Digital Health Literacy and Tool Adoption in Postoperative Care in a Safety-Net Hospital Population: Mixed Methods Study
Christopher Awad, Alexander Jakub Martinek, Chunhao Zou, Rosalind Byrd, Hui Jean Ooi, Kimberly Do, Henry Young, Bhavin Adhyaru, Muhammed Idris, Rosa I Arriaga

TL;DR
This study explores digital health literacy and tool adoption among postoperative patients in a safety-net hospital, finding that many are confident using digital tools for health, though confidence in decision-making lags.
Contribution
The study provides new insights into digital health literacy and tool adoption in underserved safety-net hospital populations using mixed methods.
Findings
69% of patients reported high confidence in finding health resources online.
Only 49% felt confident using digital resources for health decision-making.
Patients and providers rated a digital health prototype highly for ease of use and intuitiveness.
Abstract
Digital health tools are increasingly prevalent in postoperative care management, yet limited research exists on digital health literacy and tool adoption among safety-net hospital populations. Understanding these factors is crucial for developing effective digital health solutions for historically underserved communities. This study aimed to evaluate digital health literacy, assess technology adoption readiness, and examine the relationship between patient-reported capabilities and demographic factors in a postoperative care context at a safety-net hospital. We conducted a mixed methods study with 71 postoperative patients and 29 health care providers at a safety-net hospital. Participants completed a modified eHealth Literacy Scale (eHEALS) assessment and a demographic questionnaire, followed by usability testing of PocketDoc, a digital health prototype. The modified 7-item eHEALS…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
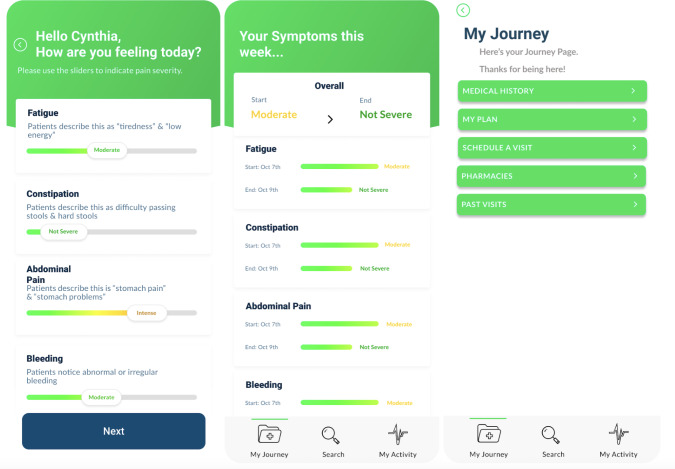 Figure 1
Figure 1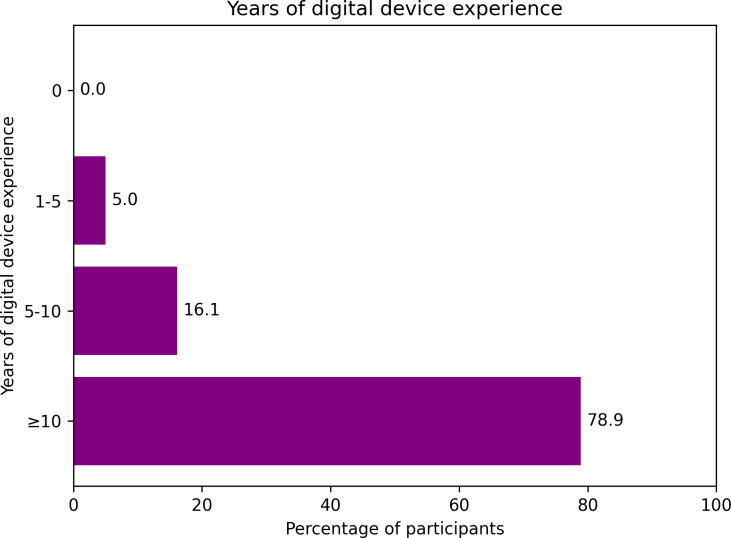 Figure 2
Figure 2| Characteristic and category | Participants, n (%) |
|---|---|
| Survey completion | |
| eHEALS | 71 (100) |
| PocketDoc postsurvey | 71 (100) |
| Time when surgery was conducted | |
| Within the previous month | 41 (57.7) |
| Within the previous 6 months | 19 (26.8) |
| Within the previous year | 10 (14.1) |
| Chronic conditions | |
| Yes | 41 (57.7) |
| No | 27 (38) |
| Number of chronic conditions (n=41) | |
| 1 | 23 (56.1) |
| 2 | 12 (29.3) |
| 3 | 6 (14.6) |
| Age group (y) | |
| 18-24 | 14 (19.7) |
| 25-34 | 19 (26.8) |
| 35-44 | 9 (12.7) |
| 45-54 | 7 (9.9) |
| 55-64 | 12 (16.9) |
| 65-74 | 7 (9.9) |
| 75-84 | 3 (4.2) |
| ≥85 | 0 (0) |
| eHEALS item | Score (1-5), median (IQR) |
|---|---|
| Evaluating resources | 3 (2-3) |
| Knowing how to find resources | 3 (2-3) |
| Using resources | 3 (2-3) |
| Knowing about the existence of resources | 3 (2-3.5) |
| Identifying the quality of resources | 3 (2-3.5) |
| Knowing where to find resources | 3 (2-4) |
| Making decisions with resources | 2 (2-3) |
| Usability metric | Survey item | Score (1-10), median (IQR) |
|---|---|---|
| Ease of use | “I think PocketDoc was easy to use.” | 10 (8-10) |
| Task scenario intuitiveness | “I think the Task Scenarios were intuitive to complete with PocketDoc.” | 10 (8-10) |
| Interface satisfaction | “I like the interface of PocketDoc.” | 9 (8-10) |
| Information findability | “I think my health information was presented to me in a way that was easy to find.” | 9 (7-10) |
| Information organization | “I think my health information was presented to me in a way that was well organized.” | 8 (7-10) |
| Compassionate wording | “I think my health information was presented to me in a way that was worded compassionately.” | 10 (9-10) |
| Information summary | “I think my health information was presented to me in a way that was useful for summary.” | 9 (7-10) |
| Health journey support | “I think PocketDoc would help me record my health journey after surgery.” | 9 (7-10) |
| Patient confidence | “I am confident in my ability to use PocketDoc (as demonstrated).” | 10 (9-10) |
| Item | eHEALS item wording |
|---|---|
| 1 | “I know what health resources are available on the Internet.” |
| 2 | “I know where to find helpful health resources on the Internet.” |
| 3 | “I know how to find helpful health resources on the Internet.” |
| 4 | “I know how to use the Internet to answer my questions about health.” |
| 6 | “I have the skills I need to evaluate the health resources I find on the Internet.” |
| 7 | “I can tell high-quality health resources from low-quality health resources on the Internet.” |
| 8 | “I feel confident in using information from the Internet to make health decisions.” |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Literacy and Information Accessibility · Mobile Health and mHealth Applications · Telemedicine and Telehealth Implementation
Introduction
Postoperative care increasingly relies on digital health tools to support patient recovery, manage symptoms, and facilitate physician-patient communication [12]. As health care systems transition toward digital solutions, understanding patients’ ability to effectively engage with these tools becomes crucial, particularly in safety-net hospital settings, where digital health literacy barriers may impact care delivery and outcomes [3]. Digital health literacy, defined as “the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem” [4], plays a vital role in the successful implementation of digital health tools [25].
There is evidence suggesting that digital tools are effective in improving disease outcomes and health literacy [6-9]. Mobile health apps in the postoperative period have been correlated with earlier discharge, reduction of in-person follow-ups [1011], promotion of rehabilitation [12], earlier detection of surgical complications [13], and improved communication between patients and health care professionals [1415]. Beyond these clinical benefits, postoperative monitoring apps have shown potential to empower patients, providing autonomy over their own health and potentially improving satisfaction and recovery motivation [16-18].
However, it remains unclear what factors make these digital tools superior to human health navigators or resources available through simple internet searches [19], particularly in postoperative settings [20]. Despite the proliferation of digital health tools in postoperative care [21], limited research exists on digital health literacy and technology adoption readiness among safety-net hospital populations [2223]. While studies demonstrate the efficacy of mobile apps in improving postoperative outcomes [24], these benefits presume a baseline level of digital health literacy that may not be universal across all patient populations, particularly in historically underserved communities [25].
In safety-net hospital settings, health literacy is shaped by factors such as educational level, language, and socioeconomic status, with lower health literacy levels linked to poorer health outcomes, reduced treatment adherence, and greater reliance on emergency care. Digital literacy, while related, is a distinct construct that poses additional barriers—particularly for older adults, non–English speakers, and individuals from lower socioeconomic backgrounds, who often face limited internet access and lack the digital skills necessary for navigating health care tools and systems. These separate constructs highlight a need for tailored tools to improve both forms of literacy [26].
The assumption that patients in safety-net hospitals face substantial barriers to digital health tool adoption has shaped both the development and implementation of digital interventions [23]. However, this assumption may not fully reflect current realities as smartphone ownership and digital technology use have become increasingly prevalent across socioeconomic groups [2728]. As digital health tools continue to expand in postoperative care, understanding the actual digital health literacy levels and technology adoption readiness of safety-net hospital patients is essential for designing effective and equitable solutions [29].
In this study, we distinguished between 2 related but distinct constructs. Digital health literacy refers to patients’ perceived ability to seek, evaluate, and apply online health information, whereas technology adoption readiness reflects patients’ ability and confidence to engage with a specific digital health tool. Differentiating these constructs is critical as baseline literacy does not necessarily translate into successful interaction with or adoption of digital interventions.
In this paper, we present PocketDoc, a digital health application designed to support postoperative patient care, and use its evaluation to examine digital health literacy and technology adoption readiness in a safety-net hospital setting. We pursued 2 interrelated objectives. The primary aim was to assess digital health literacy levels among postoperative patients and health care providers. The secondary aim was to evaluate the usability of PocketDoc to determine whether a user-centered digital tool could be accessible to populations traditionally considered vulnerable to the digital divide.
These objectives are intentionally linked. Baseline digital health literacy provides essential context for interpreting usability findings, whereas usability outcomes inform whether patients are likely to adopt and meaningfully engage with digital health resources. By examining both constructs through a mixed methods approach—combining a modified eHealth Literacy Scale (eHEALS) assessment [30] with usability testing of a digital health prototype—we aimed to challenge prevailing assumptions about digital health literacy barriers and identify opportunities for more effective postoperative digital health tool implementation.
Methods
Study Design and Setting
This research was conducted at a large safety-net hospital in a Southern US state. We used a mixed methods approach combining quantitative assessments of digital health literacy with a qualitative usability testing of a digital health prototype.
Study Population and Recruitment
Participants included 71 postoperative patients and 29 health care providers. Study inclusion criteria required participants to be adults (aged ≥18 years) who had had surgery within the previous year, were caretakers of someone who had had surgery in the previous year, or provided clinical care in the postsurgical period. Participants were not excluded based on health status, gender, race, or socioeconomic status, although patients with cognitive deficits or functional impairments preventing the use of digital devices were not recruited.
Digital Health Literacy Assessment
Participants completed a modified version of the eHEALS, a validated instrument for measuring individuals’ combined knowledge, comfort, and perceived skills regarding finding, evaluating, and applying online health information [30]. The modified eHEALS included 7 of the original 8 items using its standard 5-point Likert scale (1=“not at all confident”; 5=“completely confident”). One question from the original eHEALS instrument, “I know how to use the health information I find on the internet to help me,” was inadvertently omitted during survey implementation. The modified 7-item scale demonstrated adequate internal consistency among the 71 patient participants (Cronbach α=0.77). We proceeded with analysis of the collected data while acknowledging this limitation in our interpretation of the results. This assessment captured perceived digital health literacy and did not evaluate task-based interaction with a specific technology.
PocketDoc Development and Testing
PocketDoc (Figure 1) is a comprehensive digital health tool designed to support patients during the postoperative period, particularly in historically underserved populations. Key functionality includes symptom tracking, medication management with reminders, secure messaging for communication with health care providers, and educational resources tailored to specific procedures. The platform also includes appointment scheduling, follow-up management, and real-time tools for assessing symptom burden, all aimed at enhancing recovery and improving patient outcomes. These features were designed to accommodate varying levels of digital literacy, with particular attention to intuitive navigation and clear information presentation. The interface incorporated evidence-based design principles for health care applications [31], including consistent layout patterns, clear call to action elements, and simplified medical terminology. The development process included multiple rounds of iterative design and input from design professionals, business consultants, and historically underserved patients through multiple rounds of feedback.
Select screenshots of the introduction page and “My Journey” tab of PocketDoc.
For the usability testing and posttask surveys, responses were collected using a 10-point Likert scale (1=“strongly disagree”; 10=“strongly agree”) to obtain granular insights into participants’ experiences with the digital health prototype. Usability testing and posttask surveys were used to assess technology adoption readiness and perceived usability rather than digital health literacy.
Data Collection Procedures
Data collection occurred in 2 phases: the first phase included the demographic questionnaire, modified eHEALS assessment, and technology experience survey, and the second phase was the usability test, including standardized introductions to tasks, think-aloud protocols during task completion, and a posttask survey [32]. Sessions were conducted either in person or virtually via videoconference to accommodate participant availability, with each session lasting approximately 20 minutes.
Data Analysis
Survey results were analyzed using the Kruskal-Wallis H test to examine differences in digital health literacy and tool adoption across geographic categories. Post hoc Dunn-Bonferroni tests were conducted to examine rural-suburban and rural-urban comparisons in terms of digital health literacy. The Spearman rank-order correlation was used for associations between patient-reported capabilities and use of health resources, as well as relationships between technology experience and tool adoption. Descriptive statistics were calculated for demographic and survey data. Exploratory linear regression analyses were conducted to examine whether technology experience (≥10 years vs <10 years) and overall digital health literacy were associated with patient confidence in their ability to use PocketDoc.
Ethical Considerations
This research was approved by Emory University’s institutional review board in collaboration with a safety-net hospital in a southern US state (STUDY00004346). Written informed consent was obtained from all participants before taking part in the study. The informed consent process included a detailed explanation of study procedures, potential risks and benefits, the voluntary nature of participating, and the right to withdraw at any time. Participants were provided the opportunity to ask questions before providing consent. Participants received a US $20 gift card as compensation for their time. All data were deidentified before analysis.
Results
Participant Demographics
All 71 patients completed the modified eHEALS presurvey and subsequent assessments. Patient demographics are presented in Table 1. We found that there was diverse representation across age groups, with approximately half (n=33, 47%) between the ages of 18 and 34 years. Most participants came from urban (n=23, 32%) and suburban (n=43, 61%) environments, with limited rural representation (n=3, 4%). Most participants (n=41, 58%) had undergone surgery within the previous month, whereas 27% (n=19) had had surgery within the previous 6 months, and 14% (n=10) had had surgery within the previous year. Chronic conditions were reported by 58% (n=41) of the participants, indicating a population with ongoing health care needs. The patient sample was predominantly composed of Black individuals, reflecting the racial composition of the safety-net hospital population served.
Digital Health Literacy Levels
Analysis of the modified eHEALS survey (Table 2 and Multimedia Appendix 1) revealed that 69% (49/71) of patients reported high confidence (score of ≥3 on a 5-point scale) in finding health resources online (median 3, IQR 2-3). Furthermore, 61% (n=43) of participants expressed confidence in using the internet for health-related questions (median 3, IQR 2-3), and 63% (n=45) reported feeling capable of evaluating health resources (median 3, IQR 2-3). However, a notable drop occurred when examining confidence in health decision-making, with only 49% (n=35) feeling confident in using digital resources for making health decisions (median 2, IQR 2-3). Statistical analysis revealed that patients’ confidence in finding health resources was positively correlated with interface satisfaction (ρ=0.262, 95% CI 0.03‐0.47; P=.03). Similarly, patients’ confidence in using these resources showed a significant positive correlation with interface satisfaction (ρ=0.304, 95% CI 0.07‐0.52; P=.01).
Technology Experience and Demographic Correlations
Analysis of technology experience (Figure 2) revealed that 79% (56/71) of the participants reported 10 or more years of digital device experience, indicating substantial familiarity with technology within the study population. Statistical analysis demonstrated no significant correlation between digital literacy and age or educational level. However, geographic location emerged as a notable factor in digital literacy levels. The Kruskal-Wallis H test revealed significant differences in perceptions based on living environment (effect size=0.112; P=.05). Urban and suburban patients reported similarly high mean confidence scores (urban: mean 9/10, SD 1.33; suburban: mean 9/10, SD 1.19), whereas rural patients reported significantly lower scores (mean 7/10, SD 0.0). Post hoc Dunn-Bonferroni tests showed differences between rural-suburban (P=.081) and rural-urban comparisons (P=.080), which did not meet the significance threshold.
Years of digital device experience among postoperative patients (N=71).
Tool Adoption and Use Patterns
In the usability assessment of the digital health prototype (Tables34), participants demonstrated high levels of engagement and capability. Usability ratings across participants were high for ease of use (median 10, IQR 8-10), with task intuitiveness scoring highly at an average of 8.82 of 10 (median 10, IQR 8-10). Analysis revealed a significant correlation between prior technology exposure and perceived helpfulness of a digital health tool such as PocketDoc (ρ=0.230, 95% CI 0.01‐0.43; P=.04). Participants with ≥10 years of digital device experience showed particularly strong performance in information-finding tasks (median 9, IQR 7-10).
Interestingly, participants’ ability to distinguish high-quality health resources showed a significant negative correlation with ease of finding information (ρ=−0.251, 95% CI −0.46 to −0.02; P=.04), whereas the correlation with information organization perception was marginally significant (ρ=−0.215, 95% CI −0.42 to 0.01; P=.07).
In an exploratory regression analysis examining predictors of confidence in ability to use PocketDoc, the overall model was statistically significant (R^2^=0.15; P=.004). Higher digital health literacy was independently associated with lower usability confidence (β=−0.31, 95% CI −0.50 to −0.12; P=.002), whereas technology experience (≥10 years vs <10 years) was not independently associated after accounting for literacy (β=0.36, 95% CI −0.19 to 0.91; P=.20).
Discussion
Principal Findings
Digital health literacy and technology adoption in safety-net hospital populations present a more nuanced picture than traditionally assumed. Prior research has suggested that patients in safety-net settings face barriers to digital health tool adoption due to limited access, lower digital literacy, and poor health literacy [26]. Our findings challenge the universality of these assumptions while highlighting specific areas in which targeted support may still be necessary for effective postoperative digital health implementation.
Importantly, digital health literacy and technology adoption readiness represent related but distinct constructs. The eHEALS captures patients’ perceived ability to seek, evaluate, and apply online health information broadly, whereas usability findings reflect patients’ interaction with a specific digital health tool within a defined clinical context. Distinguishing these constructs is critical for interpreting how baseline capabilities translate into real-world technology use.
In this study, relatively high levels of self-reported digital competency were observed, with 69% (49/71) of participants reporting high confidence in finding health resources online. This suggests that basic digital literacy barriers may be less universal among safety-net hospital patients than previously assumed [26]. These findings align with broader trends of increasing smartphone ownership and digital technology use across socioeconomic groups [27]. The high prevalence of substantial technology experience (n=56, 79% reporting ≥10 years of device use) further supports this shift.
Assessing digital health literacy alongside prototype usability provided important contextual insights. The relatively high baseline confidence in finding online health information helps frame the strong usability ratings observed for PocketDoc, including high scores for ease of use and task intuitiveness (median 10, IQR 8-10 in both cases). Together, these findings suggest that user-centered design approaches may facilitate accessibility across varying levels of digital health literacy.
A more granular pattern emerged when examining specific domains of digital health literacy. While many participants felt confident evaluating health resources (45/71, 63%) and using the internet for health-related questions (43/71, 61%), fewer reported confidence in using digital information for health decision-making (35/71, 49%). This pattern is consistent with prior work demonstrating that digital health literacy comprises multiple competencies, with decision-making often representing the greatest challenge [4253334].
The gap between general digital competency and confidence in health decision-making mirrors findings from recent studies highlighting the complexity of translating basic digital skills into applied health management [3536]. This challenge may be particularly salient in postoperative care, where patients must interpret complex instructions and make time-sensitive decisions that carry immediate health implications [37].
Geographic differences in digital health literacy could not be robustly assessed due to the small rural sample size (n=3). Although rural participants demonstrated lower mean confidence scores than urban and suburban participants, these observations are exploratory and not suitable for inferential conclusions. Nonetheless, the observed pattern aligns with broader literature on rural-urban digital health disparities and underscores the need for future studies with adequately powered rural samples [3538].
An additional insight emerged from the relationship between digital health literacy and usability perceptions. The negative association between critical evaluation skills and satisfaction with information organization (ρ=−0.251; P=.04) reflects a paradox observed in prior digital health research [39-41]. More digitally literate users may hold higher expectations for information presentation and usability rather than experiencing reduced capability.
This interpretation is further supported by exploratory regression analyses, which suggested that higher digital health literacy was associated with lower confidence in usability. Together, these findings highlight a key design challenge: digital health tools must accommodate users with varying levels of sophistication and expectations. Adaptive interfaces that provide both simplified overviews and optional advanced features may be particularly well suited for postoperative care contexts.
While this study also collected rich qualitative data through interviews and extended usability observations, this manuscript focuses on quantitative analyses and usability themes. A forthcoming manuscript will explore qualitative findings in greater depth to further contextualize patient experiences and perspectives. This approach was chosen to maintain focus on the study’s primary quantitative and usability outcomes.
Limitations
Several limitations should be considered when interpreting these findings. Our use of a modified eHEALS, which inadvertently omitted question 5 (“I know how to use the health information I find on the internet to help me”), may have affected the comprehensiveness of our digital health literacy assessment. This modification constitutes use of a nonvalidated tool, and while the modified version demonstrated internal consistency (Cronbach α=0.77), this omission limits direct comparability with other eHEALS-based studies and potentially overestimates overall literacy levels.
Our sample included limited representation from rural areas (n=3), which precludes any meaningful conclusions about geographic disparities. Any observed differences between rural and both urban and suburban participants are reported as exploratory findings only and require replication in adequately powered samples. Relatedly, post hoc power for the geographic group comparison was low; thus, this study is underpowered to detect true rural–urban and suburban differences. This limitation is relevant given the differences we observed between both urban and suburban and rural participants.
This study’s reliance on self-reported measures of digital health literacy may not fully capture actual capabilities. While self-reported measures are widely used in digital health literacy research [42], they may be subject to social desirability bias and over- or underestimation of abilities. Our study may be subject to Berkson bias and self-selection bias as individuals with extremely low digital literacy or limited interest in digital tools may have been less likely to participate, and individuals with greater comfort with or interest in digital technologies may have been more likely to enroll.
Correlation analyses were exploratory and not adjusted for multiple testing, raising the possibility of type I error; therefore, the findings should be interpreted as hypothesis generating. Exploratory regression analyses were intentionally constrained to a small number of predictors due to sample size and ceiling effects in usability ratings and should not be interpreted as supporting causal inference.
Conclusions
This study advances our understanding of the evolving landscape of digital readiness among postoperative patients in safety-net settings. While participants reported substantial experience with digital devices, the data highlight a persistent challenge: translating general digital familiarity into confidence in managing personal health decisions. This gap suggests that, even when access and basic skills are present, patients may still struggle to apply digital tools meaningfully in complex clinical contexts such as postoperative care. Moreover, preliminary geographic trends point to location-based factors rather than traditional demographic variables as potential influences on confidence and engagement with digital health tools. These insights underscore the importance of designing tools that go beyond increasing access or general literacy, instead emphasizing support for decision-making and personalization based on patients’ lived environments. Addressing these nuanced barriers may be key to optimizing digital health strategies and ensuring equitable postoperative support across diverse care settings.
Supplementary material
10.2196/75496Multimedia Appendix 1Patient-reported digital health literacy scores by domain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang J Ge Y Yang M Ivers R Webster R Tian M The role of digital health for post-surgery care of older patients with hip fracture: a scoping review JMIR Preprints Preprint posted online on Jun 102021 doi 10.2196/preprints.3115735144101 · doi ↗ · pubmed ↗
- 2He M Chen M Ji Y Lu G Effectiveness of smartphone app-based interventions after surgery on quality of recovery among cancer patients: a systematic review and meta-analysis Ann Med Dec 20245612390167 doi 10.1080/07853890.2024.2390167 Medline 39140390 PMC 11328604 · doi ↗ · pubmed ↗
- 3Kemp E Trigg J Beatty L et al Health literacy, digital health literacy and the implementation of digital health technologies in cancer care: the need for a strategic approach Health Promot J Austr Feb 202132 Suppl 14104114 doi 10.1002/hpja.387Medline 32681656 · doi ↗ · pubmed ↗
- 4Conard S Best practices in digital health literacy Int J Cardiol Oct 12019292277279 doi 10.1016/j.ijcard.2019.05.070Medline 31230937 · doi ↗ · pubmed ↗
- 5Campanozzi LL Gibelli F Bailo P Nittari G Sirignano A Ricci G The role of digital literacy in achieving health equity in the third millennium society: a literature review Front Public Health Feb 202023111109323 doi 10.3389/fpubh.2023.1109323 Medline 36891330 PMC 9986277 · doi ↗ · pubmed ↗
- 6Guhl E Althouse AD Pusateri AM et al The atrial fibrillation health literacy information technology trial: pilot trial of a mobile health app for atrial fibrillation JMIR Cardio Sep 4202041 e 17162 doi 10.2196/17162 Medline 32886070 PMC 7501575 · doi ↗ · pubmed ↗
- 7Hendawi R Alian S Li J A smart mobile app to simplify medical documents and improve health literacy: system design and feasibility validation JMIR Form Res Apr 1202264 e 35069 doi 10.2196/35069 Medline 35363142 PMC 9015750 · doi ↗ · pubmed ↗
- 8Mc Kay FH Cheng C Wright A Shill J Stephens H Uccellini M Evaluating mobile phone applications for health behaviour change: a systematic review J Telemed Telecare 0120182412230 doi 10.1177/1357633 X 16673538 Medline 27760883 · doi ↗ · pubmed ↗