Variation in the Management of Test Results after Hospital Discharge: A Pediatric Safety Concern
Meenu Krishnasamy, Rhiya Sharma, Lydia Nashed, Khoa Luong, Courtney Port

TL;DR
This study shows that managing test results after pediatric hospital discharge is a safety concern due to inconsistent practices and unclear responsibilities.
Contribution
The paper provides insights into pediatric hospitalists' and residents' practices and perceptions regarding test result follow-up after discharge.
Findings
Many hospitalists reported missing test results, but few linked it to care delays.
Most hospitalists and residents want a standardized process for managing test results.
Residents were more likely to prefer shared responsibility for test result follow-up.
Abstract
Delay or failure to follow up tests pending at discharge (TPAD) is a major safety concern and a focus in the literature, but few studies exist in the pediatric context. We aimed to explore pediatric hospital medicine physicians’ practices and perceptions of the management of TPAD. Surveys were provided to hospitalists and residents at a single institution using selected questions from a published national adult primary care survey and newly developed questions. Results were analyzed using descriptive statistics and Fisher’s exact tests. Surveys were completed by 25 hospitalists (89%) and 25 residents (68%). Forty-four percent (n = 11) of hospitalists reported missing test results, yet only 18% (n = 2) agreed that this error led to a delay in care. Seventy-six percent (n = 19) of hospitalists reported lacking adequate assistance to manage TPAD. There is uncertainty about who is…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
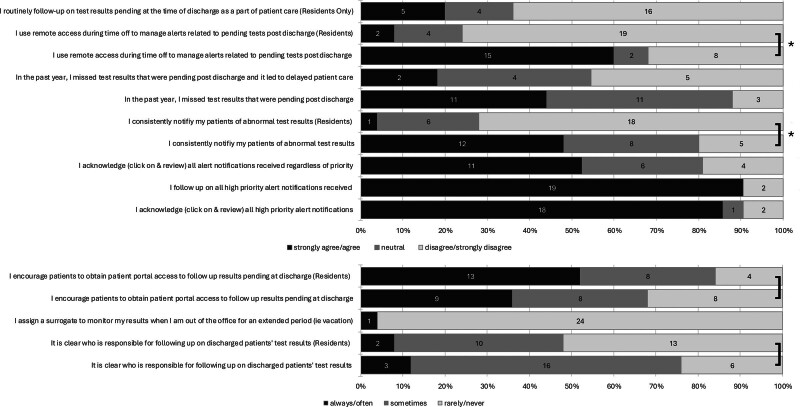 Fig. 1
Fig. 1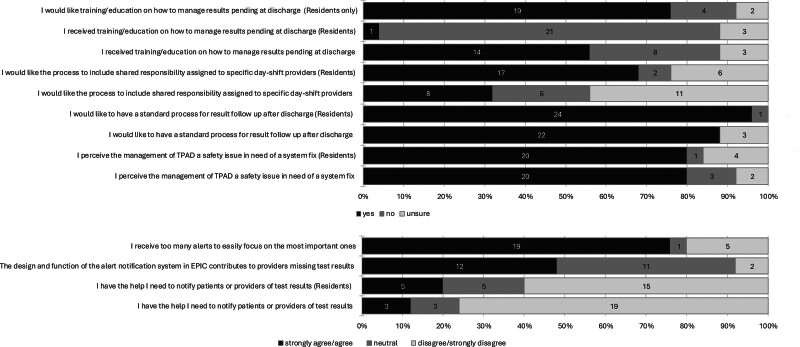 Fig. 2
Fig. 2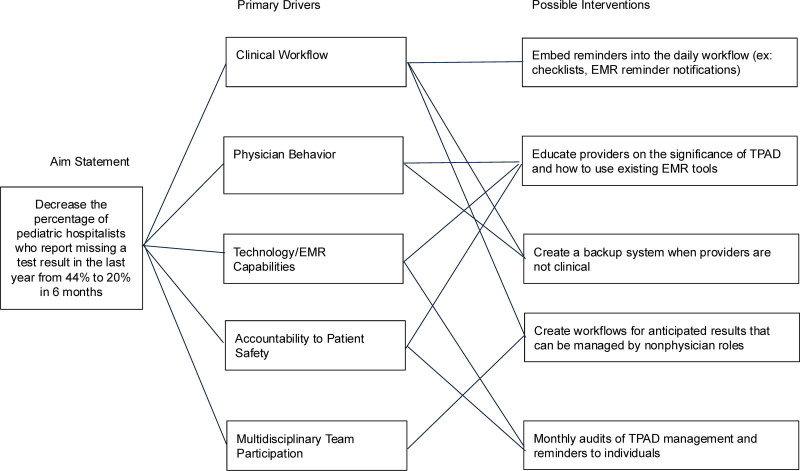 Fig. 3
Fig. 3| Use of Information Technology Tools | Yes | No | Unsure | ||||
|---|---|---|---|---|---|---|---|
| I use the in-basket to follow up on TPAD | 21 | 84% | 4 | 16% | n/a | n/a | |
| I use the sort function in my in-basket results according to urgency, patient name, location, or alert date/time | 2 | 8% | 18 | 72% | 1 | 4% | |
| I have remote access to the EMR | 23 | 92% | 2 | 8% | n/a | n/a | 0.99 |
| Residents | 24 | 96% | 0 | 0% | 1 | 4% | |
| I use the mobile EMR App on my personal cell phone | 17 | 68% | 8 | 32% | n/a | n/a |
|
| Residents | 24 | 100% | 0 | 0% | 0 | 0% | |
| I use at least 1 manual cognitive reminder for TPAD | 18 | 72% | 7 | 28% | n/a | n/a |
|
| Residents | 5 | 20% | 20 | 80% | n/a | n/a | |
| Cognitive reminder: add to a reminder list in the EMR | 4 | 16% | 21 | 84% | n/a | n/a | 0.67 |
| Residents | 2 | 8% | 23 | 92% | n/a | n/a | |
| Cognitive reminder: add to a personal follow-up list in the EMR | 11 | 44% | 14 | 56% | n/a | n/a | 0.06 |
| Residents | 4 | 16% | 21 | 84% | n/a | n/a | |
| Cognitive reminder: personal electronic or handwritten notes/to-do list | 4 | 16% | 21 | 84% | n/a | n/a | 0.11 |
| Residents | 0 | 0% | 25 | 100% | n/a | n/a | |
| Cognitive reminder: none of the above, I only use the in-basket results | 7 | 28% | 18 | 72% | n/a | n/a |
|
| Residents | 20 | 80% | 5 | 20% | n/a | n/a | |
| Cognitive reminder: other | 0 | 0% | 25 | 100% | n/a | n/a | 0.99 |
| Residents | 1 | 4% | 24 | 96% | n/a | n/a | |
| I use the patient portal to notify patients of test results | 1 | 4% | 24 | 96% | 0 | 0% | 0.99 |
| Residents | 2 | 8% | 20 | 80% | 3 | 12% | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHospital Admissions and Outcomes · Heart Failure Treatment and Management · Clinical Reasoning and Diagnostic Skills
INTRODUCTION
Index Case
Overnight, a pediatric patient with an expected discharge for the following day reported dysuria, prompting the resident physician to order a urine culture. Due to miscommunication, the discharging team was unaware of the pending result. The urine culture, which showed more than 100,000 colony forming units/mL Escherichia coli, was not followed up after discharge. Several days later, the patient returned with urosepsis, requiring intensive care unit–level care before making a full recovery. A brief exploration of test result management after discharge revealed that the average time to mark an in-basket result as “done” during the past year was 8.4 days among all inpatient providers. Notably, there was significant variation across departments, ranging from 0.4 to 44 days.
Background
Within the inpatient medical system, the follow-up of tests pending at discharge (TPAD) is an ongoing patient safety concern identified by several safety organizations.^1,2^ About 40% of patients leave the hospital with at least 1 TPAD.^3^ In 1 systematic review, there was a lack of follow-up on 20%–61% of test results from discharged hospitalized patients; this issue was particularly significant for critical test results.^4^ Although laboratories have policies for critical test result notification, there is great heterogeneity in the content of critical test alert lists.^5^ Depending on patient characteristics, even results of tests deemed “noncritical” could be clinically significant, as demonstrated by our index case. Failure to follow up on TPAD increases the risk of missed or delayed diagnoses, leading to suboptimal clinical outcomes. It may have serious medicolegal implications.^6^ Following the 21st Century Cures Act,^7^ many institutions now release results directly to patient portals. Delays or failures by providers to address these results with patients can erode trust in the healthcare system.^8,9^
Many physicians are aware of this gap in patient safety. Eighty-three percent of surveyed general adult practitioners reported encountering at least 1 delayed test result that affected patient care during the last 2 months.^10^ Additionally, about 30% of primary care providers (PCPs) surveyed reported seeing at least 1 patient in the last month with a missed test result from their inpatient admission.^10^ However, few studies exist describing TPAD management in the pediatric context.^11,12^ Studies among adult patients^13–16^ note large variability in addressing TPAD, a lack of communication between the discharging team and PCP, ambiguity of responsibility, and delays in addressing actionable results. Our study aimed to explore TPAD management practices and perceptions among pediatric hospital medicine (PHM) clinicians at a large suburban center.
METHODS
We conducted a cross-sectional, electronic survey of clinicians at a large mid-Atlantic children’s hospital with 226 pediatric beds and 7000 pediatric admissions annually. Our institution uses Epic Systems Corporation’s electronic health record (Epic, Verona, WI), one of the most widely used systems globally.^17^
The study population included attending PHM physicians (hospitalists), PHM fellows, and pediatric resident physicians. We recruited participants via email and at department meetings. Our team conducted a local needs assessment from July 2023 to October 2023, and our local institutional review board approved the study.
Data Collection
We used a 23-item electronic survey developed through literature review, iterative content review, and pilot testing to collect data. (See Supplemental Digital Content 1, which displays survey questions, https://links.lww.com/PQ9/A740.) We selected content areas and 14 survey questions from a previously published national survey.^18^ Focus areas included hardware and software content, user interface, workflow and communication, organizational features, and responder characteristics. We created additional questions to assess perceived time spent, attitudes about TPAD as a safety issue, and prior training on result management. Because residents do not independently review TPAD results at our institution, we selected 13 questions from the hospitalist survey for a shortened resident survey. The survey questions were multiple choice, with most items scored on a 5-point Likert scale or a yes/no/unsure scale.
We administered the survey electronically and anonymously via REDCap, a Health Insurance Portability and Accountability Act–compliant software platform.^19,20^ The survey was beta-tested by the authors, pediatric chief residents, and PHM advanced practice providers for readability and clarity.
Outcomes and Analysis
We generated descriptive statistics to summarize responder characteristics and aggregate responses. We used Fisher’s exact test, with P values less than 0.05 considered significant, to determine differences between groups. This study was approved by our local review board (INOVA-2024-61).
RESULTS
A total of 50 physicians completed the survey: 23 hospitalists (81% response rate), 2 PHM fellows (100% response rate), and 25 resident physicians (68% response rate). We grouped the fellows with hospitalists to preserve anonymity. Forty-four percent (n = 11) of hospitalists reported more than 10 years since residency/fellowship, 32% (n = 8) reported 6–10 years, and 24% (n = 6) reported 1–5 years. (See table 1, Supplemental Digital Content 2, which demonstrates responder demographics and current practices, https://links.lww.com/PQ9/A741.) Of the 25 resident physicians, 7 (28%) were PGY-1, 11 (44%) were PGY-2, and 7 (28%) were PGY-3.
Forty-four percent (n = 11) of hospitalists reported missing results in the past year, whereas another 44% (n = 11) were unsure. Despite this, only 18% (n = 2) of those reporting missed results agreed that it led to a delay in patient care, whereas 36% (n = 4) were neutral and 46% (n = 5) disagreed (Fig. 1). Hospitalists who reported missing a test result in the past year, compared with those who did not or were unsure, were more likely to agree that there are too many alerts to easily focus on the most important ones (100%, n = 11, versus 57%, n = 8; P = 0.02) (Supplemental Digital Content 2, https://links.lww.com/PQ9/A741).
*Provider practices. P < 0.001.
Seventy-six percent (n = 19) of hospitalists and 60% (n = 15) of residents reported lacking the support needed to manage TPAD, and 72% (n = 18) of hospitalists and 20% (n = 5) of residents use manual cognitive reminders to follow up on results (Table 1). Of those hospitalists and residents who use at least 1 cognitive reminder (n = 23, 46%), the most frequently used cognitive reminder was manually putting the patient on a personal follow-up list within the electronic medical record (EMR) (65%, n = 15), followed by using a personal reminder in the EMR for notification of the result (26%, n = 6)—4 hospitalists (17%) used notes/to-do lists outside of the EMR as cognitive reminders.
There is ambiguity about who is responsible for managing TPAD, with only 12% (n = 3) of hospitalists and 8% (n = 2) of residents reporting that it is always or often clear who is responsible for following up on TPAD. Forty-eight percent (n = 12) of hospitalists agreed that they consistently notify patients or PCPs of abnormal results, whereas 32% (n = 8) neither agreed nor disagreed, and 20% (n = 5) disagreed or strongly disagreed. Among residents, 72% (n = 18) disagreed that they consistently notify patients or PCPs of abnormal results, whereas only 4% (n = 1) agreed. These differences between hospitalist and resident responses were statistically significant (P < 0.001) (Fig. 1; Supplemental Digital Content 2, https://links.lww.com/PQ9/A741).
Eighty percent (n = 20) of hospitalists and 80% (n = 20) of residents agreed or strongly agreed that the management of TPAD is a safety issue requiring a system solution. Eighty-eight percent (n = 22) of hospitalists and 96% (n = 24) of residents agreed with creating a standardized process for TPAD management. Additionally, 56% (n = 14) of hospitalists and 4% (n = 1) of residents had formal education in result management. Seventy-six percent (n = 19) of residents desire training (Fig. 2). (See table 2, Supplemental Digital Content 3, which demonstrates responder attitudes, perceptions, and preferences, https://links.lww.com/PQ9/A742.)
Attitudes, perceptions, and preferences.
DISCUSSION
This study of pediatric hospitalists and residents described current practices, the use of information technology tools, and attitudes and preferences regarding the management of TPAD. Overall, there is a widespread acknowledgement of TPAD as a patient safety issue. Similar to studies in the adult literature,^15,16^ our study found high levels of uncertainty regarding responsibility for managing TPAD, with only 12% of hospitalists and 8% of residents reporting that there is always or often clarity on who should follow up on results. Given such uncertainty, the variability among hospitalists we found in PCP and caregiver notification of abnormal test results is no surprise. Differences in notification between residents and hospitalists are likely due to residents’ limited experience with TPAD management. Variability in hospitalist notification practices aligns with prior studies showing vulnerability at transition points in care, such as hospital^21–24^ and emergency room discharge.^25^ This is especially true for health systems such as ours, where PCPs and specialists may not use the same EMR as the hospital.^10^
Many (72%) hospitalists reported relying on manual cognitive reminders, which may suggest that existing EMR tools are inadequate to support physicians in this process. Suboptimal use or design issues in the EMR can cause providers to miss results.^21–24^ High cognitive workloads can also lead to avoidance or cognitive dismissal of results.^26^ This is consistent with our study, where those who reported missing results, compared with those who did not or were unsure, were more likely to cite alert fatigue as a problem (100% versus 57%). These findings underscore the need for a process to reduce cognitive burden during TPAD management. Overall, both hospitalists (80%) and residents (80%) agreed that inpatient physicians require a system-based solution to manage TPAD.
Only 18% of hospitalists reported missing results during the past year, leading to care delays, compared with 83% of adult outpatient physicians who reported patient care delays during the past 2 months.^10^ This difference may stem from limited continuity of care, leading hospitalists to be unaware of delays in care. Limitations of our study include recall bias and other inaccuracies in self-reported data, as well as its single-institution design, which limits the generalizability of the results. The lower response rate by residents and the overall small number of providers limited our ability to analyze practices and perceptions by provider characteristics. Further research is needed to determine if results are similar across different PHM contexts.
To improve the safety of test result management within departments, we suggest using a quality improvement methodology with a SMART (Specific, Measurable, Achievable, Realistic, Time-based) aim to decrease the percentage of pediatric hospitalists who report missing a test result in the last year from 44% to 20% in 6 months (Fig. 3). Additional quality improvement measures of interest could include the frequency of diagnostic delays (outcome), turnaround time for result management (process), and provider satisfaction (balancing). Interventions should focus on reducing variability by clarifying responsibilities and establishing a standard workflow. Provider education and feedback have been shown to improve rates of result management.^27^ This education should focus on optimizing or creating new EMR result management tools, determining the urgency of a result, and expectations and methods for patient and other care team provider notification and documentation. Practices, especially those doing shift work, should also consider developing a process with shared responsibility, using interprofessional teams^28^ for postdischarge result management.
Driver diagram.
CONCLUSIONS
Pediatric hospitalists and residents are concerned about missing results after discharge and agree that a system-based solution is needed. We found considerable variability in current practices and a consistent desire for a standard TPAD management process. Next steps include a quality initiative and the development of a trainee curriculum to improve TPAD management.
Supplementary Material
**
**
**
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Alliance for Patient Safety. Summary of the evidence on patient safety: implications for research. 2008. World Health Organization. Available at https://iris.who.int/server/api/core/bitstreams/10c 19ae 7-2759-49b 0-a 6e 8-b 8f 30546 d 682/content. Accessed June 15, 2025.
- 2ECRI Institute. Top 10 patient safety concerns for healthcare organizations. 2017. Available at https://www.ecri.org/emailresources/psrq/top 10/2017_pstop 10_executivebrief.pdf. Accessed March 15, 2025.
- 3Were MC Li X Kesterson J. Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow-up providers. J Gen Intern Med. 2009;24:1002–1006.19575268 10.1007/s 11606-009-1057-y PMC 2726888 · doi ↗ · pubmed ↗
- 4Callen J Georgiou A Li J. The safety implications of missed test results for hospitalised patients: a systematic review. BMJ Qual Saf. 2011;20:194–199.10.1136/bmjqs.2010.044339 PMC 303810421300992 · doi ↗ · pubmed ↗
- 5Truijens K Frans G Vermeersch P. Critical results in laboratory medicine. Clin Chem. 2024;70:1220–1230.39245958 10.1093/clinchem/hvae 120 · doi ↗ · pubmed ↗
- 6Graber ML Franklin N Gordon R. Diagnostic error in internal medicine. Arch Intern Med. 2005;165:1493–1499.16009864 10.1001/archinte.165.13.1493 · doi ↗ · pubmed ↗
- 7Office of the National Coordinator for Health Information Technology, US Department of Health and Human Services. 21st century cures act: interoperability, information blocking, and the ONC health it certification program. Fed Regist. 2020;85:25642–25961.
- 8Steitz BD Turer RW Lin C. Perspectives of patients about immediate access to test results through an online patient portal. JAMA Netw Open. 2023;6:e 233572.36939703 10.1001/jamanetworkopen.2023.3572 PMC 10028486 · doi ↗ · pubmed ↗