Intratesticular Fetus in Fetu Arising from an Intra-Abdominal Undescended Right Testis: A Case Report
Fuminori Numano, Noboru Oyachi, Satoshi Shinohara, Rei Sunami

TL;DR
A rare case of fetus in fetu was found inside an undescended testis in a newborn, highlighting an unusual congenital anomaly.
Contribution
Reports a novel case of intratesticular fetus in fetu arising from an undescended testis, expanding clinical understanding.
Findings
Fetus in fetu was identified within an intra-abdominal undescended right testis in a neonate.
Histopathology confirmed vertebral-like structures within the mass, with no testicular tissue present.
The mass was tethered to the inguinal ring, suggesting a vascular connection during fetal development.
Abstract
Fetus in fetu (FIF) is a rare congenital anomaly. The most common location of FIF is the retroperitoneum. FIF of testicular origin is extremely rare, with only 9 cases reported previously. We present a case of intratesticular FIF within an intra-abdominal undescended right testis and review previously reported cases to discuss the possibility of intratesticular FIF. A male neonate was born through normal vaginal delivery at 37 weeks and 5 days of gestation, with a birth weight of 2648 g. An abdominal mass suspected to be a FIF was prenatally detected. At 26 weeks of gestation, fetal ultrasonography revealed a mass measuring 20 mm in diameter that contains structures resembling an embryo and an umbilical cord in the abdominal cavity; however, these structures were no longer identifiable after 29 weeks of gestation. Postnatally, a mass measuring 20 mm in diameter was found in the right…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
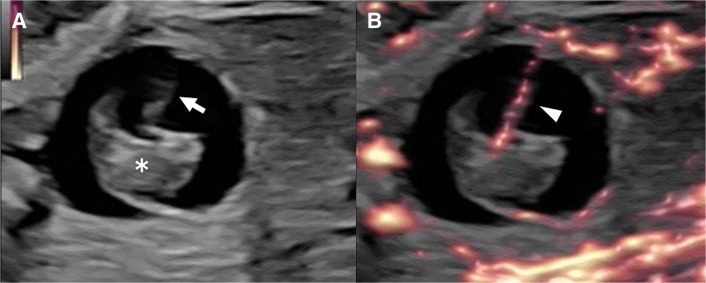 Fig. 1
Fig. 1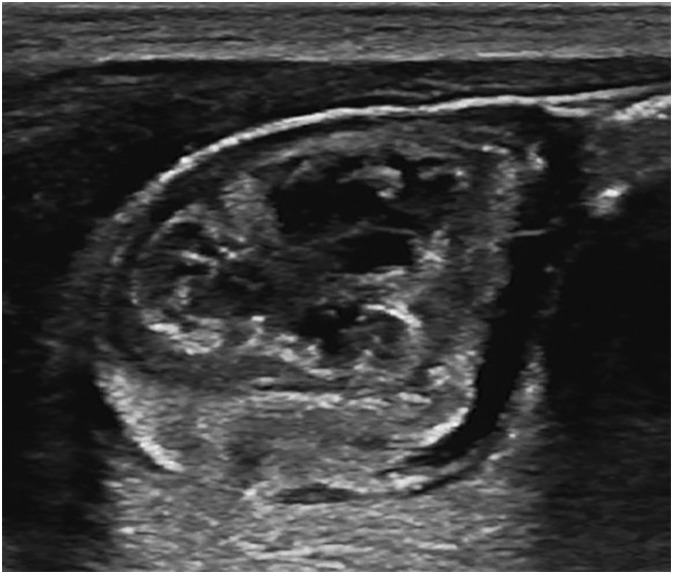 Fig. 2
Fig. 2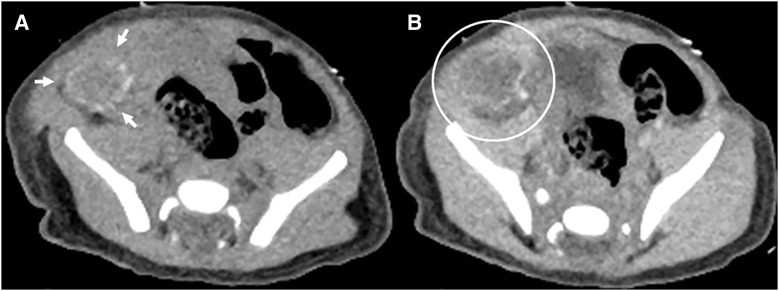 Fig. 3
Fig. 3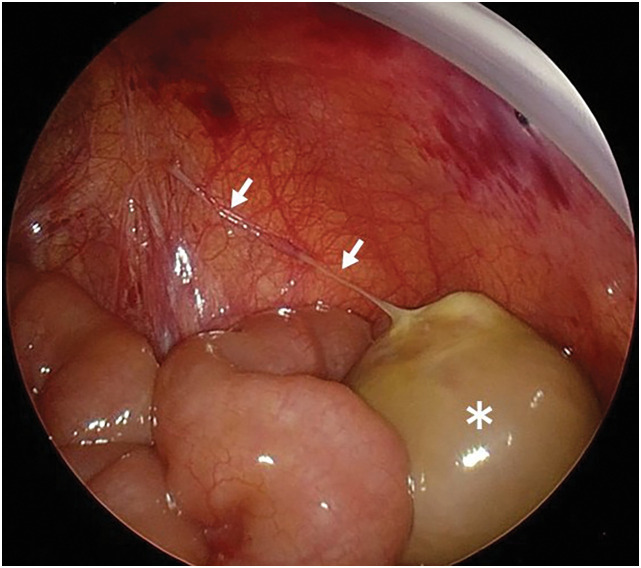 Fig. 4
Fig. 4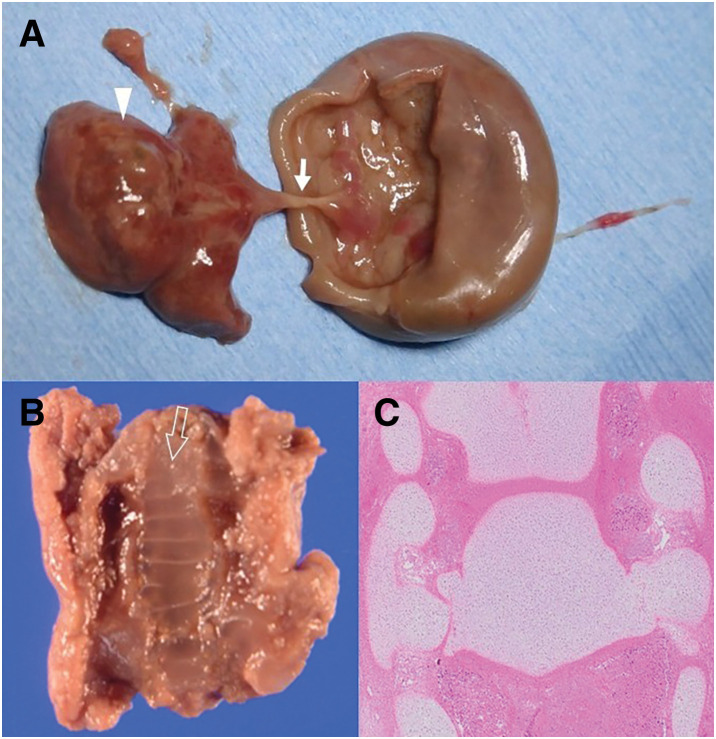 Fig. 5
Fig. 5| Year | Author | Basis for intratesticular FIF | ||
|---|---|---|---|---|
| Absence of normal unilateral testis | Histopathological remnants (testis/epididymis/spermatic cord) | Presence of FIF in the scrotum | ||
| 1972 | Kakizoe | Yes; Left | No | Yes |
| 1985 | Alpers | Yes; Left | Yes | No; intra-abdominal |
| 1990 | Chateil | Yes; Right | Yes | No; intra-abdominal |
| 1999 | Shin | Yes; Right | Yes | Yes |
| 2015 | Ji | Yes; Right | Yes | Yes |
| 2016 | Landmann | Yes; Right | Yes | No; intra-abdominal |
| 2016 | Khope | Yes; Left | Yes | Yes |
| 2022 | Heitman | Yes; Left | Yes | Yes |
| 2024 | Luo | Yes; Left | Yes | No; intra-abdominal |
| 2026 | Current case | Yes; Right | No | No; intra-abdominal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Assisted Reproductive Technology and Twin Pregnancy · Teratomas and Epidermoid Cysts
Abbreviation
FIF fetus in fetu
INTRODUCTION
FIF is a rare congenital anomaly characterized by the presence of a malformed parasitic fetus incorporated into the body of the host fetus. The estimated incidence is approximately 1 in 500000 live births. Most cases arise in the retroperitoneum, and only a few cases have been reported in the testis to date. In this report, we describe a case of intra-abdominal FIF presumed to have originated from the right testis, based on characteristic gross and histopathological findings. In addition, we review previously reported cases to discuss the possibility of intratesticular FIF.
CASE PRESENTATION
We present the case of a male neonate born at 37 weeks and 5 days of gestation through normal vaginal delivery, with a birth weight of 2648 g. Antenatal sonography at 23 weeks of gestation revealed a 10-mm intra-abdominal cystic mass at the lower pole of the right kidney. At 26 weeks of gestation, the cystic mass enlarged to 20 mm in diameter. Solid components resembling an embryo and a cord-like structure with blood flow resembling an umbilical cord were observed inside the cystic mass; therefore, FIF was suspected (Fig. 1). However, by 29 weeks of gestation, these structures had collapsed, and the contents of the mass had become heterogeneous without detectable blood flow. Thereafter, the size and internal structure of the mass remained unchanged until birth.
Ultrasound findings at 26 weeks of gestation. (A) Cystic mass, 20 mm in diameter, with an internal solid structure (asterisk) and a cord-like structure (arrow). (B) Cord demonstrating blood flow (arrowhead). The solid structure resembles an embryo, and the cord-like structure resembles an umbilical cord.
Postnatally, ultrasonography demonstrated a 20-mm mass in the right lower abdomen. The mass was mobile, well defined, heterogeneous, and hypovascular (Fig. 2). Abdominal CT revealed a low-density mass located on the right side of the bladder, with annular calcifications along its margin. Contrast-enhanced CT showed no enhancement within the mass (Fig. 3). MRI demonstrated an organized hematoma within the mass on the cephalic side of the bladder. The left testis was normal in size and morphology; however, the normal right testis was not identified.
Postnatal ultrasound findings. A 20-mm abdominal mass observed in the right lower abdomen.
CT findings. (A) Plain CT showing a low-density mass with annular calcifications at the margins (arrows). (B) Contrast-enhanced CT showing no contrast enhancement in the mass (circle).
The patient’s general condition was stable; therefore, elective laparotomy was performed through a right lower transverse incision on the 15th day of life. Intraoperatively, a 20-mm oval mass with a smooth surface was identified, anchored by a single thin fibrous band. Laparoscopic inspection of the abdominal cavity confirmed that the mass was located in the right lower abdomen and that the fibrous band was connected to the right internal inguinal ring, without any additional adhesions (Fig. 4). The mass was detached from its attachment and completely excised.
Surgical findings. A 20-mm oval mass with a smooth surface in the right lower abdomen (asterisk) anchored by a single thin fibrous band connected to the right internal inguinal ring (arrows).
Gross examination of the excised specimen revealed a peach-colored, muddy hematoma and firm, solid structures resembling bone. The solid structures were connected to the inner wall of the mass through a cord-like structure and grossly resembled an embryo and an umbilical cord (Fig. 5A). On coronal sectioning, the solid structures were arranged in a ladder-like configuration, resembling a vertebral column (Fig. 5B). Histopathological examination demonstrated cartilage within the solid structures, which exhibited a regular, segmental arrangement consistent with vertebral elements (Fig. 5C). The cord-like structure was confirmed to be a blood vessel on histopathological examination. Accordingly, the solid and cord-like structures were considered consistent with a fetus and an umbilical cord, respectively. The single thin fibrous band anchoring the mass contained vessels but no vas deferens, and no testicular or epididymal remnants were identified within the mass.
Gross and histopathological findings of the excised specimen. (A) Solid structures (arrowhead) connected to the inner wall of the mass through a cord-like structure (solid arrow). (B) Solid structures on coronal section, showing a ladder-like arrangement (open arrow). (C) Histopathological examination of the coronal section contain cartilage and exhibit a regular and segmental arrangement.
Based on the characteristic gross and histopathological findings and the absence of a normal right testis, the lesion was considered most consistent with FIF arising within an intra-abdominal undescended right testis. Although the fibrous band did not contain a histologically identifiable vas deferens, it was considered as the feeding vessel of the mass and possibly a remnant of the spermatic cord, based on its gross morphology.
DISCUSSION
FIF is a rare congenital malformation first described by Meckel in the 18th century.^1)^ The most common location of FIF is the retroperitoneum, whereas atypical locations include the intracranial and oral cavities, neck, adrenal gland, liver, scrotum, pelvis, and mediastinum.^2)^ The reported male-to-female ratio is approximately 1.1:1, indicating a slightly higher incidence in males.^3)^ The clinical presentation is nonspecific and depends on the size and location of the lesion. FIF may be detected incidentally or may present with symptoms caused by compression of adjacent structures.^4,5)^ The etiology is believed to involve defective implantation. During the second week of development in multiple pregnancies, one or more embryos may invade the extra-embryonic mesenchyme of the dominant embryo instead of the uterine wall. Following the development of the primitive streaks, as the dominant embryo undergoes delimitation, another embryo may be incorporated within its mesenchyme. This results in parasitic, non-dominant fetuses with vascular connections embedded in various regions of the mesenchymal components of the dominant embryo.^6)^ Currently, no established guidelines exist regarding the treatment or postoperative follow-up of FIF. Although FIF is generally considered benign, complete surgical resection is the recommended treatment, and prognosis is favorable in most cases. However, intracranial FIF grows within the host brain parenchyma, causing severe compression of surrounding brain tissue and accumulation of cerebrospinal fluid, leading to increased intracranial pressure. Consequently, intracranial FIF is associated with a poor prognosis, regardless of whether complete resection is achieved.^7)^ In addition, several reports have described recurrence as teratoma or malignant transformation following incomplete excision.^8–10)^ Therefore, complete excision is recommended; however, careful postoperative surveillance is warranted when complete excision cannot be achieved.^2,4)^
Distinguishing FIF from teratomas is crucial for accurate diagnosis. FIF is widely recognized as a clinical entity distinct from teratomas, and radiographic or pathological evidence of a vertebral structure is considered essential for diagnosis.^11)^ Willis^12)^ and Lord^13)^ argued that FIF is fundamentally distinct from a teratoma. Willis suggested that the diagnosis of FIF should be limited to cases demonstrating a definitive vertebral column, as teratomas lack vertebral structures because they do not pass through the period of primitive streak formation required for vertebral development. Lord further emphasized that a true diagnosis of FIF requires unequivocal radiographic or anatomical demonstration of part or all of the vertebral axis. In contrast, some authors have argued that FIF may represent a highly developed or complex form of teratoma.^14)^ Teratomas, despite containing well-organized structures, are neoplasms originating from embryonic pluripotent cells.^3)^ Several cases have been reported in which FIF was diagnosed based on advanced structural organization despite the absence of a defined vertebral column.^15,16)^ However, these cases are not consistent with the widely accepted clinical entity, and cases lacking vertebral structures remain a matter of debate.
As previously mentioned, FIF can occur in various anatomical locations and may also develop within an intra-abdominal undescended testis. Although intratesticular FIF has been hypothesized to originate from primordial germ cells,^17)^ its etiology remains unclear and could not be definitively determined in the current case. To date, only 9 cases of intratesticular FIF have been identified in a PubMed search, underscoring the rarity of this condition. Table 1 summarizes the characteristics of all 10 cases,^2,11,17–23)^ including the current case. All reported cases underwent surgical excision and had uneventful prognoses. The intratesticular FIF was located in the scrotum in 5 cases and in the abdominal cavity in the remaining 5 cases. The affected testis replaced by FIF was on the left side in 5 cases and on the right side in the remaining 5. Residual tissue of the testis, epididymis, or spermatic cord was identified in 8 but not in 2 cases (the current case and the case reported by Kakizoe and Tahara^18)^). These findings suggest that the testis may be completely replaced by FIF and that testicular descent from the retroperitoneum to the scrotal sac can occur even in such cases. Taken together, the findings from the current and previously reported cases suggest that intratesticular FIF should be considered when a unilateral testis cannot be identified and FIF is located in proximity to the normal pathway of testicular descent.
In the current case, the diagnosis of FIF was not based on the presence of an advanced degree of fetal organization but rather on the identification of a vertebral column. Solid components and a cord-like structure with blood flow observed within the mass at 26 weeks of gestation were subsequently shown on histopathological examination to contain vertebral elements and blood vessels, respectively, suggesting the presence of a parasitic fetus and an umbilical cord. However, these structures were no longer visible after 29 weeks of gestation, presumably reflecting failure of the feeding vessels, leading to hemorrhage, necrosis, and degeneration of the FIF. In addition, the normal right testis could not be identified. The oval mass was located in proximity to the normal pathway of testicular descent, and the fibrous band originating from the internal inguinal ring was considered to represent the feeding vessel of the mass. The gross morphology of the mass and fibrous band resembled that of the testis and the spermatic cord. Nevertheless, histopathological evidence of testicular, epididymal, or spermatic cord tissue could not be demonstrated. The testis is a common site for teratomas, and the etiology of FIF remains under debate; therefore, the possibility that the current case represents a teratoma cannot be completely excluded. However, based on the presence of a vertebral column, the absence of a normal unilateral testis, the location of the mass in proximity to the normal pathway of testicular descent, and the gross morphology of the mass and fibrous band, this case was considered most consistent with an intratesticular FIF arising from an intra-abdominal undescended right testis.
CONCLUSIONS
We report a case of FIF detected prenatally and successfully resected during the neonatal period, with a favorable outcome. Although the distinction between FIF and teratoma remains a matter of debate, the current case shares key clinical, gross, and histopathological features with previously reported cases. Based on these findings, this case was considered consistent with intratesticular FIF arising from an intra-abdominal undescended right testis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chua JHA, Chui CH, Sai Prasad TR, et al. Fetus-in-fetu in the pelvis: report of a case and literature review. Ann Acad Med Singap 2005; 34: 646–9.16382253 · pubmed ↗
- 2Ji Y, Song B, Chen S, et al. Fetus in fetu in the scrotal sac: case report and literature review. Medicine (Baltimore) 2015; 94: e 1322.26266375 10.1097/MD.0000000000001322 PMC 4616709 · doi ↗ · pubmed ↗
- 3Palo S, Mangla M, Gabbeta S, et al. Demystifying fetus-in-fetu: a systematic review of its clinical and pathological attributes. J Indian Assoc Pediatr Surg 2024; 29: 406–16.39479419 10.4103/jiaps.jiaps_67_24PMC 11521215 · doi ↗ · pubmed ↗
- 4Rahman GA, Abdulkadir A, Abdur-Rahman LO. Fetus-in fetu: a review article. Eur J Sci Res 2007; 18: 663–73.
- 5Sinha S, Sarin YK, Khurana N. Prenatally diagnosed retroperitoneal fetus-in-fetu with ipsilateral testicular atrophy: a case report. J Neonatal Surg 2012; 1: 41.26023400 PMC 4420410 · pubmed ↗
- 6Cingel V, Durdik S, Babala J, et al. Fetus in fetu from newborn’s mediastinum: case report and a review of literature. Surg Radiol Anat 2012; 34: 197–202.21901374 10.1007/s 00276-011-0868-9 · doi ↗ · pubmed ↗
- 7Qin X, Chen X, Zhao X, et al. Intracranial parasitic fetus in a living infant: a case study with surgical intervention and prognosis analysis. Am J Case Rep 2024; 25: e 944371.38902917 10.12659/AJCR.944371 PMC 11334086 · doi ↗ · pubmed ↗
- 8Hopkins KL, Dickson PK, Ball TI, et al. Fetus-in-fetu with malignant recurrence. J Pediatr Surg 1997; 32: 1476–9.9349774 10.1016/s 0022-3468(97)90567-4 · doi ↗ · pubmed ↗