |
| Rituximab | 4.0 (1.2) | 64 | 2.5 (1.9) | 0.07 | |
| Pan et al., 2022 ( | Doxycycline | – | 4 | 42/48c | 0.14 |
| 12 | 42/48c | ||||
| Placebo | – | 4 | 38/50c | 0.82 | |
| 12 | 43/50c | ||||
| Shen et al., 2022 ( | MP | 4.5 (3-5)b | 12 | 2 (1-4)b | 0.1 |
| Reduced MP + MTX | 4 (3-5)b | 12 | 2 (1-3)b | 0.1 | |
| MP + MTX | 4 (4-5)b | 12 | 2 (1-3)b | 0.1 | |
| Boutzios et al., 2023 ( | Tocilizumab | – | 30 | 6/6d | 0.002 |
| Wang et al., 2023 ( | Rituximab | 4.86 (0.69) | 52 | 0.86 (0.90) | 0.001 |
| Men et al., 2024 ( | Teprotumumab | 4.4 | 24 | -3.8 (1.6)a | 0.01 |
| Hoang et al., 2024 ( | Teprotumumab | 4 (2.5-5)b | 24 | 1 (0-3)b | 0.0002 |
| Rosenblatt et al., 2024 ( | Teprotumumab | 5.11 | 42 | 0.84 | 0.001 |
| Matoc et al., 2024 ( | Doxycycline | 34 (82.9) | 12 | 6 (14.6) | – |
| No treatment | 19 (46.3) | 9 (22) | |||
| Habroosh et al., 2024 ( | Tocilizumab | 7.92 (0.66) | 52 | 2.85 (1.03) | <0.0001 |
| Lee et al., 2024 ( | Tocilizumab | – | 90 | 16/19d | – |
| Farde et al., 2025 ( | Tocilizumab | 5.22 (1.53) | 40 | 2.09 (1.38) | <0.001 |
| Hiromatsu et al., 2025 ( | Teprotumumab | 4.5 (1.3) | 24 | 16/27d | 0.0031 |
| Placebo | 4.0 (0.8) | 6/27d |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Eye Disorders · Thyroid Disorders and Treatments · Vestibular and auditory disorders
Introduction
Graves’ ophthalmopathy (GO) is a potentially sight-threatening autoimmune disease, characterized by inflammation of the orbit and its surrounding tissues. It forms the most frequent extrathyroidal manifestation of Graves’ disease (1). At least 50% of patients with Graves’ disease develop clinically significant GO (2), leading to an estimated prevalence in Europe of 90–155 per 100,000 people (3). The most recent guidelines from the European Group on Graves’ Orbitopathy (EUGOGO) subcategorizes presentation as mild, moderate-to-severe, or sight-threatening disease (4). GO can be subclassified further into inactive and active phases of GO.
Typically, diagnosis relies on the presence of key clinical features on a background of confirmed Graves’ disease (5). However, thyroid stimulating hormone receptor antibodies (TRAbs) have demonstrated independent association with GO and the potential to predict disease severity and clinical outcomes (6). Currently, TRAbs are the only biomarker specific to both Graves’ disease and GO (7).
Distinguishing active and inactive GO is currently measured using the validated Clinical Activity Score (CAS), which helps direct treatment strategies (Table 1) (4, 9).
Historically, corticosteroid therapy was the mainstay of active, moderate-to-severe GO (11) and remains popular for alleviating orbital inflammation (8, 12). Other interventions include orbital radiotherapy and corticosteroid-sparing agents such as methotrexate and cyclosporine (13, 14). These are all associated with significant side effects and can be quite co-morbid, so alternative treatments are welcome.
Recent developments in our understanding of the immunological basis of GO have placed increasing focus on newer, more targeted immunomodulatory therapies such as monoclonal antibodies. In 2020, the monoclonal antibody teprotumumab became the first FDA approved drug for the treatment of GO in adult patients (15).
The EUGOGO 2021 guidelines outline clear treatment recommendations for mild disease and first-line strategies for moderate-to-severe disease (4). The evidence basis for second-line treatments in moderate-to-severe disease is less prescriptive due to a lack of sufficient evidence. As newer treatment strategies emerge and our understanding of existing medications expands, uncertainty grows regarding the optimal management of complex GO.
This systematic review aims to analyze the current evidence regarding immunomodulation in GO to determine the most effective treatment strategies.
Methods
The review was conducted in accordance with PRISMA guidelines (Appendix A) (16). The study protocol was prospectively registered on the PROSPERO database of systematic reviews (CRD42023400285).
A search strategy was developed in collaboration with information specialist librarians [JD, EJ] (Appendix B). Published records were collected by searching systematically on Cochrane (CENTRAL), Embase, MEDLINE, ProQuest, PubMed, SCOPUS, and Web of Science databases with no limits placed on date. Reference lists from the selected studies were assessed against the eligibility criteria (Table 1). Case reports, literature reviews and non-English language papers were excluded. Titles and abstracts were independently screened by two blinded reviewers [SY, SS]. All discrepancies were resolved through discussion with an independent reviewer [JM]. The PICO framework is documented in (Table 2).
Data extraction was performed by two reviewers [AY, SS]. Data were collected and entered into a standardized spreadsheet for analysis. Patient characteristics were reviewed to ensure comparability between studies. Our primary data outcome was CAS. However, where data was not available, alternative scoring methods were extracted, including assessment of TRAb reduction and B cell depletion. Specifically generated composite indices were also included, provided they were supported by an appropriately cited evidence base.
The Cochrane RoB (Risk of Bias) 2 tool (17) was used for randomized trials, whilst non-randomised studies were assessed with the Cochrane ROBINS-I (Risk of Bias in Non-randomized Studies – of Interventions) tool (18). Data was presented using the Robvis tool (19). The risk of bias assessments were conducted by two reviewers [AY, SS] and the same risk of bias tools were used to assess bias in missing data.
Results
Our search strategy identified 4839 records across all seven databases after removal of duplicates. After screening, 41 studies met criteria for inclusion; fourteen randomized controlled trials, four prospective cohort studies, eleven retrospective cohort studies and twelve case series. Reasons for report exclusion are documented in (Figure 1).
PRISMA Flowchart.
(Table 3) presents the characteristics of all 41 studies included in this systematic review. These studies comprise 1546 participants in total. Heterogeneity in outcome measurement, type of drug treatment, drug dosing and duration of treatment is present across all studies. Previous thyroid treatment also varied greatly across all studies. Patient characteristics are presented in (Supplementary Table 5).
Risk of bias was assessed for fourteen RCTs included in this review (Figures 2, 3). All were assessed as having low or some concerns for bias with the exception of Stan et al. (31) which had a serious risk of bias. Concerning non-RCT studies, most had a serious risk of bias mostly due to the lack of control variables and consideration for confounding factors (Figures 4, 5).
Summary plot for risk of bias for randomised trials.
Traffic light plot of the risk of bias for randomised trials using the Robvis tool (22).
Summary plot of risk of bias for non-randomised trials.
Traffic light plot of the risk of bias for non-randomised trials using the robvis tool (22).
(Table 4) demonstrates the CAS outcomes. 24 studies reported CAS as their main outcome and 8 studies included CAS as a secondary outcome. All studies looking at rituximab demonstrated a statistically significant decrease in mean or median CAS score after treatment apart from Stan et al. (31) which showed no significant difference compared with placebo. Similarly, teprotumumab was shown to significantly improve CAS score but did not show any significant change in Douglas et al. (41). Doxycycline demonstrated a reduction in the number of patients with a CAS score of 3 and above in Matoc et al. (49) but did not show any statistically significant changes in Pan et al. (43). Methotrexate with either reduced- or full-dose methylprednisolone (44) showed a non-significant change in CAS. All studies looking at tocilizumab showed a significant improvement in CAS score.
Twenty studies reported proptosis as their main outcome. Nine further studies reported proptosis as a secondary outcome. These results are shown in (Supplementary Table 6). Teprotumumab consistently demonstrated the greatest improvement in proptosis, with clinically meaningful reductions across all studies. Similarly, studies looking at tocilizumab also showed consistent and statistically significant reduction. Placebo groups consistently showed little to no change, reinforcing the treatment effect observed with teprotumumab and tocilizumab. The rest of the results were generally mixed, with some studies showing benefit with treatment and others less clear. The quality of data was varied and some studies did not provide data on significance or were statistically insignificant. Studies looking at rituximab yielded variable results, as the improvements were minimal with inconsistent significance. Overall, teprotumumab and tocilizumab appear to be the most effective in reducing proptosis.
Reduction in TRAb levels is documented in (Supplementary Table 7). While almost all studies recorded baseline thyroid function tests, only eleven studies measured levels of TRAb in patients. Definite improvements in TRAb levels with tocilizumab use cannot be concluded as there is a statistically significant reduction seen in Ceballos-Macias et al. (36) and Perez-Moreiras et al. (40), but not in Moi et al. (38) and Farde et al. (53). With the exception of Hoang et al. (47) and Deltour et al. (36), all other study results showed no significant change in TRAb associated with treatment.
B Cell depletion is documented in (Supplementary Table 8). In total, five studies investigated the immunomodulatory effects of rituximab (27, 29, 31, 37, 51). All studies showed that rituximab treatment was associated with a reduction in B lymphocyte count.
There were seven studies that reported QoL, in all cases as a secondary outcome and these are presented in (Supplementary Table 9) (35, 45, 47–49, 52, 60). With the exception of Insull et al. (34), who developed their own questionnaire for the purposes of their trial, all of these studies reported QoL with the Graves’ Ophthalmopathy Quality of Life (GO-QOL) questionnaire, which indicates greater QoL as the total score increases (54). Adverse events from the studies are listed in (Supplementary Table 10**).**
Discussion
Overall, this review exhibits a benefit in the use of immunomodulators for thyroid eye disease. While this was seen across the majority of studies included in this review, results were limited by small sample sizes, heterogeneity in outcomes, variability in follow up times and variations in drug comparison.
Rituximab
Although studies on rituximab showed reductions in CAS, proptosis, and B cell levels, the broader evidence base remains mixed. Two key RCTs assessed rituximab in patients with active, moderate-to-severe GO: one against IV methylprednisolone (61) and one against placebo (33). Salvi et al. (61) found significantly greater CAS improvements in the rituximab arm, with 100% of patients showing improvement at 24 weeks compared to 69% in the steroid arm (p<0.001). In contrast, Stan et al. (33) reported no difference between rituximab and placebo (p=0.75). The discrepancy may be due to differences in disease duration as the patient cohort in the Salvi et al. (61) trial had a shorter average duration of GO. Overall, these findings suggest rituximab could be effective for active GO, however the evidence is limited and further head to head studies are required to compare rituximab against newer immunomodulators such as tocilizumab and teprotumumab.
Furthermore, its use is recommended only in specialized centres due to potential serious adverse events (AEs). Dysthyroid optic neuropathy and severe infusion reactions were reported in the RCTs (33, 61). One study (28) reported a cardiac arrest following a second infusion, resulting in patient death. While causality is unclear, rituximab has been associated with cardiac events such as hypotension, arrhythmia, and cardiogenic shock. A meta-analysis by Shen et al. found inconsistent rates of serious AEs (62). These findings support the cautionary stance in current guidelines (4).
Tocilizumab
Tocilizumab is shown to effectively reduce CAS and proptosis in multiple observational studies. In Europe, Tocilizumab has been licensed for the treatment of severe rheumatoid arthritis, systemic juvenile idiopathic arthritis, juvenile polyarthritis, giant cell arthritis, cytokine release syndrome and even COVID-19 but not yet for managing GO (63). The study by Perez-Moreiras et al. (35) remains the only RCT looking at tocilizumab in the context of treating GO. The trial provided encouraging evidence for the use of tocilizumab but there were several limitations that could have impacted the overall outcomes. Firstly, the sample size was relatively small, reducing statistical power and leading to potential imbalance between study groups. For example, the baseline GO-QoL score in the tocilizumab group was considerably higher (median 72.2) compared with the placebo group (median 25.0), which may have allowed greater scope for improvement in the latter. Furthermore, there was no limit to disease duration in the inclusion criteria leading to heterogeneity in disease chronicity. This raises the possibility that some participants were not in the active phase of GO at the time of the trial. These factors lead to uncertainty when directly comparing the two cohorts and may have affected the magnitude of treatment response. Nonetheless, despite these methodological limitations, the evidence from the RCT suggests that tocilizumab has positive therapeutic effects, even among patients with long standing disease.
Generally, the safety profile for tocilizumab is favourable, with most patients experiencing mild to moderate side effects. Neutropenia is a recognised side effect of tocilizumab however the studies observed that this was usually transient and resolved with the discontinuation of therapy. Moi et al. (42) reported three cases of malignancy diagnosed after treatment with tocilizumab. Causality cannot be confirmed given the observational nature of the findings and tocilizumab is not known to be associated with an increased risk of cancer. Instead, the observed association may reflect the underlying predisposition linked to autoimmune thyroid disease which has been associated with a higher incidence of certain malignancies – most commonly thyroid, breast, head and neck (64).
Teprotumumab
Evidence from included studies suggests that teprotumumab is a promising therapy for the treatment of active GO with mild side effects. Smith et al. (34) and Douglas et al. (38) conducted RCTs with comparable designs and sample sizes, both of which found teprotumumab superior to placebo in improving CAS, proptosis, and QoL. Patients with the highest initial proptosis levels appeared to have the largest reductions with teprotumumab, highlighting its efficacy in moderate to severe disease. Patients also experienced rapid therapeutic effects; in Smith et al. 43% achieved a meaningful proptosis response in 6 weeks and Douglas et al. reported a median time to response of 6.4 weeks. In these studies, data was limited on the durability of efficacy in patients with longstanding TED. A follow up study by Douglas et al. (45) looked at the effect on patients with long duration and low disease activity which again demonstrated good treatment effect, highlighting its efficacy regardless of disease severity and duration. However, the open-label design and high loss to follow-up introduces potential bias, highlighting the need for further RCTs to confirm these findings.
Adverse events (AEs) were mostly mild; each RCT reported two serious AEs, with some deemed potentially treatment related. A major recognised side effect of teprotumumab is hearing loss and this was experienced by patients across several studies. Centres delivering teprotumumab should consider regular audiometry and protocols to manage hearing loss associated with its use (65). Overall, current evidence supports the efficacy and general safety of teprotumumab for active GO. However, due to the paucity of data; further research is warranted, in particular long-term and comparative studies. EUGOGO guidelines recommend teprotumumab as a second-line treatment option (4).
DMARDs
Among the included studies, cyclosporine and methotrexate were evaluated as steroid-sparing agents. Cyclosporine was primarily studied in combination with corticosteroids, limiting the ability to assess its independent efficacy. Meyer et al. reported full visual recovery in patients with dysthyroid optic neuropathy treated with IV methylprednisolone, oral prednisolone, and cyclosporine, but did not report outcomes relevant to this review, such as CAS, proptosis, or QoL (25). Utech et al. (21) found proptosis normalized in 20 of 39 patients treated with cyclosporine and prednisolone. A previous RCT showed cyclosporine alone was less effective than prednisolone (22% vs. 61% response rate; p=0.018), although combination therapy improved outcomes in treatment-resistant patients (66).
Methotrexate was studied in two trials. Shen et al. (48) found no significant differences in CAS, proptosis, or QoL across treatment groups, but reported fewer adverse events in the methotrexate plus reduced-dose methylprednisolone group (p=0.017). Another study of 24 patients receiving methotrexate and IV methylprednisolone showed significant improvements in VISA (an alternative scoring system to CAS) at both intermediate and long-term follow-up, with no serious adverse events reported (67). However, the concurrent use of adjunctive treatments (e.g. cyclosporine, azathioprine, rituximab) are confounding factors and limit the reliability of these findings.
Overall, the evidence supports the potential role of steroid-sparing agents, particularly in combination with corticosteroids. This aligns with EUGOGO guidelines, which recommend IV methylprednisolone in combination with agents like cyclosporine or orbital radiotherapy to enhance steroid efficacy (4). Cyclosporine in combination with oral steroids is considered a valid second-line option, with azathioprine and mycophenolate also noted. Methotrexate, however, is not currently endorsed, likely due to limited supporting data.
IV Immunoglobulins
IVIG was assessed in two studies, both showing some benefit in reducing proptosis, with Kahaly et al. (22) also noting a reduction in TRAb levels (20, 22). Neither study reported serious adverse events, though IVIG carries a small potential risk of transmitting viral infections, such as HIV and hepatitis B, as it is a blood product (68). Additionally, the need for intravenous administration and associated high costs, limit its practical use. As such, IVIG is not currently considered a viable treatment option for GO (4).
Other drugs
This review also examined two drugs not routinely used for GO: octreotide and doxycycline. While Ozata et al. (23) reported a reduction in proptosis with octreotide, subsequent studies have shown limited benefit. Three double-blind RCTs on long-acting release octreotide (octreotide-LAR) failed to demonstrate significant improvements in disease outcomes. Dickinson et al. (24) found no benefit in moderately severe GO. Stan et al. reported improvement in CAS but was noted to have overrepresentation of patients with higher baseline CAS in the octreotide-LAR group as well as a small control group (33). The third trial noted a reduction in proptosis but no effect on disease activity in mild cases (69). These RCTs suggest octreotide is not a suitable immunomodulator for GO. This is the position of the EUGOGO guidelines (4), which cite these RCTs as evidence. The guidelines also cite evidence from an RCT on lanreotide, showing no significant differences in CAS or proptosis compared to placebo (70).
Regarding doxycycline, limited evidence is available on its efficacy as an immunomodulator in GO; there is also no advice in the EUGOGO guidelines (4). A 2015 case series reported improvements in CAS and soft tissue swelling in 8/13 patients after treatment with doxycycline (71). However, the small sample size and lack of control group limit the generalizability. Another study in the same year showed improvements in CAS and proptosis with a combined regimen of doxycycline and steroids, though the efficacy of doxycycline alone remains unclear (72). Matoc et al. (55) conducted an RCT that demonstrated significant improvements in quality of life (QOL) and CAS. Although the study reported low rates of adverse events, these findings should be interpreted with caution due to the short duration of the trial and the small sample size. Additionally, the lack of a placebo group, with no treatment as the comparator, limits the ability to draw definitive conclusions about the true efficacy of the intervention.
Limitations
Due to the heterogeneity of the studies in this review, conducting a meta-analysis was not feasible. This was particularly evident in the reported outcomes. Not every study reported the primary outcome of CAS and there was significant variation in secondary outcomes across all studies. Direct comparison between studies was also limited by a lack of consistency in the reporting of outcomes. Some utilized mean, others median and some even categorical. Furthermore, all the studies consisted of a small number of participants, with 119 patients being the highest patient cohort in a study, limiting the extent to which their results can be extrapolated. The review was also limited to English language studies, which could have excluded other relevant research and introduced bias.
The risk of bias assessments revealed several concerns, particularly in non-randomized trials. These included confounding bias (Domain 1), bias due to missing data from loss to follow-up (Domain 2), outcome measurement bias (Domain 6), and selective reporting (Domain 7). Confounding bias was especially prevalent, often stemming from study designs that allowed prior or concurrent treatments without proper adjustment. For example, Insull et al. (37) investigated rituximab but IV methylprednisolone and optional methotrexate was also concurrently used, without accounting for these confounders.
In contrast, RCTs generally showed a lower risk of bias, though most concerns were highlighted in the randomization process (Domain 1) and bias in the selection of reported results (Domain 5). Overall, this systematic review highlights serious risk of bias in the current literature, especially in non-randomized trials. Future non-randomized studies should adhere more closely to Cochrane ROBINS-I guidelines, particularly by applying statistical methods—such as stratification, regression, matching, standardization, or inverse probability weighting—to control for confounding. Notably, these methods were rarely, if ever, used in the studies reviewed.
Implications for practice and policy
Overall, this systematic review suggests that tocilizumab and teprotumumab are effective in treating Graves’ orbitopathy (GO), particularly in reducing CAS and proptosis. Combination therapy with steroids and steroid-sparing agents also show benefit. This is seen in Meyer et al. (25) and Shen et al. (48), where both treatments reduced proptosis, with the latter also reducing CAS and TRAb levels. However, based on the data alone, determining the optimal treatment for clinical practice remains challenging. There is a lack of statistical analyses across the studies and variability in methodology such as dosing and outcome measurements prevents direct comparisons between newer and older treatment methods. Dosage and frequency varied even within observational studies looking at a single drug. Heterogeneity of results and methodologies prevent meaningful comparisons of interventions. It highlights the need to standardize outcome measurements for future research. Establishing clinically significant thresholds for improvements in CAS and proptosis would be beneficial in facilitating more reliable comparisons and to establish the true efficacy of emerging therapies.
Additionally, factors such as cost, availability, and patient preferences play a significant role in treatment decisions. While biologics like tocilizumab and teprotumumab may offer greater efficacy and fewer adverse events than established treatments, their high costs limit their widespread use. One treatment course of Teprotumumab costs approximately 360,000 US dollars (73). This is perhaps the reason as to why Teprotumumab is still not widely available in most countries and has only recently been approved in Europe (74). Given this statistic, it is unlikely to be financially viable for public health systems to afford such agents as first line when treatments like steroids are cost-effective and widely accessible. This is also compounded by the fact that other agents, such as rituximab and tocilizumab, may offer similar efficacy in treating active GO and are in comparison less expensive. Furthermore, tocilizumab is available as a subcutaneous preparation, allowing patients to self- administer the treatment at home without having to attend a specialist unit. This could reduce the overall cost burden, as the IV preparation is three times more expensive than the subcutaneous form (75). However, this has yet to be explored in RCTs for GO and could represent a promising avenue for further research to evaluate its efficacy and cost-effectiveness. The EUGOGO guidelines also note the need for further data on teprotumumab’s affordability before it can be considered for first-line use (4). This demonstrates the importance of early referral to specialist centers (e.g. joint thyroid-eye clinics), where a multidisciplinary approach can tailor treatment options to improve patient outcomes.
Implications for research
While this systematic review has identified a substantial body of research on GO treatment, there are several ways in which this can be improved and built upon. This review has highlighted the need for higher quality primary studies (i.e. RCTs) with large sample sizes, as the majority of studies were small and non-randomized.
Several studies in this review included IV methylprednisolone as part of their treatment regimens, however none compared it to biologics or steroid-sparing agents directly. Similarly, there is a paucity of data on methotrexate as a treatment for GO compared to other steroid-sparing agents. Given the evidence that combination therapy with steroids is more efficacious than steroid-sparing drugs in isolation, there is arguably scope for further RCTs investigating the combined efficacy of methotrexate with steroids, as done by Shen et al. (48).
Emerging treatments also merit further investigation. Long-term RCTs comparing teprotumumab with IV steroids would be beneficial in establishing its safety, sustained efficacy and cost effectiveness. Although teprotumumab is now approved, it is only recommended as a second-line option for active, moderate-to-severe GO. Relatively few patients meet the eligibility criteria for biologic therapies, and their high costs limit their use as first-line treatments within public health systems. Consequently, conducting large-scale RCTs for agents such as teprotumumab can be challenging in some settings. Further research in this area may become possible as teprotumumab becomes more widely accessible.
Similarly, doxycycline requires further evaluation beyond short-term outcomes; additional RCTs should also assess its use in both mild and moderate-to-severe GO. If proven to be beneficial, this could change the outlook of GO treatment given its low cost and accessibility. Novel therapies currently in preclinical development, such as small molecule TSHR antagonists, may prove to be an interesting focus for future clinical trials (76).
Conclusion
This systematic review highlights positive outcomes for biologics such as tocilizumab and teprotumumab in reducing CAS and proptosis. However, the evidence is limited by heterogeneity between studies and a lack of direct comparisons with standard treatments, hence this review is not conclusive. Future research in the form of RCTs with head-to-head comparisons between drugs are required in order to influence clinical decision-making. Additional research into emerging therapies such as TSH receptor antagonists, constitutes an important direction for future research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bartalena L Fatourechi V . Extrathyroidal manifestations of Graves’ disease: a 2014 update. J Endocrinol Invest. (2014) 37:691–700. doi: 10.1007/s 40618-014-0097-2, PMID: 24913238 · doi ↗ · pubmed ↗
- 2Cockerham KP Chan SS . Thyroid eye disease. Neurol Clin. (2010) 28:3. doi: 10.1016/j.ncl.2010.03.010, PMID: 20637998 · doi ↗ · pubmed ↗
- 3Perros P Hegedüs L Bartalena L Marcocci C Kahaly GJ Baldeschi L . Graves’ orbitopathy as a rare disease in Europe: a European Group on Graves’ Orbitopathy (EUGOGO) position statement. Orphanet J Rare Dis. (2017) 12:1. doi: 10.1186/s 13023-017-0625-1, PMID: 28427469 PMC 5397790 · doi ↗ · pubmed ↗
- 4Bartalena L Kahaly GJ Baldeschi L Dayan CM Eckstein A Marcocci C . The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. (2021) 185:4. doi: 10.1530/EJE-21-0479, PMID: 34297684 · doi ↗ · pubmed ↗
- 5Cawood T Moriarty P O’Shea D . Recent developments in thyroid eye disease. BMJ. (2004) 329:7462. doi: 10.1136/bmj.329.7462.385, PMID: 15310608 PMC 509348 · doi ↗ · pubmed ↗
- 6Eckstein AK Plicht M Lax H Neuhäuser M Mann K Lederbogen S . Thyrotropin receptor autoantibodies are independent risk factors for graves’ Ophthalmopathy and help to predict severity and outcome of the disease. J Clin Endocrinol Metab. (2006) 91:9. doi: 10.1210/jc.2005-2813, PMID: 16835285 · doi ↗ · pubmed ↗
- 7Diana T Ponto KA Kahaly GJ . Thyrotropin receptor antibodies and Graves’ orbitopathy. J Endocrinol Invest. (2021) 44:4. doi: 10.1007/s 40618-020-01380-9, PMID: 32749654 PMC 8310479 · doi ↗ · pubmed ↗
- 8Gillespie EF Smith TJ Douglas RS . Thyroid eye disease: towards an evidence base for treatment in the 21st century. Curr Neurol Neurosci Rep. (2012) 12:3. doi: 10.1007/s 11910-012-0256-9, PMID: 22354545 PMC 3463137 · doi ↗ · pubmed ↗