A Case Report of Acquired ALK Fusion in ALK Wild‐Type Lung Adenocarcinoma Following Chemotherapy and a Literature Review Is Presented
Wenqing Cheng, Ganling Qiao, Wenhua Zhang, Yifan Song, Xiangyi Zan

TL;DR
A patient with lung cancer initially negative for ALK fusion later developed it after chemotherapy, suggesting treatment may select for ALK-positive tumor cells.
Contribution
This case report presents a rare instance of acquired ALK fusion in lung adenocarcinoma following chemotherapy.
Findings
ALK fusion was detected after disease progression following chemotherapy in a patient initially ALK-negative.
Switching to ALK inhibitor alectinib led to a partial response, indicating the clinical relevance of repeat genetic testing.
Chemotherapy may exert selective pressure that enriches ALK fusion-positive tumor clones.
Abstract
ALK fusion is a key driver mutation in non‐small cell lung cancer, typically present as a primary genetic alteration. This article reports a rare case of a patient who was initially ALK‐negative but subsequently developed an ALK fusion following chemotherapy. A 52‐year‐old female was diagnosed with advanced lung adenocarcinoma. Initial genetic testing showed wild‐type EGFR and ALK. She received first‐line platinum‐based doublet chemotherapy combined with a VEGF inhibitor and a PD‐L1 inhibitor, achieving a partial response. Upon disease progression, repeat genetic testing unexpectedly detected an ALK fusion. Treatment was then switched to the ALK inhibitor alectinib, and the patient again achieved a partial response. This case suggests that chemotherapy may enrich ALK fusion‐positive tumour cell clones through selective pressure. These findings highlight the clinical importance of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
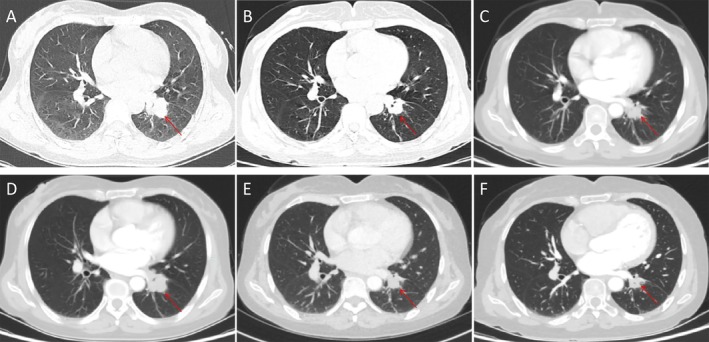 FIGURE 1
FIGURE 1- —Natural Science Foundation of Gansu Province10.13039/501100004775
- —Lanzhou University Second Hospital Cuiying Program
- —Gansu Provincial Drug Regulatory Science Research Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment · Lung Cancer Research Studies
Introduction
1
Lung cancer remains the leading cause of cancer‐related mortality worldwide, with non‐small cell lung cancer (NSCLC) accounting for approximately 85% of cases. The treatment of advanced NSCLC has evolved from conventional chemotherapy to driver gene‐based individualised targeted therapy. Agents directed against various targets such as EGFR and ALK have become first‐line standard regimens, significantly prolonging patient survival and transitioning lung cancer into an era of chronic disease management [1]. ALK fusion is identified in approximately 3%–7% of NSCLC cases, representing a relatively uncommon driver alteration. In contrast to EGFR mutations, ALK fusions are more frequently observed in younger patients (typically under 55 years of age), never‐ or light‐smokers with adenocarcinoma, particularly those containing signet‐ring cell components [2]. Although the vast majority of ALK fusions are primary events, acquired ALK fusions are exceedingly rare. They have been occasionally reported following resistance to EGFR‐TKIs [3], but cases reported after chemotherapy are even more uncommon. This report presents a rare case of ALK fusion emerging after chemotherapy and discusses its potential mechanisms and clinical implications.
Case Report
2
A 52‐year‐old non‐smoking female presented in March 2022 with a six‐month history of cough, expectoration, and left‐sided chest and back pain. Imaging studies identified a 2.2 × 1.8 cm mass in the left lower lung lobe (Figure 1A) accompanied by enlarged hilar and mediastinal lymph nodes, bilateral adnexal masses and multiple systemic bone metastases. Bronchoscopic biopsy of a lesion in the left lower lobe (specimen diameter: 0.4 cm) confirmed the diagnosis of lung adenocarcinoma. Immunohistochemical staining showed positivity for CKpt^+^, TTF‐1^+^, and CK7^+^, weak positivity for NapsinA, and negativity for CK5/6^−^, p40^−^, Syn^−^ and CgA^−^. CD56 showed focal positivity, and the Ki‐67 index was approximately 15%. Genetic testing revealed wild‐type EGFR and no ALK fusion. The patient was diagnosed with left lung adenocarcinoma (stage cT1bN3M1c IVB). The patient began treatment in April 2022 with eight cycles of pemetrexed, cisplatin and bevacizumab. In March 2023, the treatment regimen was changed to three cycles of liposomal paclitaxel, cisplatin, bevacizumab and pembrolizumab, resulting in a partial response (Figure 1B,C). This was followed by six cycles of maintenance therapy with bevacizumab and pembrolizumab. Three months after treatment discontinuation, a follow‐up examination showed an increase in lesion size to 2.3 × 2.6 cm (Figure 1D), indicating disease progression (PD). Repeat biopsy and genetic testing revealed an ALK fusion. The patient was started on alectinib (600 mg twice daily). After 2 months of targeted therapy, re‐evaluation showed a reduction in lesion size to 2.0 × 1.6 cm (Figure 1E), again assessed as PR. The patient has now been on alectinib for 14 months. Recent imaging demonstrates further shrinkage of the lesion to 1.5 × 1.2 cm (Figure 1F), as well as improvement in bone metastases and adnexal lesions.
(A) Initial diagnosis of lung adenocarcinoma; (B) After 3 months of chemotherapy; (C) After 1 year of chemotherapy; (D) Disease progression; (E) After 2 months of targeted therapy following progression; (F) After 1 year of targeted therapy following progression.
All ALK testing (both at baseline and upon progression) in this study was performed in the Department of Pathology of Lanzhou University Second Hospital. The widely validated Ventana ALK (D5F3) CDx Assay immunohistochemistry (IHC) method was uniformly applied. Staining was interpreted by an experienced pathologist in strict accordance with CAP/AMP guidelines, with positivity defined as strong, complete membranous staining in ≥ 1% of tumour cells. Previous studies have confirmed that this detection system has a sensitivity of > 95% for ALK rearrangements in lung adenocarcinoma [4]. The use of the same IHC platform, reagents and interpretation criteria for both baseline and follow‐up testing ensured methodological consistency.
Discussion
3
This case report describes a patient with advanced lung adenocarcinoma who, following progression on platinum‐based chemotherapy and immunotherapy, was found to have an acquired ALK fusion during secondary genetic testing and ultimately benefited from ALK‐TKI therapy. This case provides important insights into understanding tumour resistance mechanisms and clinical decision‐making.
ALK fusions are typically considered primary drivers in NSCLC [2]. In this case, initial ALK testing was negative, yet an ALK fusion was newly detected after chemotherapy. Such ‘acquired’ rearrangements are extremely rare. Existing reports indicate that acquired ALK fusions predominantly emerge after EGFR‐TKI resistance, often via bypass activation mechanisms [3]. This case suggests that conventional chemotherapy can also exert powerful evolutionary pressure, driving tumour genomic rearrangements.
Regarding the mechanism, we favour the clonal selection hypothesis [5]. This suggests that a small subclone carrying the ALK fusion, inherently resistant to chemotherapy, may have existed in the initial tumour but remained undetected due to its abundance falling below the detection limit. Platinum‐based chemotherapy eliminated the dominant sensitive clones, creating space for this resistant clone to expand and ultimately become the predominant population. Another possibility—chemotherapy directly inducing genomic instability leading to ALK rearrangement [5]—remains theoretically plausible but lacks evidence and is considered less likely.
The core clinical value of this case lies in confirming the necessity of repeated genetic testing during disease progression. Regardless of prior treatment regimens, once disease progresses, re‐biopsy should be performed to identify new targetable mechanisms, which is crucial for securing precision treatment opportunities for patients. Upon detection of acquired ALK fusions, immediate conversion to ALK‐TKI targeted therapy is warranted. This patient achieved rapid partial remission after alectinib treatment, fully demonstrating the exceptional efficacy of late‐line precision targeted therapy.
This study also has several limitations. First, as a single‐case report, it cannot estimate the overall incidence of such acquired ALK fusions. Second, due to the limited baseline biopsy specimen (small volume), we were unable to retrospectively perform ultra‐deep sequencing to verify whether low‐abundance ALK‐fusion clones existed in the initial tissue. Thus, direct molecular evidence supporting the clonal selection hypothesis remains unavailable. Third, the small baseline biopsy itself carries a risk of false‐negative ALK IHC results due to tumour heterogeneity and sampling bias. Given these specimen‐ and evidence‐related constraints, the exact causal relationship between chemotherapy and the detection of the ALK fusion remains unclear. The previously mentioned notion that ‘chemotherapy might induce gene rearrangement’ remains only a mechanistic hypothesis; an explanation more consistent with current tumour evolution theory is that chemotherapy exerted clonal selection pressure, promoting the expansion of pre‐existing ALK‐fusion‐positive subclones into the dominant population. The causal relationship between chemotherapy and the emergence of the ALK fusion requires validation in future prospective studies using paired pre‐ and post‐treatment specimens and deep‐sequencing technologies.
Author Contributions
Wenqing Cheng: data curation, investigation, writing – original draft. Ganling Qiao, Wenhua Zhang, Yifan Song: investigation, visualisation, writing – review and editing. Xiangyi Zan: conceptualisation, supervision, project administration, writing – review and editing.
Funding
This work was supported by the Natural Science Foundation of Gansu Province (22JR5RA993), Lanzhou University Second Hospital Cuiying Program (CY2023‐MS‐B11), Gansu Provincial Drug Regulatory Science Research Project (2023GSMPA019).
Consent
The authors declare that written informed consent was obtained for the publication of this manuscript and accompanying images using the consent form provided by the Journal.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1F. Bray , M. Laversanne , H. Sung , et al., “Global Cancer Statistics 2022: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA: A Cancer Journal for Clinicians 74, no. 3 (2024): 229–263.38572751 10.3322/caac.21834 · doi ↗ · pubmed ↗
- 2M. Soda , Y. L. Choi , M. Enomoto , et al., “Identification of the Transforming Eml 4‐Alk Fusion Gene in Non‐Small‐Cell Lung Cancer,” Nature 448, no. 7153 (2007): 561–566.17625570 10.1038/nature 05945 · doi ↗ · pubmed ↗
- 3L. S. Wang , S. Q. Chen , X. Zhong , et al., “Acquired Eml 4‐Alk Fusion and Egfr C 797s in Cis Mutation as Resistance Mechanisms to Osimertinib in a Non‐Small Cell Lung Cancer Patient With Egfr L 858r/T 790m,” Anti‐Cancer Drugs 34, no. 10 (2023): 1146–1150.36728908 10.1097/CAD.0000000000001489 · doi ↗ · pubmed ↗
- 4K. F. To , J. H. Tong , K. S. Yeung , et al., “Detection of ALK Rearrangement by Immunohistochemistry in Lung Adenocarcinoma and the Identification of a Novel EML 4‐ALK Variant,” Journal of Thoracic Oncology 8, no. 7 (2013): 883–891.23625156 10.1097/JTO.0b 013e 3182904 e 22 · doi ↗ · pubmed ↗
- 5N. Mc Granahan and C. Swanton , “Clonal Heterogeneity and Tumor Evolution: Past, Present, and the Future,” Cell 168, no. 4 (2017): 613–628.28187284 10.1016/j.cell.2017.01.018 · doi ↗ · pubmed ↗