Distribution and Drug‐Resistance Analysis of Uropathogens in Urinary Tract Infections
Weiyi Wu, Qiong Wu, Wenying Zhong, Lizhong Han

TL;DR
This study analyzed UTI-causing bacteria in Shanghai and found high drug resistance, especially to common antibiotics.
Contribution
The study provides up-to-date regional data on uropathogen distribution and resistance patterns in Shanghai, China.
Findings
Escherichia coli was the most common UTI pathogen, with high resistance to ampicillin, levofloxacin, and cefazolin.
Klebsiella pneumoniae showed the highest resistance to ampicillin (97.3%) and levofloxacin (45.1%).
Female sex, age >60 years, and hospitalization were significant risk factors for UTIs.
Abstract
Urinary tract infections (UTIs) are a major global health concern with increasing antimicrobial resistance. Regional data on pathogen distribution and resistance patterns are essential for guiding empirical therapy. This study aimed to investigate the distribution and antimicrobial resistance profiles of UTI pathogens in Shanghai, China, and identify risk factors associated with UTIs. A retrospective analysis was conducted on urine culture records from 61,450 patients suspected of UTIs, collected between January 1 and December 31, 2023, from two general hospitals in Shanghai. Pathogen identification and antimicrobial susceptibility testing were performed according to CLSI guidelines (2021). Multivariable logistic regression was used to analyze risk factors for UTIs. Among 5671 confirmed UTI cases, Escherichia coli was the predominant pathogen (36.1%), followed by Enterococcus faecalis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
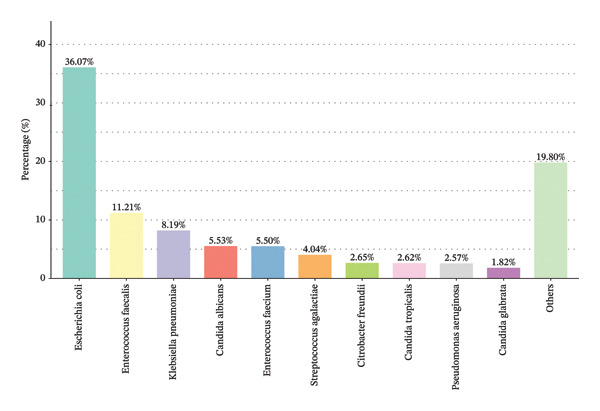 FIGURE 1
FIGURE 1| Characteristics |
|
|---|---|
|
| 61,450 (100.0) |
| Sex | |
| Male | 29,910 (51.3) |
| Female | 31,540 (48.7) |
| Age | |
| ≤ 60 years old | 22,675 (36.9) |
| > 60 years old | 38,775 (63.1) |
| Patient source | |
| Outpatient service | 11,614 (18.9) |
| Hospitalized | 49,836 (81.1) |
| Hospital | |
| A | 44,991 (73.2) |
| B | 16,459 (26.8) |
| Department | |
| Internal Medicine | 17,329 (28.2) |
| Surgery department | 28,144 (45.8) |
| Gynecology department | 12,843 (20.6) |
| Pediatric department | 3318 (5.4) |
| Urinary tract infection (UTI) | |
| Positive | 5671 (9.2) |
| Negative | 55,779 (90.8) |
| Drug‐resistant bacteria |
|
|
|
|---|---|---|---|
| Ampicillin | 1578 (75.9) | 459 (97.3) | 102 (66.7) |
| Cefazolin | 1021 (49.1) | 261 (55.3) | 92 (60.1) |
| Cefuroxime | 894 (43.0) | 230 (48.7) | 68 (44.4) |
| Ceftazidime | 393 (18.9) | 207 (43.9) | 13 (8.5) |
| Ceftriaxone | 896 (43.1) | 235 (49.7) | 53 (34.6) |
| Aztreonam | 516 (24.8) | 205 (43.5) | 30 (19.6) |
| Imipenem | 21 (1.0) | 117 (24.8) | Intrinsically resistant |
| Compound sulfamethoxazole | 877 (42.2) | 191 (40.4) | 81 (52.9) |
| Cefepime | 568 (27.3) | 172 (36.4) | 14 (9.2) |
| Meropenem | 21 (1.0) | 118 (24.9) | 2 (1.3) |
| Fosfomycin | 175 (8.4) | 148 (31.4) | 53 (34.6) |
| Ampicillin/sulbactam | 516 (24.8) | 234 (49.6) | 62 (40.5) |
| Colistin | 25 (1.2) | 21 (4.4) | Intrinsically resistant |
| Levofloxacin | 1231 (59.2) | 213 (45.1) | 62 (40.5) |
| Piperacillin/tazobactam | 264 (12.7) | 118 (24.9) | 3 (2.0) |
| Tigecycline | 6 (0.3) | 38 (8.1) | 0 (0) |
| Cefoperazone/sulbactam | 102 (4.9) | 148 (31.4) | 3 (2.0) |
| Ceftazidime/avibactam | 29 (1.4) | 16 (3.4) | 4 (2.6) |
| Characteristics | OR | 95% CI |
|
|---|---|---|---|
| Sex | |||
| Male | — | — | — |
| Female | 1.549 | 1.254, 1.887 | 0.003∗ |
| Age | |||
| ≤ 60 years old | — | — | — |
| > 60 years old | 2.598 | 2.075, 2.994 | < 0.001∗ |
| Patient source | |||
| Outpatient service | — | — | — |
| Hospitalized | 2.487 | 1.954, 2.954 | < 0.001∗ |
| Hospital | |||
| A | —. | — | — |
| B | 1.214 | 1.027, 1.459 | 0.028∗ |
| Department | |||
| Internal Medicine | — | — | — |
| Surgery department | 1.894 | 0.572, 2.458 | 0.384 |
| Gynecology department | 0.785 | 0.438, 1.157 | 0.578 |
| Pediatric department | 1.571 | 0.965, 2.001 | 0.684 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Pediatric Urology and Nephrology Studies · Reproductive tract infections research
1. Introduction
Urinary tract infections (UTIs) are among the most common infectious diseases worldwide. Epidemiological studies suggest that approximately 40% of women and 12% of men experience at least one symptomatic UTI in their lifetime. Moreover, 11% of women over the age of 18 develop a UTI each year, and nearly 27%–48% of women suffer from recurrent UTIs [1, 2], which pose substantial clinical challenges. Globally, UTIs affect approximately 150 million individuals annually [3]. International data indicate that over the past few decades, the global incidence, mortality, and disability‐adjusted life years (DALYs) associated with UTIs have continued to rise, establishing UTIs as a pressing public health issue worldwide [4]. The increasing incidence of UTIs prolongs hospital stays and imposes a significant economic burden. In 2011 alone, the total healthcare cost attributable to UTIs in the United States exceeded $2.8 billion [5].
UTIs can be classified in several ways, most commonly as uncomplicated or complicated. Uncomplicated UTIs occur in individuals without structural or neurological urinary tract abnormalities, whereas complicated UTIs are associated with factors such as functional or anatomical anomalies, urinary retention, obstruction, renal transplantation, pregnancy, immunosuppression, indwelling catheters, or calculi [6]. Based on the site of infection, UTIs may also be categorized as upper (e.g., renal pyelonephritis) or lower (e.g., cystitis and urethritis). Lower UTIs typically present with symptoms such as urinary frequency, urgency, and dysuria, while upper UTIs may additionally manifest with chills, fever, flank pain, and potential systemic complications including bacteremia, sepsis, and in severe cases, chronic renal failure or life‐threatening conditions [7]. Notably, the 2024 guidelines issued by the European Association of Urology (EAU) recommend classifying UTIs caused by multidrug‐resistant organisms or occurring in special populations (e.g., males and pregnant individuals) as complicated UTIs [8], a distinction that carries important implications for antimicrobial therapy selection.
Antibiotic therapy remains the cornerstone of UTI management. To achieve effective and personalized treatment, the choice of antimicrobial agents should be guided by several factors, including local antibiotic resistance patterns, the type of infection (community‐acquired vs. healthcare‐associated), and patient‐specific characteristics such as age, sex, previous antibiotic exposure, history of UTIs, and anatomical site of infection [9]. Although urine culture and antimicrobial susceptibility testing represent the gold standard for UTI diagnosis [10], providing accurate pathogen identification and resistance profiles, these results typically require 48–72 h. Consequently, clinicians often initiate empirical broad‐spectrum antibiotic therapy while awaiting laboratory findings. While this approach may alleviate symptoms temporarily, it carries risks such as therapeutic failure and the emergence of resistant strains, which may complicate treatment and exacerbate patient outcomes [11]. Thus, although empirical antibiotic use is widespread, it must be applied judiciously. Inappropriate antibiotic selection may not only lead to treatment failure but also create a reservoir of persistent pathogens within the urinary tract, fostering recurrence and adversely affecting long‐term prognosis. In the current climate of escalating antimicrobial resistance, prompt and accurate pathogen identification followed by tailored therapeutic strategies is essential for improving outcomes in UTI management.
Common uropathogens include Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, and Enterococcus species. Their antibiotic susceptibility profiles vary considerably. Although E. coli, K. pneumoniae, and P. mirabilis are all Gram‐negative bacilli, they exhibit distinct resistance patterns [12]. Furthermore, pathogens such as Enterococcus spp. and fungi require entirely different therapeutic approaches compared to Gram‐negative bacteria, further complicating clinical decision‐making. Reliance on broad‐spectrum antibiotics is increasingly problematic, as it may exacerbate resistance and reduce treatment efficacy. Achieving precision therapy while minimizing unnecessary antibiotic use has thus become an urgent priority in clinical practice. The distribution of uropathogens, their resistance patterns, and epidemiological characteristics vary significantly across regions and patient populations [13]. Although current guidelines emphasize the importance of regularly updated local antibiogram data to inform empirical treatment [14], recent in‐depth studies on UTIs in our region remain scarce. When assessing the spectrum of uropathogens, the potential involvement of commensal skin bacteria like Staphylococcus epidermidis and Corynebacterium species must be acknowledged, as they can act as causative agents of UTIs, particularly in healthcare settings or in individuals with underlying risk factors [15].
Therefore, this study aims to investigate the distribution and antimicrobial resistance profiles of UTI pathogens in our local population and to further examine the influence of factors such as sex, age, and infection setting (community vs. hospital) on pathogen prevalence and resistance patterns. We hope that our findings will provide a robust evidence base to guide clinical decision‐making, optimize empirical antibiotic therapy, facilitate early detection of infection trends across subgroups, support precision treatment approaches, mitigate the emergence of resistance due to antibiotic overuse, and ultimately improve therapeutic outcomes while reducing unnecessary healthcare costs.
2. Methods
2.1. Materials and Data
Urine culture records between January 1, 2023, and December 31, 2023, were extracted from the Laboratory Information System (LIS) of two general hospitals (A and B) in Shanghai, China. Urine samples were primarily collected using the clean‐catch midstream method from noncatheterized outpatients and ward patients. For catheterized patients, samples were aseptically collected from the catheter port. Duplicate bacterial strains isolated from the same site of the same patient were excluded. The criteria for a positive urine culture were established in accordance with the Clinical and Laboratory Standards Institute (CLSI) guidelines, 2021 edition: for Gram‐negative bacilli, a colony count greater than 10^5^ CFU/mL was considered positive; for Gram‐positive cocci and fungi, the threshold was set at greater than 10^4^ CFU/mL. This retrospective study was approved by the Ethics Committee of Shanghai Sixth People’s Hospital (Approval No. 2024‐KY‐051K).
2.2. Quality Control
To ensure the reliability and accuracy of this study, stringent quality control measures were implemented throughout the methodological process. Standardized protocols were strictly followed during sample collection, processing, and analysis. All laboratory procedures, including microbial culture and identification, were conducted in accordance with guidelines from the CLSI. Data extraction and entry were performed independently by two researchers to minimize errors, with consistency checks applied to resolve discrepancies. Statistical analyses were carried out using validated methods in SPSS, with appropriate tests selected based on data characteristics. Additionally, calibration of equipment and use of control strains were employed to maintain analytical precision. All steps were documented to ensure reproducibility and transparency of the research.
2.3. Statistical Analysis
Statistical analysis was performed using SPSS software (version 26). Categorical variables were compared using the Chi‐square (χ ^2^) test, while continuous variables were analyzed with the Student’s t‐test. A two‐tailed p value of less than 0.05 was considered indicative of statistical significance. To further explore factors influencing the outcomes, multivariate logistic regression analyses were conducted. Results were expressed as odds ratios (OR) with corresponding 95% confidence intervals (CI). Model fit was assessed using the Hosmer–Lemeshow test, and multicollinearity among variables was evaluated via variance inflation factors (VIF), with a VIF > 10 indicating significant collinearity.
3. Results
3.1. The Characteristics of Participants
A total of 61,450 participants with suspected UTIs were included in this study. The general characteristics of the study population are summarized in Table 1. Among them, 51.3% were male and 48.7% were female. The majority of participants (63.1%) were over 60 years of age. Most cases (81.1%) were from hospitalized patients, while 18.9% were from outpatient services. The study involved two hospitals, with 73.2% of samples originating from Hospital A and 26.8% from Hospital B. Department‐wise, the highest number of cases came from the Surgery department (45.8%), followed by Internal Medicine (28.2%), Gynecology (20.6%), and Pediatrics (5.4%). UTI was confirmed in 9.2% of cases (n = 5671).
3.2. The Distribution of Pathogenic Bacteria
The distribution of pathogenic bacteria isolated from urine cultures is summarized in Figure 1. Escherichia coli was the most predominant pathogen, accounting for 36.07% of the isolates (n = 2079). This was followed by Enterococcus faecalis (11.21%, n = 646) and Klebsiella pneumoniae (8.19%, n = 472). Candida albicans represented 5.53% (n = 319), while Enterococcus faecium constituted 5.5% (n = 317). Other notable pathogens included Streptococcus agalactiae (4.04%, n = 233), Citrobacter freundii (2.65%, n = 153), Candida tropicalis (2.62%, n = 151), Pseudomonas aeruginosa (2.57%, n = 148), and Candida glabrata (1.82%, n = 105). Together, these data summarize the key pathogenic agents observed and their relative prevalence in the analyzed samples.
Pathogenic bacteria types and distribution map.
3.3. The Distribution of Drug‐Resistant Bacteria
Table 2 details the antimicrobial resistance profiles of the three predominant uropathogens identified in this study: Escherichia coli (n = 2079), Klebsiella pneumoniae (n = 472), and Proteus mirabilis (n = 153). Escherichia coli demonstrated notably high resistance rates to ampicillin (75.9%), levofloxacin (59.2%), and cefazolin (49.1%), with moderate resistance observed against ceftriaxone (43.1%), cefuroxime (43.0%), and compound sulfamethoxazole (42.2%). Resistance to extended‐spectrum cephalosporins such as ceftazidime and cefepime was 18.9% and 27.3%, respectively, while resistance to carbapenems remained low (imipenem 1.0% and meropenem 1.0%). Additionally, resistance to ampicillin/sulbactam was 24.8% and to piperacillin/tazobactam was 12.7%. Klebsiella pneumoniae exhibited higher overall resistance, with the highest rates observed for ampicillin (97.3%) and cefuroxime (48.7%), ceftazidime (48.7%), ceftriaxone (43.9%), aztreonam (43.5%), and Levofloxacin (45.1%), along with 55.3% resistance to cefazolin and 48.7%% to cefuroxime. The two most clinically relevant enterococcal species, Enterococcus faecalis and Enterococcus faecium, exhibit divergent antimicrobial resistance profiles. E. faecium exhibited consistently higher resistance rates across most antibiotic classes. Notably, resistance to penicillin and ampicillin was exceedingly high in E. faecium (91.6% and 96.5%, respectively), compared to E. faecalis (16.5% and 6.3%). A similar, profound disparity was observed for ciprofloxacin (97.8% vs. 40.8%) and nitrofurantoin (62.6% vs. 2.3%). Resistance to levofloxacin was also significantly more common in E. faecium (79.9% vs. 42.1%). Conversely, E. faecalis showed a significantly higher rate of resistance to tetracycline (77.4% vs. 35.9%). Resistance to the glycopeptide vancomycin was low in both groups but remained statistically higher in E. faecium (2.5% vs. 0.6%). Resistance to high‐level gentamicin was comparable between the two species (44.0% vs. 42.9%). No resistance to tigecycline was detected in E. faecalis, while a low rate (0.9%) was observed in E. faecium.
3.4. The Multivariable Logistic Regression Analysis Factors of UTI
Multivariable logistic regression analysis factors associated with UTI risk is shown in Table 3. Female sex (OR = 1.55, 95% CI: 1.25–1.89, p = 0.003), age > 60 years (OR = 2.60, 95% CI: 2.08–2.99, p < 0.001), hospitalization (OR = 2.49, 95% CI: 1.95–2.95, p < 0.001), and receiving care at Hospital B (OR = 1.21, 95% CI: 1.03–1.46, p = 0.028) were identified as significant risk factors for UTI. No significant associations were found between hospital department and UTI risk.
4. Discussion
This study provides a comprehensive analysis of the distribution and antimicrobial resistance profiles of major uropathogens isolated from a large cohort of patients in Shanghai, China. Our findings reveal that Escherichia coli remains the predominant pathogen in UTIs, accounting for 36.1% of positive cultures, followed by Enterococcus faecalis (11.2%) and Klebsiella pneumoniae (8.2%). These results were consistent with global epidemiological reports indicating that E. coli is the most common cause of both community‐acquired and healthcare‐associated UTIs [16]. However, the high prevalence of Enterococcus spp. and Candida spp. observed in our study may reflect local epidemiological characteristics or the influence of a predominantly hospitalized and elderly population.
A key finding of this study was the high prevalence of antimicrobial resistance among common uropathogens. Escherichia coli exhibited alarmingly high resistance rates to commonly prescribed antibiotics such as ampicillin (75.9%), levofloxacin (59.2%), and cefazolin (49.1%). These rates are considerably higher than those reported in recent studies from North America and Europe [17, 18], highlighting significant regional variations in resistance patterns. The low resistance to carbapenems (1.0% for both imipenem and meropenem) is reassuring and suggests that these agents remain effective for treating multidrug‐resistant infections in our setting. Nevertheless, the high resistance to fluoroquinolones and third‐generation cephalosporins underscores the urgent need to reconsider their empirical use in UTIs.
Klebsiella pneumoniae isolates showed relatively higher resistance rates compared to E. coli, with the highest was observed for ampicillin (97.3%) and levofloxacin (45.1%). The very highcarbapenem resistance (24.9%) is consistent with reports from other Chinese studies [19] and supports the retention of carbapenems as a therapeutic option for serious K. pneumoniae infections. Proteus spp. demonstrated high resistance to ampicillin (66.7%) and cefazolin (60.1%), which is consistent with their intrinsic resistance mechanisms [20]. Notably, the high fosfomycin resistance (34.6%) in Proteus spp. is concerning, as this drug is often considered a therapeutic alternative for multidrug‐resistant UTIs [21]. An unexpected finding was the 16.1% susceptibility rate of K. pneumoniae to ampicillin, contrary to its well‐documented intrinsic resistance. This discrepancy may be attributed to rare susceptible strains or, more likely, to technical or interpretive nuances in the automated susceptibility testing system used. This result should be interpreted with caution, and ampicillin remains an unsuitable choice for empirical treatment of Klebsiella infections.
Multivariable analysis identified several factors significantly associated with UTI risk, including female sex, advanced age (> 60 years), hospitalization, and care at Hospital B. These findings align with established literature indicating that female gender, older age, and healthcare exposure are major risk factors for UTIs [22, 23]. The increased risk associated with hospitalization may be attributed to greater exposure to multidrug‐resistant organisms, invasive procedures, and underlying comorbidities [24]. The variation in UTI risk between hospitals may reflect differences in patient populations, infection control practices, or local prescribing behaviors, warranting further investigation [25, 26].
The high overall resistance burden, particularly among E. coli isolates (84.5%), underscores the growing challenge of antimicrobial resistance in UTIs. These findings emphasize the importance of ongoing surveillance and antimicrobial stewardship programs to guide empirical therapy and prevent further emergence of resistance [27]. The significant proportion of infections caused by non‐E. coli pathogens, including enterococci and fungi, also highlights the need for broader differential diagnoses and individualized treatment approaches, especially in hospitalized and elderly patients [28–30].
Several limitations should be considered when interpreting the results of this study. First, as a retrospective analysis, certain data were unavailable, which may have restricted the depth of our analysis. Moreover, the findings may not be fully generalizable to other hospital settings due to the specific context of the study. Finally, future prospective studies are needed to validate these findings and explore temporal trends in resistance patterns.
In conclusion, this study highlights the high prevalence of antimicrobial resistance among uropathogens in Shanghai, China, and identifies key risk factors for UTIs. Our findings underscore the need for region‐specific antibiotic guidelines and enhanced stewardship efforts to optimize empirical therapy and mitigate the spread of resistance.
Author Contributions
Conceptualization: Weiyi Wu and Lizhong Han.
Data curation: Weiyi Wu.
Formal analysis: Weiyi Wu.
Investigation: Weiyi Wu.
Methodology: Weiyi Wu.
Project administration: Wenying Zhong.
Resource: Weiyi Wu and Lizhong Han.
Software: Qiong Wu.
Supervision: Qiong Wu.
Validation: Qiong Wu.
Visualization: Wenying Zhong.
Writing–original draft: Weiyi Wu and Lizhong Han.
Writing–review and editing: Weiyi Wu and Lizhong Han.
Funding
There is no specific funding received for this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting Information
Table S1. Distribution of pathogens among outpatient and inpatient patients.
Supporting information
Supporting Information Additional supporting information can be found online in the Supporting Information section.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brumbaugh A. R. , Smith S. N. , and Mobley H. L. T. , Immunization With the Yersiniabactin Receptor, Fyu A, Protects Against Pyelonephritis in a Murine Model of Urinary Tract Infection, Infection and Immunity. (2013) 81, no. 9, 3309–3316, 10.1128/iai.00470-13, 2-s 2.0-84884264246.23798537 PMC 3754202 · doi ↗ · pubmed ↗
- 2Micali S. , Isgro G. , Bianchi G. , Miceli N. , Calapai G. , and Navarra M. , Cranberry and Recurrent Cystitis: More Than Marketing?, Critical Reviews in Food Science and Nutrition. (2014) 54, no. 8, 1063–1075, 10.1080/10408398.2011.625574, 2-s 2.0-84893625419.24499122 · doi ↗ · pubmed ↗
- 3Mc Lellan L. K. and Hunstad D. A. , Urinary Tract Infection: Pathogenesis and Outlook, Trends in Molecular Medicine. (2016) 22, no. 11, 946–957, 10.1016/j.molmed.2016.09.003, 2-s 2.0-84992734412.27692880 PMC 5159206 · doi ↗ · pubmed ↗
- 4Kot B. , Wicha J. , Grużewska A. , Piechota M. , Wolska K. , and Obrębska M. , Virulence Factors, Biofilm-Forming Ability, and Antimicrobial Resistance of Urinary Escherichia coli Strains Isolated From Hospitalized Patients, Turkish Journal of Medical Sciences. (2016) 46, 1908–1914, 10.3906/sag-1508-105, 2-s 2.0-85006699771.28081347 · doi ↗ · pubmed ↗
- 5Guglietta A. , Recurrent Urinary Tract Infections in Women: Risk Factors, Etiology, Pathogenesis and Prophylaxis, Future Microbiology. (2017) 12, no. 3, 239–246, 10.2217/fmb-2016-0145, 2-s 2.0-85014607485.28262045 · doi ↗ · pubmed ↗
- 6Simmering J. E. , Tang F. , Cavanaugh J. E. , Polgreen L. A. , and Polgreen P. M. , The Increase in Hospitalizations for Urinary Tract Infections and the Associated Costs in the United States, 1998–2011, Open Forum Infectious Diseases. (2017) 4, no. 1, 10.1093/ofid/ofw 281.PMC 541404628480273 · doi ↗ · pubmed ↗
- 7You L. , Qian W. , Yang Q. et al., ERG 11 Gene Mutations and MDR 1 Upregulation Confer Pan-Azole Resistance in Candida tropicalis Causing Disseminated Candidiasis in an Acute Lymphoblastic Leukemia Patient on Posaconazole Prophylaxis, Antimicrobial Agents and Chemotherapy. (2017) 61, no. 7, 10.1128/AAC.02496-16, 2-s 2.0-85021913077.PMC 548766328507109 · doi ↗ · pubmed ↗
- 8Terlizzi M. E. , Gribaudo G. , and Maffei M. E. , Uro Pathogenic Escherichia coli (UPEC) Infections: Virulence Factors, Bladder Responses, Antibiotic, and Non-Antibiotic Antimicrobial Strategies, Frontiers in Microbiology. (2017) 8, 10.3389/fmicb.2017.01566, 2-s 2.0-85027726949.PMC 555950228861072 · doi ↗ · pubmed ↗